What could be the reason for prolactin increased in body without pregnancy and also increase in testosterone??
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching the Web
causes of elevated prolactin and elevated testosterone at the same time
Finding Sources
Finding Sources
Now I have a comprehensive picture. Let me compile the full answer.
Causes of Elevated Prolactin (Without Pregnancy) + Elevated Testosterone
These two findings together narrow the differential significantly. Here is a structured breakdown:
Why Both Can Rise Together
Prolactin and testosterone are normally regulated in opposition - high prolactin tends to suppress testosterone via the HPG axis. So finding both elevated simultaneously points to specific conditions where independent mechanisms are driving each hormone up.
1. Polycystic Ovary Syndrome (PCOS) - Most Common in Women
PCOS is the leading reason to see elevated testosterone + mild hyperprolactinemia in the same patient. Approximately 30% of women with PCOS have elevated prolactin levels alongside hyperandrogenism (elevated testosterone, DHEAS).
- Mechanism: Insulin resistance and excess LH drive ovarian androgen (testosterone) overproduction. Elevated estrogens from peripheral aromatization can stimulate lactotroph cells in the pituitary, mildly raising prolactin.
- Note: Significantly elevated prolactin (>100 ng/mL) actually excludes PCOS by diagnostic criteria - it suggests another cause.
- Associated features: Oligomenorrhea/amenorrhea, hirsutism, acne, polycystic ovaries on ultrasound, LH:FSH ratio >3:1.
(Tietz Textbook of Laboratory Medicine, 7th Ed.; Swanson's Family Medicine Review)
2. Prolactinoma Co-existing with Adrenal/Ovarian Pathology
A pituitary prolactin-secreting adenoma (prolactinoma) can coexist with:
- Androgen-secreting adrenal or ovarian tumor - rare but possible, particularly in MEN1 (multiple endocrine neoplasia type 1)
- Congenital adrenal hyperplasia (CAH) - especially non-classical/late-onset CAH, which raises adrenal androgens (including testosterone precursors) independently
3. Medications
Several drugs raise prolactin AND can indirectly affect testosterone:
- Antipsychotics (risperidone, haloperidol, metoclopramide) - dopamine antagonists raise prolactin; chronic use can alter sex hormone balance
- Opioids - raise prolactin AND suppress testosterone
- Anabolic steroids / exogenous testosterone - aromatization to estradiol stimulates prolactin release from pituitary lactotrophs
4. Hypothyroidism
Primary hypothyroidism causes compensatory TRH elevation, and TRH is a potent prolactin-releasing factor. Concurrently, hypothyroidism reduces sex hormone-binding globulin (SHBG), which can raise free testosterone even when total testosterone is normal.
(Harrison's Principles of Internal Medicine 22E)
5. Congenital Adrenal Hyperplasia (CAH) - Non-Classical
- Adrenal enzyme deficiency (especially 21-hydroxylase) causes excess adrenal androgens including testosterone
- This elevated androgen milieu can feed back to stimulate mild prolactin elevation via estrogenic pathways
6. Chronic Stress / Physiologic Causes
- Stress, intense exercise, sleep deprivation, and chest wall stimulation all transiently raise prolactin
- In the same individual with underlying androgen excess (e.g., PCOS, CAH), this can produce a combined picture
Summary Table
| Cause | Prolactin | Testosterone | Notes |
|---|---|---|---|
| PCOS | Mildly ↑ | ↑ | Most common, insulin resistance driven |
| Non-classical CAH | Mild ↑ | ↑ (adrenal androgens) | 17-OHP elevated |
| Prolactinoma + adrenal/ovarian tumor | Markedly ↑ | ↑ | Rare, consider MEN1 |
| Opioid use | ↑ | Variable | Drug history |
| Exogenous testosterone / anabolic steroids | ↑ (via aromatization to estradiol) | ↑ | Performance drugs |
| Hypothyroidism | ↑ | Free T may ↑ (low SHBG) | TSH elevated |
| Idiopathic | ↑ | Normal/slightly ↑ | Diagnosis of exclusion |
Recommended Workup
When both are elevated, the standard evaluation includes:
- Repeat prolactin (fasting, non-stressed, morning sample) - rule out spurious elevation
- MRI pituitary - rule out prolactinoma or stalk compression
- TSH / free T4 - rule out hypothyroidism
- Free and total testosterone, DHEAS, 17-OHP - differentiate ovarian vs. adrenal source
- Pelvic ultrasound (in women) - look for polycystic ovaries
- Medication review - dopamine antagonists, opioids, estrogens
- LH, FSH - assess gonadotropin axis
- Renal and liver function - chronic kidney disease and cirrhosis both raise prolactin
The combination of both elevations in a woman of reproductive age should prompt evaluation for PCOS first, followed by pituitary imaging if prolactin is significantly elevated (>100 ng/mL) or the clinical picture doesn't fit PCOS.
(Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; Tietz Textbook of Laboratory Medicine 7th Ed.)
Okay so pcos it is? Why does that happen?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is the full picture of how and why PCOS happens:
Why Does PCOS Happen? - The Pathophysiology Explained
PCOS is not caused by a single event. It is a multi-compartment hormonal vicious cycle, starting with a genetic predisposition and triggered or worsened by environmental factors like diet and body weight.
Here is the official pathophysiology diagram from Berek & Novak's Gynecology:
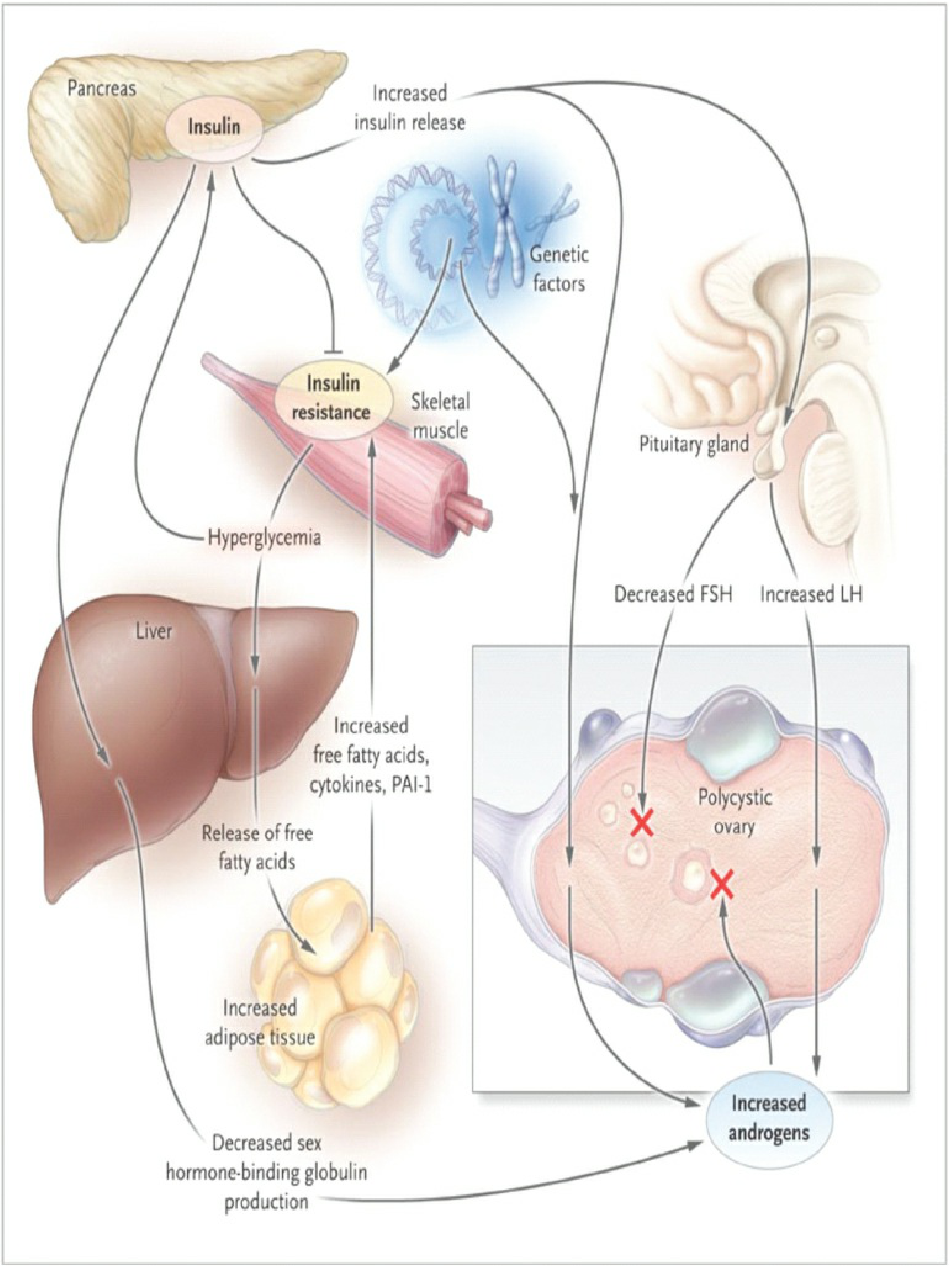
The Core Problem: Insulin Resistance
The central driver in most women with PCOS is insulin resistance (IR) - the body's cells (especially skeletal muscle) stop responding properly to insulin. The pancreas compensates by producing even more insulin (hyperinsulinemia).
This excess insulin then acts on two key places:
1. The Ovaries (Theca Cells)
- Insulin works together with LH (luteinizing hormone) to stimulate the theca cells of the ovary
- Theca cells overproduce androgens - primarily testosterone and androstenedione
- This is why testosterone goes up in PCOS
2. The Liver
- Excess insulin suppresses the liver's production of Sex Hormone-Binding Globulin (SHBG)
- SHBG is the protein that binds testosterone in the blood and keeps it inactive
- Less SHBG = more free, bioavailable testosterone circulating - making the androgen excess even worse
The Pituitary Disruption: LH/FSH Imbalance
Simultaneously, in the hypothalamus and pituitary:
- GnRH pulse frequency increases - the hypothalamus fires faster than normal
- This drives the pituitary to release more LH but not more FSH
- The result: elevated LH with low/normal FSH - classic LH:FSH ratio >2-3:1
- High LH further stimulates ovarian theca cells to make even more androgens - amplifying the cycle
Why doesn't FSH rise? Because the chronically elevated estrogen (from peripheral aromatization of androgens in fat tissue) and normal inhibin provide negative feedback that selectively suppresses FSH.
Why Eggs Don't Release (Anovulation)
- FSH is needed for follicles to fully mature and release an egg
- Without enough FSH, follicles start developing but get stuck - they don't rupture
- These stalled follicles accumulate under the ovarian surface as small cysts (the "polycystic" appearance on ultrasound)
- No ovulation = no progesterone = irregular or absent periods
Why Prolactin Gets Mildly Elevated in PCOS
About 25% of PCOS patients have mildly elevated prolactin. The mechanism:
- Chronically elevated estrogens (from peripheral aromatization of the excess androgens) provide abnormal feedback to the pituitary
- This stimulates lactotroph cells to release extra prolactin
- This is a secondary effect - prolactin is not the primary driver in PCOS
(Berek & Novak's Gynecology, p.1925)
The Vicious Cycle - All Connected
Genetic predisposition
↓
Insulin Resistance
↓
Hyperinsulinemia
↙ ↘
Theca cells ↓ SHBG (liver)
overproduce ↓
androgens More free testosterone
↓
Excess androgens → converted to estrogens in fat
↓
Abnormal pituitary feedback → ↑ LH, FSH stays low
↓
Follicles don't mature → no ovulation → more androgens
↓ ↑
Cysts form on ovary ─────────────────────────┘
What Triggers It in the First Place?
PCOS has a strong genetic component (polygenic - multiple genes involved, including insulin receptor genes, CYP17 androgen enzyme genes, and FSH receptor genes). However, it is triggered and made worse by:
| Trigger | How it worsens PCOS |
|---|---|
| Obesity | Fat tissue worsens insulin resistance and increases aromatization |
| Puberty | Adrenal androgen surge (adrenarche) may initiate the cycle |
| Sedentary lifestyle | Worsens insulin resistance in skeletal muscle |
| High carbohydrate diet | Drives hyperinsulinemia |
Bottom Line
PCOS is essentially a genetic tendency toward insulin resistance, which spirals into a self-reinforcing loop of high insulin → high androgens (testosterone) → disrupted pituitary signaling → failed ovulation → more androgens. The mildly elevated prolactin is a downstream effect of all the excess estrogen, not the root cause.
(Berek & Novak's Gynecology; Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E)
This is a shared conversation. Sign in to Orris to start your own chat.