Rinnes test
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a complete overview of Rinne's test from authoritative ENT textbooks:
Rinne's Test
Purpose
Rinne's test compares air conduction (AC) versus bone conduction (BC) in the same ear to determine whether a conductive component (air-bone gap) is present. It does not localize the side of hearing loss - that is the role of the Weber test.
Tuning Fork Selection
The preferred fork is 512 Hz. Some clinicians use 256 Hz, which actually gives superior sensitivity and specificity for detecting conductive defects (see chart below). Forks of 1024 Hz and higher are less appropriate as they decay too quickly.
Technique
Method 1 - Loudness Comparison (Preferred)
- Strike the tuning fork and place it firmly on the flat mastoid bone behind the pinna (bone conduction).
- Then hold it approximately 2 cm (or ~2 inches) lateral to the external auditory meatus (air conduction).
- Ask the patient: "Which sounds louder - position 1 or position 2?"
This is the more reliable method.
Method 2 - Threshold Comparison (Less Reliable)
- Hold the activated fork at the ear canal until the patient can no longer hear it.
- Immediately place it on the mastoid.
- If the patient hears it again, BC > AC (negative Rinne = conductive loss).
This method is less reliable and not recommended over the loudness comparison method.
Interpretation
| Result | Finding | Meaning |
|---|---|---|
| AC > BC (Positive Rinne) | Sound louder at ear canal | Normal hearing OR sensorineural hearing loss |
| BC > AC (Negative Rinne) | Sound louder on mastoid | Conductive hearing loss (~20 dB or greater air-bone gap) |
| AC = BC | Equal loudness | Borderline / uninterpretable (occurs in up to 10% of patients with 11-40 dB air-bone gap) |
Note: The positive/negative Rinne terminology is a frequent source of confusion because a positive result is actually normal. Some authors prefer simply documenting "AC > BC" or "BC > AC."
Sensitivity & Specificity
The 256 Hz fork using the loudness comparison method outperforms the 512 Hz threshold method:
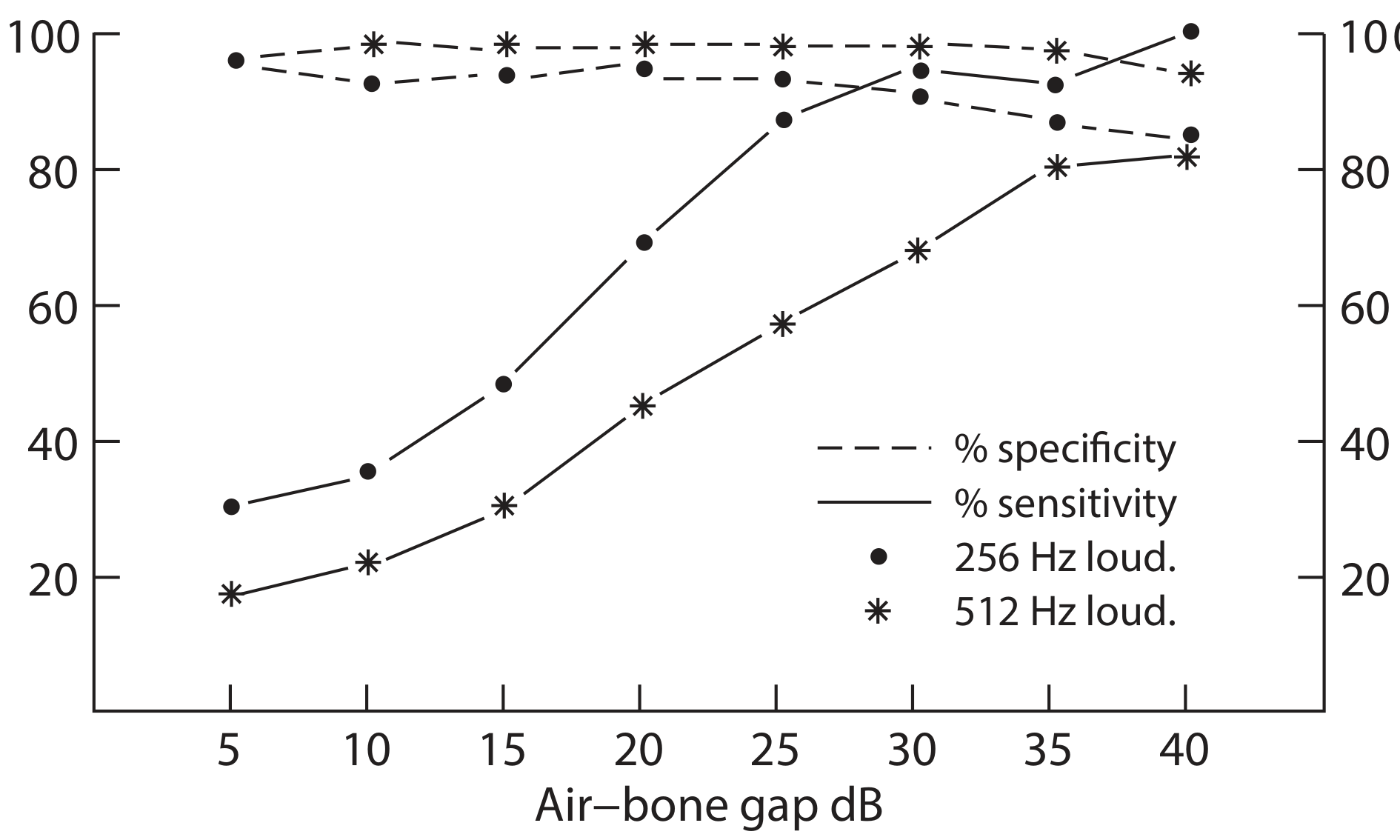
Key thresholds for the 256 Hz fork (loudness comparison):
- Detects conductive defect >30 dB in 90% of patients
- Sensitivity falls to ~70% for 20-30 dB gaps
- Sensitivity drops below 50% for 10-20 dB gaps
- False-positive rate in normal patients: ~20%
With a 512 Hz fork, BC > AC suggests a conductive loss of 20 dB or worse.
Table: Rinne result vs. air-bone gap (512 Hz, loudness comparison)
| Air-bone gap (dB) | AC > BC | AC = BC | BC > AC |
|---|---|---|---|
| 0-10 | 97% | 1% | 2% |
| 10-20 | 61% | 11% | 19% |
| 21-30 | 32% | 8% | 60% |
| 31-40 | 42% | 8% | 49% |
| >40 | 10% | 0% | 90% |
False-Positive Rinne ("False Negative")
A false-positive Rinne (BC appears > AC but is actually being heard by the opposite, better ear via transcranial bone conduction) occurs in cases of dead ear / profound ipsilateral SNHL. The bone conduction sound crosses to the contralateral cochlea. To avoid this error:
- Masking of the non-test ear with a Barany box or narrow-band masker is required when testing a poorer-hearing ear.
Combined Interpretation with Weber Test
| Weber Lateralizes To | Rinne in Both Ears | Diagnosis |
|---|---|---|
| Left | Positive bilateral (AC > BC) | SNHL right ear (or mild CHL left) |
| Right | Positive bilateral (AC > BC) | SNHL left ear (or mild CHL right) |
| Left | Negative left (BC > AC) | CHL left ear |
| Right | Negative right (BC > AC) | CHL right ear |
| Left | Negative right | Mixed HL right / CHL left |
Comparison with Other Tuning Fork Tests
| Test | Purpose | Normal | Conductive Loss | SNHL |
|---|---|---|---|---|
| Rinne | AC vs BC comparison | AC > BC (positive) | BC > AC (negative) | AC > BC (positive) |
| Weber | Lateralization | Midline | Lateralizes to affected (poorer) ear | Lateralizes to better ear |
| Bing | Occlusion effect | Positive (louder when canal occluded) | Negative (no change) | Positive |
| Schwabach | BC vs. examiner's BC | Normal duration | Prolonged | Diminished |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2, Ch. 73
- Shambaugh Surgery of the Ear, pp. 205-206
- Cummings Otolaryngology Head and Neck Surgery, Table 137.6
- K.J. Lee's Essential Otolaryngology, pp. 293-294
Webers test
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Here is a complete account of Weber's test from authoritative ENT and neurology textbooks:
Weber's Test
Purpose
Weber's test is a test of lateralization - it identifies which ear perceives a midline bone-conducted sound as louder. It is used to distinguish between conductive and sensorineural hearing loss, and to identify which ear is affected in unilateral or asymmetric loss. It is not useful if hearing is symmetric in both ears (the sound will simply be midline).
Tuning Fork
512 Hz is standard. The fork must be struck on a soft surface (e.g., the heel of the hand or a rubber pad) - never a hard surface, which creates high-frequency overtones that complicate interpretation.
Technique
- Strike the tuning fork and place its stem firmly on the midline of the skull - any of these positions work:
- Centre of the forehead (most common)
- Bridge of the nose
- Central incisor teeth (with teeth tightly clenched)
- Vertex of the skull
- Mandibular symphysis
- Ask the patient: "In which ear is the sound louder, or is it equal in both?"
Interpretation
| Patient Response | Meaning |
|---|---|
| Midline / equal in both ears | Normal hearing, or symmetrical hearing loss in both ears |
| Lateralizes to the poorer ear | Unilateral conductive hearing loss on that side |
| Lateralizes to the better ear | Unilateral sensorineural hearing loss on the opposite side |
Why does it lateralize in conductive loss?
In a conductive hearing loss, the affected ear has less background environmental noise reaching the cochlea via air conduction. This relative "quietness" makes the bone-conducted signal from the tuning fork stand out as louder in the affected ear. Additionally, the masking effect of ambient noise is reduced on the side of the conductive loss.
Why does it lateralize to the better ear in SNHL?
In sensorineural hearing loss, the damaged cochlea perceives the bone-conducted signal more poorly. The intact cochlea on the other side receives the signal more clearly, so sound appears louder there.
Important: A Weber's test is described as "Weber right" or "Weber left" when it lateralizes, and "negative" when it is midline. The term "negative Weber" = normal (no lateralization).
Limitations and Accuracy
Scott-Brown's is notably candid about this:
"The Weber test has a low sensitivity and specificity and is marginally better than chance. The chance of accurately and reliably identifying conductive and sensorineural deafness is only 33%."
- It requires unilateral or asymmetric hearing loss to be interpretable
- Patients with unilateral conductive loss are sometimes reluctant to acknowledge hearing it louder in the "bad" ear
- The acoustic basis for why it lateralizes is still not fully understood
- With a 512 Hz fork, even a conductive loss of only 3-5 dB can cause lateralization
Combined Weber + Rinne Interpretation
This table summarizes the full picture when both tests are used together:
| Weber Lateralizes To | Rinne (Both Ears) | Diagnosis |
|---|---|---|
| Midline | AC > BC bilaterally | Normal hearing |
| Right | AC > BC bilaterally | Left SNHL (or mild right CHL) |
| Left | AC > BC bilaterally | Right SNHL (or mild left CHL) |
| Right | BC > AC right | Right CHL |
| Left | BC > AC left | Left CHL |
| Right | BC > AC left | Mixed HL left / Right CHL |
Clinical examples:
- Right conductive hearing loss: Weber lateralizes RIGHT; Rinne on the right is BC > AC (negative)
- Right sensorineural loss: Weber lateralizes LEFT; Rinne is AC > BC bilaterally (both positive)
Role in Clinical Practice
Tuning fork tests, including Weber's, are particularly valuable:
- When a formal audiogram is not available
- To confirm audiometric findings before surgery (especially stapedectomy)
- In the emergency or bedside setting to quickly characterize sudden hearing loss
- In cases of a masking dilemma on formal audiometry
However, pure-tone audiometry with masked bone conduction remains the definitive method for characterizing hearing loss - tuning fork tests are screening and confirmatory tools.
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2, Ch. 73
- Shambaugh Surgery of the Ear, pp. 205
- Cummings Otolaryngology Head and Neck Surgery, Table 4.3
- K.J. Lee's Essential Otolaryngology, Table 14-5
- Swanson's Family Medicine Review, Ch. 3
Schwabath test
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Excellent sources retrieved. Here is the full overview:
Schwabach's Test
Purpose
Schwabach's test compares the bone conduction (BC) of the patient with the bone conduction of a normal-hearing examiner. It is used to determine whether the patient's BC is normal, reduced, or prolonged relative to a healthy standard. It is not commonly performed in routine clinical practice but is a useful bedside test when an audiogram is unavailable.
Prerequisite: The examiner must have confirmed normal hearing to serve as a valid reference standard.
Tuning Fork
512 Hz is standard, though some sources permit 256 Hz.
Technique
- Strike the tuning fork on a soft surface.
- Place the stem firmly on the patient's mastoid process.
- When the patient signals they can no longer hear the tone, immediately transfer the fork to the examiner's mastoid.
- The examiner then reports whether the tone is still audible to them.
- The fork may also be alternated back and forth between patient and examiner to compare duration.
Interpretation
| Result | Finding | Meaning |
|---|---|---|
| Normal Schwabach | Patient and examiner stop hearing at approximately the same time | Normal hearing (BC equal to examiner's) |
| Diminished Schwabach | Patient stops hearing before the examiner | Sensorineural hearing loss - cochlear or nerve damage reduces BC thresholds |
| Prolonged Schwabach | Patient hears longer than the examiner | Conductive hearing loss - the conductive defect blocks ambient masking noise, so the bone-conducted signal appears relatively louder and lasts longer |
Physiological Basis
The key to understanding the Schwabach test lies in the masking effect of environmental noise:
- In a normal ear, ambient background noise constantly enters via air conduction and partially masks (competes with) bone-conducted signals.
- In conductive hearing loss, the middle ear blockage prevents this ambient noise from reaching the cochlea. Without this competing noise, the bone-conducted tuning fork signal stands out more, giving the patient an apparent advantage - BC sounds louder and lasts longer.
- In sensorineural hearing loss, the damaged cochlear hair cells or auditory nerve reduce all sound perception, including bone-conducted sound, so BC is diminished.
As Ganong's Review of Medical Physiology states: "The Weber and Schwabach tests demonstrate the important masking effect of environmental noise on the auditory threshold."
Summary Table: All Three Classic Tuning Fork Tests
(from Ganong's Review of Medical Physiology, Table 11-1)
| Weber | Rinne | Schwabach | |
|---|---|---|---|
| Method | Fork on vertex of skull | Fork on mastoid, then held by ear canal | Patient BC compared with examiner's BC |
| Normal | Equal in both ears | AC > BC (positive) | Patient and examiner hear equally long |
| Conductive loss (one ear) | Louder in affected ear (ambient masking absent) | BC > AC (negative Rinne) | Prolonged (BC better than normal - masking removed) |
| Sensorineural loss (one ear) | Louder in normal ear | AC > BC (positive Rinne, but both reduced) | Diminished (BC worse than normal) |
Comparison with Rinne
Both tests assess bone conduction, but differently:
| Feature | Rinne | Schwabach |
|---|---|---|
| Comparison made | AC vs BC in the same patient | Patient's BC vs examiner's normal BC |
| Absolute vs relative | Relative (within patient) | Absolute (against a normal standard) |
| Detects | Air-bone gap (conductive component) | Whether BC itself is normal, reduced, or enhanced |
Clinical Significance
- A diminished Schwabach + positive Rinne = sensorineural hearing loss
- A prolonged Schwabach + negative Rinne = conductive hearing loss
- Useful in confirming audiometric findings before surgical intervention (e.g., stapedectomy)
- In early sensorineural deafness, high-pitched sounds are lost first; in conductive deafness, low-pitched sounds are lost first - tuning forks of different frequencies can help map this loss
Sources:
- K.J. Lee's Essential Otolaryngology, pp. 293-294
- Ganong's Review of Medical Physiology, 26th ed., Table 11-1
- Adams and Victor's Principles of Neurology, 12th ed., Ch. 4
Nystagmus test in vestibular component
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Now I have comprehensive data for a complete answer. Here it is:
Nystagmus Tests in Vestibular Assessment
What is Vestibular Nystagmus?
Nystagmus is an involuntary rhythmic eye movement consisting of:
- Slow phase - a drift of the eyes driven by the vestibular system (toward the damaged side)
- Fast phase (quick phase) - a rapid saccadic corrective jerk in the opposite direction that resets eye position
By convention, the direction of nystagmus is named after the fast phase. The underlying vestibular drive is the slow phase.
Physiological basis: The vestibular nuclei on each side tonically drive the eyes in opposite horizontal directions. When this balance is disrupted - by disease, temperature change, or movement - the eyes drift, triggering a corrective fast phase, producing nystagmus.
Types of Vestibular Nystagmus
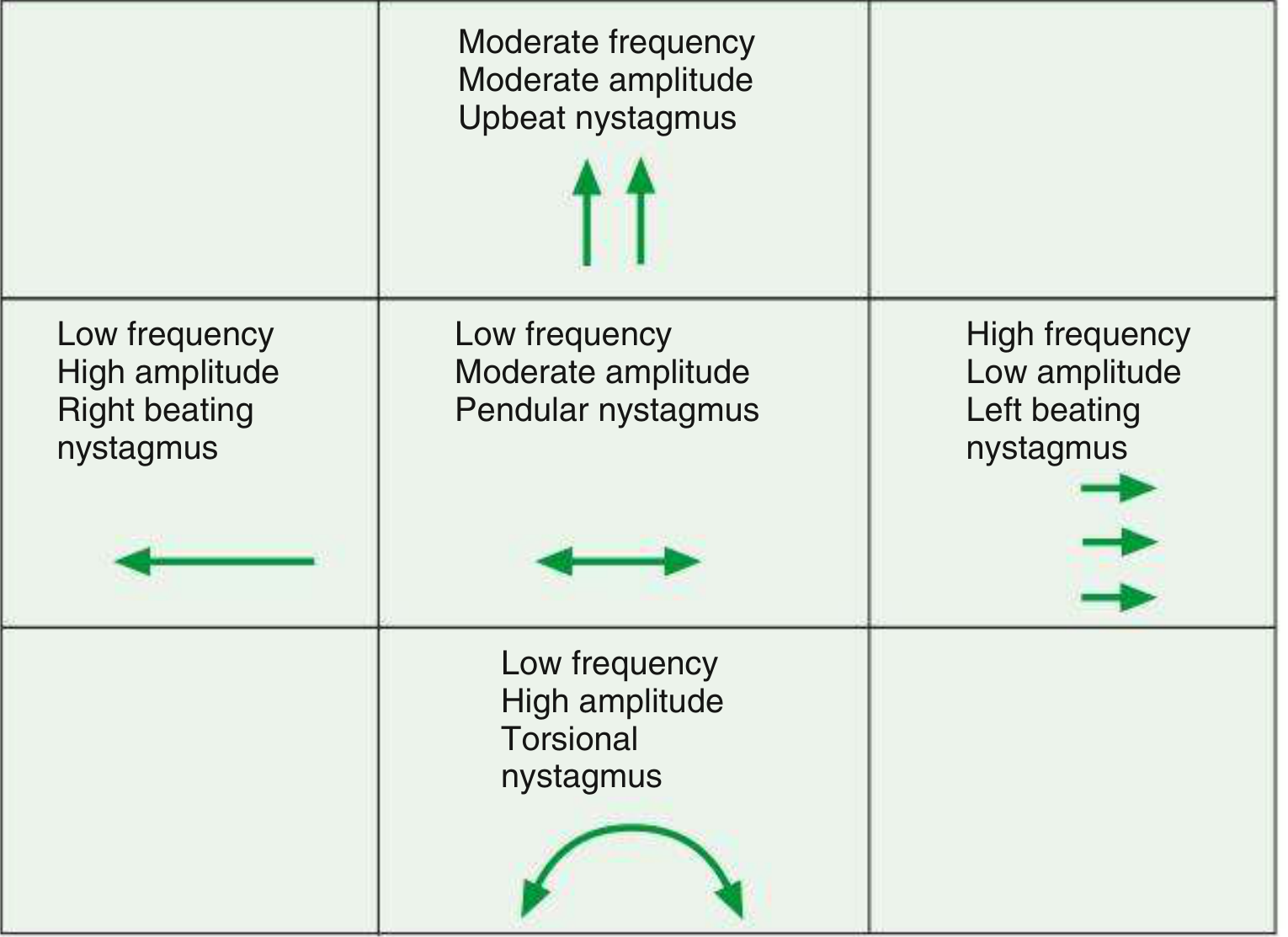
(Fig. 19.88 from Kanski's Clinical Ophthalmology - schematic for documenting nystagmus types)
Peripheral vs Central Vestibular Nystagmus
The two key distinguishing features between peripheral and central nystagmus are:
| Feature | Peripheral Vestibular | Central Vestibular |
|---|---|---|
| Direction | Unidirectional (horizontal or horizontal-torsional) | May change direction with gaze (direction-changing) |
| Fixation | Suppressed by visual fixation | NOT suppressed by fixation |
| Associated symptoms | Vertigo, tinnitus, hearing loss | Diplopia, dysarthria, limb ataxia, other CNS signs |
| Slow phase | Linear (constant velocity) | May be variable |
| Pure vertical/torsional | Rare - suggests superior/inferior nerve involvement | Pure vertical or pure torsional = central sign |
| Alexander's law | Obeyed - fast phase intensifies on gaze toward fast phase | May not obey |
| Onset with positional change | Latency present, fatigable | Immediate, non-fatigable |
Characteristics of peripheral vestibular nystagmus (Box 66.2, Scott-Brown's):
- Unidirectional
- Horizontal
- Conjugate
- Temporary
- Enhanced by removal of optic fixation
- Obeys Alexander's law
Key clinical pearl (Harrison's): "Nystagmus from an acute peripheral lesion is unidirectional, with fast phases beating away from the ear with the lesion. Nystagmus that changes direction with gaze is due to a central lesion."
"If nystagmus is easily seen in the light, it is probably due to a central cause."
Tools to Enhance Nystagmus Detection
- Frenzel glasses (self-illuminated goggles, +20-30 diopter lenses) - blur vision, prevent fixation suppression, magnify eyes for examiner
- Infrared video goggles / VNG goggles - same principle, with electronic recording
- Ophthalmoscope method - patient fixes with one eye, examiner observes the opposite optic disc for slow drift; covering the fixating eye accentuates nystagmus
Spontaneous nystagmus may subside with fixation within 1-2 weeks of onset, but with Frenzel glasses it may still be detected for 5-10 years after an acute vestibular event.
Key Bedside Tests for Vestibular Nystagmus
1. Observation for Spontaneous Nystagmus
- Patient sits still and fixates on a distant target
- Inspect gaze in primary position, 30° left, and 30° right (do not exceed 30° as this produces physiological end-point nystagmus)
- Repeat with Frenzel lenses to remove fixation suppression
- Note direction, plane, and whether it changes with gaze direction
2. Dix-Hallpike Maneuver (Hallpike Test / Nylen-Barany Maneuver)
Indication: All patients with positional vertigo; standard test for BPPV of the posterior semicircular canal.
Technique:
- Patient sits on a table capable of reclining flat, positioned so the head will extend beyond the edge when supine.
- Head turned 45° toward the suspected ear.
- Patient is rapidly lowered to supine with the head hanging ~20° below horizontal (over the table edge).
- Watch the eyes for nystagmus (ideally with Frenzel lenses). Note:
- Latency before onset
- Direction and plane
- Duration
- Whether it fatigues on repeat testing
- Return patient to sitting - may provoke dizziness again.
- Repeat with head turned to the other side.
Result: The abnormal ear is the one placed "down" when nystagmus and vertigo are provoked.
Positive result for posterior canal BPPV:
- Transient upbeating-torsional nystagmus
- Latency of 1-5 seconds
- Lasts < 30-60 seconds
- Fatigues on repeat testing
Pure vertical or pure torsional nystagmus without latency or fatigue = central lesion.
3. Head Impulse Test (Head Thrust Test / Halmagyi Test)
The most useful bedside test of peripheral vestibular function (Harrison's).
Technique:
- Patient fixates on examiner's nose.
- Examiner delivers a small, brisk (~15-20°) rapid head rotation horizontally to one side.
- Observe for catch-up saccades.
Interpretation:
- Normal VOR: Eyes remain fixed on target despite head movement. No corrective saccade.
- Abnormal VOR (peripheral lesion): Eyes are dragged with the head, then a catch-up saccade occurs back toward the target. The corrective saccade direction indicates the side of the vestibular lesion (e.g., leftward catch-up saccade = right head turn = left labyrinthine weakness).
- Bilateral lesions: Abnormal in both directions.
Critical point (Harrison's): "Absence of a head impulse sign in a patient with acute prolonged vertigo should suggest a central cause." (e.g., posterior fossa stroke can mimic vestibular neuritis but the head impulse is typically normal in central lesions.)
4. Head-Shaking Nystagmus (HSN) Test
Technique:
- Patient wears Frenzel lenses.
- Head tilted chin-down 30° to bring horizontal canals into horizontal plane.
- Head shaken vigorously side to side for ~10 seconds.
- Observe immediately for nystagmus when shaking stops.
Interpretation:
- Normal: No nystagmus, or only a few beats.
- Unilateral peripheral loss: Nystagmus with fast phase initially toward the uninvolved (stronger) side, which may then reverse toward the dysfunctional labyrinth (recovery nystagmus).
- Central lesion: May produce nystagmus in a plane different from the plane of head shaking (cross-coupling).
5. Caloric Test (Fitzgerald-Hallpike Caloric Test)
The only test that assesses each labyrinth independently.
Patient position: Supine, head tilted 30° forward - this brings the horizontal semicircular canal into the vertical plane, maximizing the convection effect.
Stimuli:
- Water: 30°C (cold) and 44°C (warm), each for 30 seconds, with ≥5 minutes between irrigations
- Air: 24°C (cold) and 58°C (warm), each for 60 seconds (used when tympanic membrane is perforated)
Mechanism: Temperature changes create a density gradient in the endolymph → convection currents → cupular deflection → nystagmus.
Mnemonic: COWS - Cold Opposite, Warm Same
| Stimulus | Effect | Nystagmus direction |
|---|---|---|
| Cold water - right ear | Endolymph falls (ampullofugal) | Fast phase beats LEFT |
| Warm water - right ear | Endolymph rises (ampullopetal) | Fast phase beats RIGHT |
| Cold water - both ears | Bilateral ampullofugal | Fast phase beats UPWARD |
| Warm water - both ears | Bilateral ampullopetal | Fast phase beats DOWNWARD |
Abnormal caloric responses:
| Abnormality | Finding | Cause |
|---|---|---|
| Bilateral canal paresis | No response to any irrigation | Aminoglycoside ototoxicity, post-meningitis bilateral labyrinthitis |
| Unilateral canal paresis | Reduced/absent response one ear | Vestibular schwannoma, vestibular neuritis |
| Directional preponderance (DP) | Asymmetry in VOR strength (one direction beats stronger) | Various - labyrinth to cortex |
| In a comatose patient | Only slow tonic deviation toward stimulated side (no fast phase) | Brainstem intact but arousal/saccade generation lost |
>20% asymmetry in nystagmus duration or slow-phase velocity between the two ears is considered significant.
6. Nystagmography (ENG / VNG)
Electronystagmography (ENG) records eye movements using skin electrodes (corneoretinal potential); Videonystagmography (VNG) uses infrared cameras in goggles.
A standard battery includes:
- Tests of visual ocular control - saccades, smooth pursuit, optokinetic nystagmus
- Search for spontaneous nystagmus (with and without fixation)
- Positional testing (Dix-Hallpike and supine roll test)
- Caloric testing (induced vestibular nystagmus)
Summary: Peripheral vs Central - Quick Reference
| Peripheral | Central | |
|---|---|---|
| Direction | Fixed, unidirectional | Direction-changing with gaze |
| Plane | Horizontal or horizontal-torsional | May be pure vertical or torsional |
| Fixation suppression | Yes | No |
| Head impulse test | Abnormal (catch-up saccade) | Usually normal |
| Hearing/tinnitus | Often present | Usually absent |
| Associated neuro signs | Absent | Present (diplopia, dysarthria, ataxia) |
| Dix-Hallpike | Fatigable, latency present | Non-fatigable, no latency |
| Urgency | Less urgent (usually benign) | Urgent - possible stroke |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2, Ch. 62, 66
- Harrison's Principles of Internal Medicine, 22nd ed., Ch. 24
- Localization in Clinical Neurology, 8th ed., Ch. 3
- Goldman-Cecil Medicine, Ch. 392/396
- Kanski's Clinical Ophthalmology, 10th ed., Ch. 19
- Shambaugh Surgery of the Ear, Ch. 9
This is a shared conversation. Sign in to Orris to start your own chat.