Functions of cerebellum physiology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive content from both Guyton & Hall and Kandel's Principles of Neural Science. Let me compile the full answer.
Functions of the Cerebellum - Physiology
The cerebellum is called a "silent area" of the brain because its electrical excitation produces no conscious sensation and rarely triggers voluntary movement. Yet its removal causes profound motor incoordination. It functions not by directly causing muscle contractions but by sequencing, monitoring, and correctively adjusting ongoing motor activities.
- Guyton and Hall Textbook of Medical Physiology, p. 699
Overview: How the Cerebellum Works
The cerebellum operates as a comparator and predictor:
- It receives the intended motor command (efference copy / corollary discharge) from the cerebral motor cortex
- It receives real-time sensory feedback from the periphery (proprioception, vestibular input, etc.)
- It compares intended vs. actual movement, then sends instantaneous subconscious corrective signals back into the motor system
- It also predicts the next sequential movement a fraction of a second in advance while the current one is still executing, enabling smooth, flowing motion
This comparison-and-correction loop is the foundation of all cerebellar motor function.
Three Functional Divisions (Longitudinal Organization)
| Division | Anatomical Region | Primary Function |
|---|---|---|
| Vestibulocerebellum | Flocculonodular lobe + adjacent vermis | Equilibrium and postural control |
| Spinocerebellum | Vermis + intermediate zones | Coordination of limb and distal extremity movements |
| Cerebrocerebellum | Lateral hemispheres | Planning and timing of sequential voluntary movements ("motor imagery") |
1. Vestibulocerebellum - Equilibrium and Balance
The flocculonodular lobe, the phylogenetically oldest part of the cerebellum, developed alongside the vestibular apparatus. It:
- Controls balance between agonist and antagonist muscles of the spine, hips, and shoulders during rapid changes in body position
- Predicts in advance the body's equilibrium state, compensating for the neural transmission delay (sensory signals from the periphery take many milliseconds to reach the brain - too slow for real-time correction alone)
- Works closely with the vestibular nuclei and spinal cord
Damage causes pronounced equilibrium disturbance, especially during rapid movements or changes in direction.
- Guyton and Hall, p. 705-706
2. Spinocerebellum - Coordination of Limb Movements
The vermis and intermediate zones receive somatotopic projections from the entire body surface. The vermis controls axial and proximal muscle movements; intermediate zones control the distal limbs, hands, and fingers.
Key functions:
- Coordination of distal extremities during purposeful movements
- Sends corrective output back to the cerebral motor cortex, red nucleus, and reticular formation via thalamo-cortical loops
- Processes continuous proprioceptive and cutaneous sensory feedback during movement execution
3. Cerebrocerebellum - Motor Planning and Sequential Movement
The large lateral hemispheres receive input almost exclusively from the premotor and somatosensory cortices and project back via the dentate nucleus and thalamus.
Functions:
-
Plans sequential voluntary movements up to tenths of a second in advance - this is "motor imagery"
-
Coordinates rapid sequential activities (typing, piano playing, running, talking)
-
Operates in a feedforward mode (acts before sensory feedback arrives)
-
Guyton and Hall, p. 705
-
Kandel's Principles of Neural Science, p. 956
Key Specific Functions
Damping and Prevention of Overshoot
A critical cerebellar function is preventing oscillation and overshooting. When a rapid movement is initiated:
- Deep cerebellar nuclei first send an excitatory signal to enhance the movement
- A few milliseconds later, Purkinje cell inhibitory signals arrive as a "delay-line negative feedback"
- This damps the movement precisely at the intended endpoint
Without this, movements overshoot and oscillate - seen clinically as intention tremor.
Timing Control
The cerebellum provides precise timing for coordinated multi-joint movements. It integrates sensory inputs with corollary discharge (copy of motor command) to determine when to initiate each phase of a movement.
- Kandel, p. 956
Motor Learning and Adaptation
The cerebellum learns from errors. Via the climbing fiber - Purkinje cell circuit:
- Climbing fibers (from the inferior olivary nucleus) carry error signals to Purkinje cells
- When a movement falls short of or overshoots the intended target, climbing fiber activity alters the long-term synaptic sensitivity of Purkinje cells to parallel fiber (granule cell) input
- Over repeated trials, cerebellar circuitry refines the timing and force of movements toward perfection
- Once learning is complete, climbing fiber error signals are no longer needed
This is the cellular basis of motor skill learning (e.g., learning to ride a bicycle, play a musical instrument).
- Guyton and Hall, p. 704-705
- Kandel, p. 956-957
Neuronal Circuit Summary
The basic cerebellar circuit involves:
| Cell Type | Role |
|---|---|
| Mossy fibers | Main afferent input (from cortex, spinal cord, brainstem); synapse on granule cells |
| Climbing fibers | From inferior olive; carry error signals; cause "complex spikes" in Purkinje cells |
| Granule cells | Excite Purkinje cells via parallel fibers; 500-1000 per Purkinje cell |
| Purkinje cells | Sole output of cerebellar cortex; fire 50-100 Hz; inhibitory on deep nuclei |
| Deep cerebellar nuclei | (Dentate, interposed, fastigial) - final output to thalamus, brainstem; fire tonically |
The balance of mossy/climbing fiber excitation vs. Purkinje cell inhibition on the deep nuclei is what allows fine-tuned modulation of motor output.
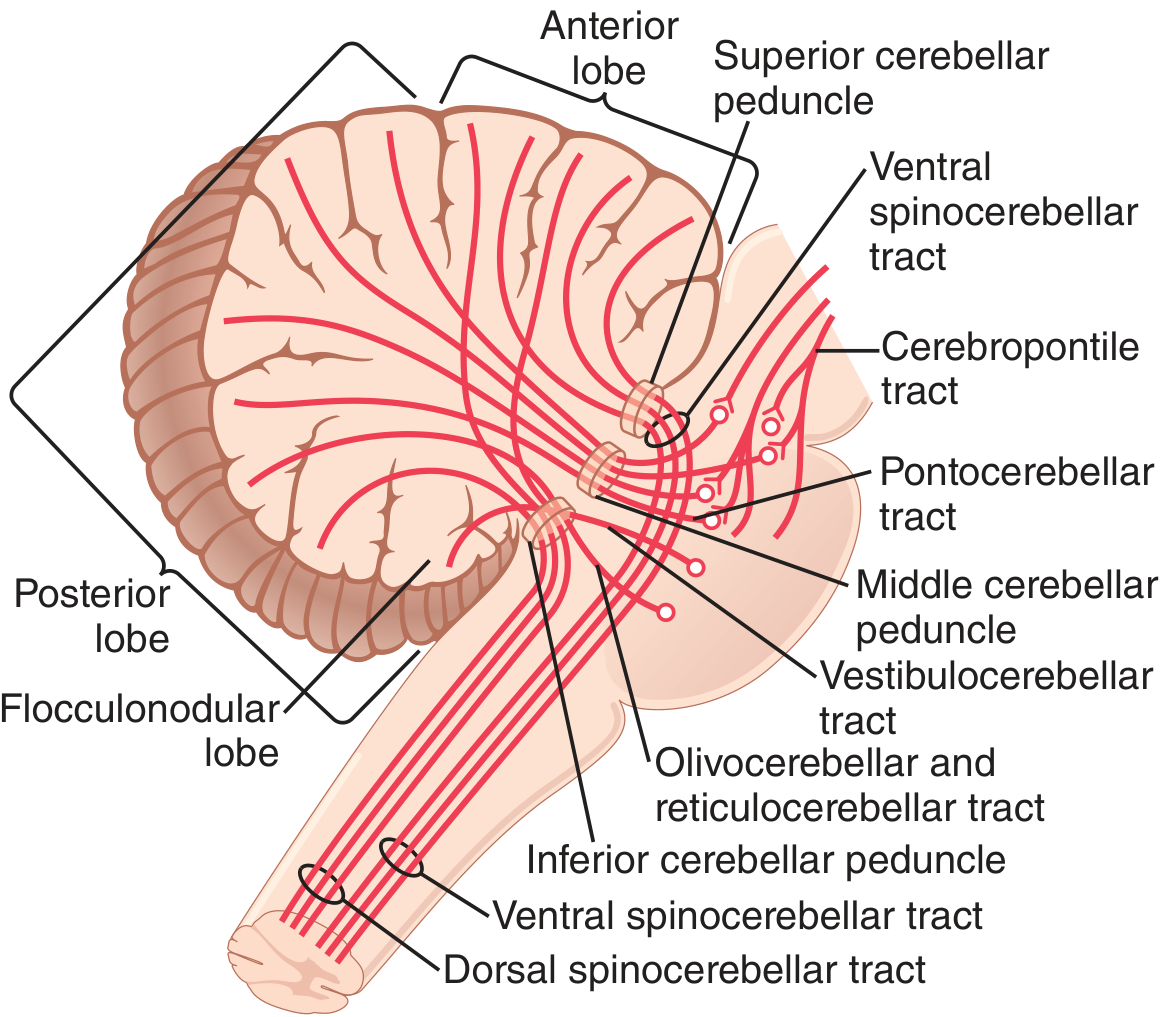
Principal afferent tracts to the cerebellum (Guyton & Hall, Fig. 57.4)
Non-Motor Functions (Cerebellar Cognitive Affective Syndrome)
Beyond motor control, there is growing evidence the cerebellum contributes to:
- Language processing
- Working memory
- Emotional regulation
- Abstract reasoning
Damage to the cerebellar posterior lobe produces Schmahmann syndrome (Cerebellar Cognitive Affective Syndrome) - diminished abstract reasoning, impaired emotional control, and sometimes autism/schizophrenia-spectrum features.
- Guyton and Hall, p. 710
- Kandel, p. 956
Clinical Signs of Cerebellar Dysfunction
| Sign | Mechanism |
|---|---|
| Dysmetria | Loss of movement prediction - movements overshoot the target |
| Past pointing | Same as dysmetria; inability to stop movement at intended endpoint |
| Intention tremor | Oscillation due to failure of damping |
| Dysdiadochokinesia | Failure of rapid alternating movements (e.g., pronation/supination) |
| Dysarthria | Failure of sequential coordination of laryngeal/oral muscles |
| Ataxic gait | Loss of coordinated postural and limb control |
| Hypotonia | Reduced tonic output from deep cerebellar nuclei to motor system |
- Guyton and Hall, p. 707-709
Summary: The cerebellum is a subconscious motor coordinator. Its three functional divisions handle equilibrium (vestibulocerebellum), limb coordination (spinocerebellum), and motor planning/learning (cerebrocerebellum). Its core mechanism is comparing intended vs. actual movement, damping overshoots, and refining motor programs through climbing-fiber-driven plasticity at Purkinje cell synapses.
Basal ganglia and it's disorders
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Excellent - I now have comprehensive content from four major textbooks. Let me compile the full answer.
Basal Ganglia: Physiology and Disorders
Anatomy: Components of the Basal Ganglia
On each side of the brain, the basal ganglia consist of four major components:
- Striatum - the main input nucleus, comprising:
- Caudate nucleus - receives mainly cortical association/prefrontal inputs; involved in cognitive control of motor sequences
- Putamen - receives mainly motor and somatosensory cortical inputs; involved in execution of learned motor patterns
- Globus pallidus - divided into internal (GPi) and external (GPe) segments; GPi is the main output nucleus
- Substantia nigra - pars compacta (SNc) sends dopamine to striatum; pars reticulata (SNr) is also an output nucleus
- Subthalamic nucleus (STN) - key node of the indirect pathway
The internal capsule - carrying almost all corticospinal and sensory fibers - passes between the caudate and putamen.
- Guyton and Hall Textbook of Medical Physiology, p. 709
Functions of the Basal Ganglia
1. Putamen Circuit - Execution of Learned Motor Patterns
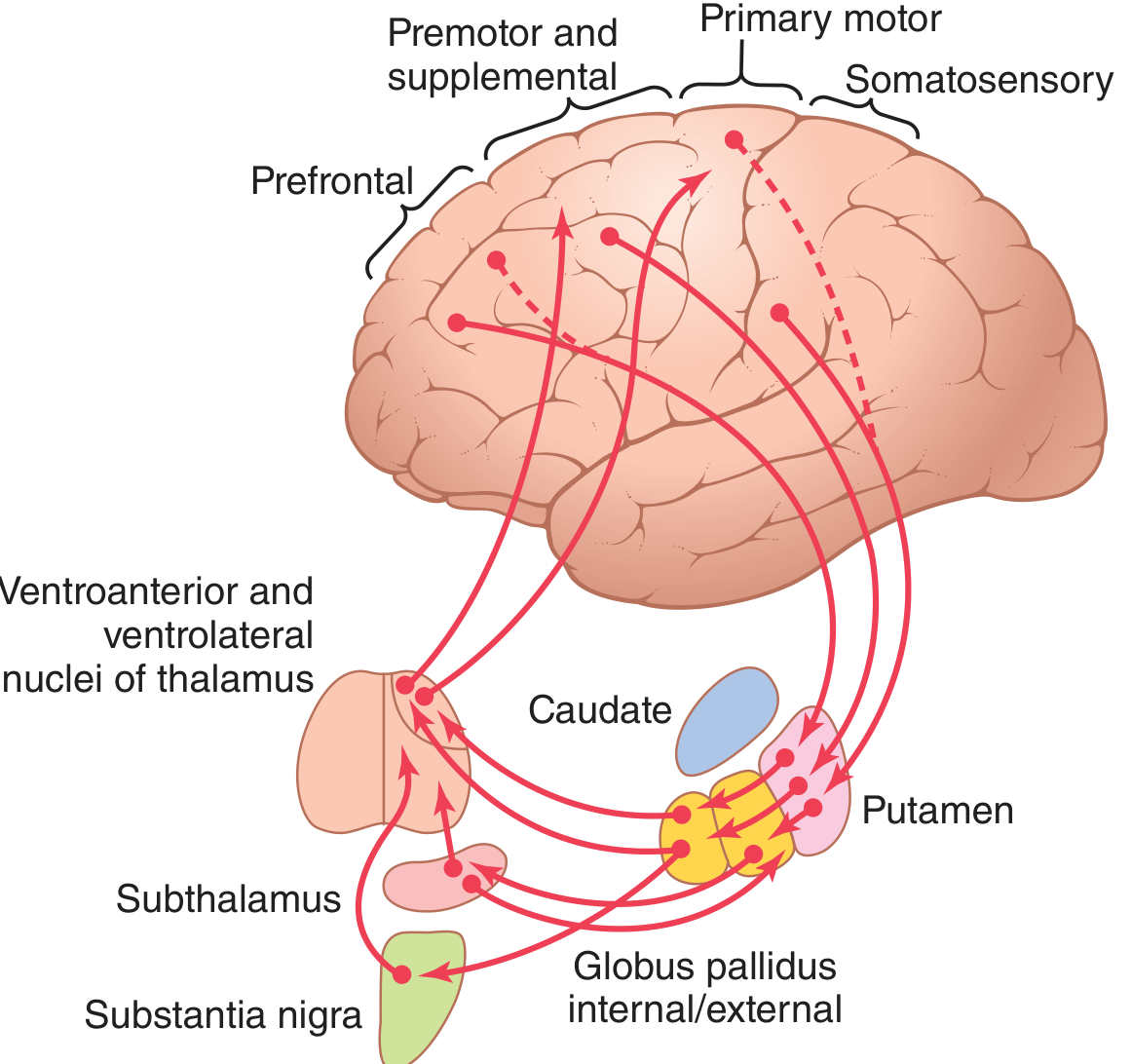
The putamen circuit controls subconscious execution of learned, complex motor patterns - writing letters, cutting with scissors, hammering nails, throwing a ball, vocalization, and eye movements. The pathway is:
Premotor & SMA cortex → Putamen → GPi/SNr → Ventroanteroior & Ventrolateral thalamus → Primary motor cortex
The input arrives from cortical areas adjacent to the primary motor cortex (premotor, SMA, somatosensory), and output returns to the primary motor cortex and closely associated premotor areas.
- Guyton and Hall, p. 709-710
2. Caudate Circuit - Cognitive Control of Motor Sequences
The caudate circuit controls cognitive (thought-driven) motor planning - converting a mental intention into an appropriate, rapid sequence of movements. Example: seeing a threat and instantly initiating turning, running, and climbing - all as a coordinated subconscious plan.
The pathway:
Prefrontal/association cortex → Caudate → GPi → Ventroanterior thalamus → Prefrontal, premotor, and SMA cortex
This circuit does not return to the primary motor cortex directly; instead it feeds the supplementary motor area, which plans sequential movements lasting 5+ seconds.
- Guyton and Hall, p. 710
3. Timing and Scaling of Movement
The basal ganglia, working with the posterior parietal cortex, determine:
- How rapidly a movement is performed (timing)
- How large the movement will be (scaling)
These functions are impaired in basal ganglia lesions - a patient can still write "A" but loses the ability to scale its size or adjust its speed.
- Guyton and Hall, p. 710-711
4. Behavioral Selection ("Focus Movement")
According to the modern view (Kandel, Principles of Neural Science), the basal ganglia act as a selection mechanism - choosing between competing behavioral options. The direct pathway facilitates a chosen action; the indirect pathway suppresses competing actions (center-surround inhibition model). This extends beyond motor behavior to include cognitive, motivational, and limbic selections.
- Kandel, Principles of Neural Science, p. 981
Direct and Indirect Pathways (The Core Circuit)
This is the most testable and clinically important concept:
Direct Pathway (facilitates movement)
Cortex → Striatum (D1 receptors, substance P) → GPi/SNr (inhibited) → Thalamus disinhibited → Motor cortex activated
Net effect: increased cortical motor activity - movement is facilitated.
Indirect Pathway (suppresses movement)
Cortex → Striatum (D2 receptors, enkephalin) → GPe (inhibited) → STN disinhibited → GPi/SNr excited → Thalamus inhibited → Motor cortex suppressed
Net effect: decreased cortical motor activity - movement is suppressed.
Hyperdirect Pathway
A direct cortex → STN → GPi pathway (bypassing the striatum) provides the fastest route to suppress movement - a rapid "brake" before full action selection.
Role of Dopamine (from SNc)
- Acts on D1 receptors in the striatum → facilitates the direct pathway (pro-movement)
- Acts on D2 receptors in the striatum → inhibits the indirect pathway (also pro-movement)
- Net effect of dopamine: promotes movement and reduces unwanted suppression
Loss of dopamine (as in Parkinson's disease) tips the balance toward the indirect pathway - too much GPi/STN firing, excessive thalamic inhibition, and hypokinesia.
- Bradley and Daroff's Neurology in Clinical Practice
- Kandel, Principles of Neural Science, p. 983
Neurotransmitters in the Basal Ganglia
| Pathway | Transmitter | Effect |
|---|---|---|
| Striatum → GPi/SNr (direct) | GABA + Substance P | Inhibitory (disinhibits thalamus) |
| Striatum → GPe (indirect) | GABA + Enkephalin | Inhibitory |
| GPe → STN | GABA | Inhibitory |
| STN → GPi | Glutamate | Excitatory |
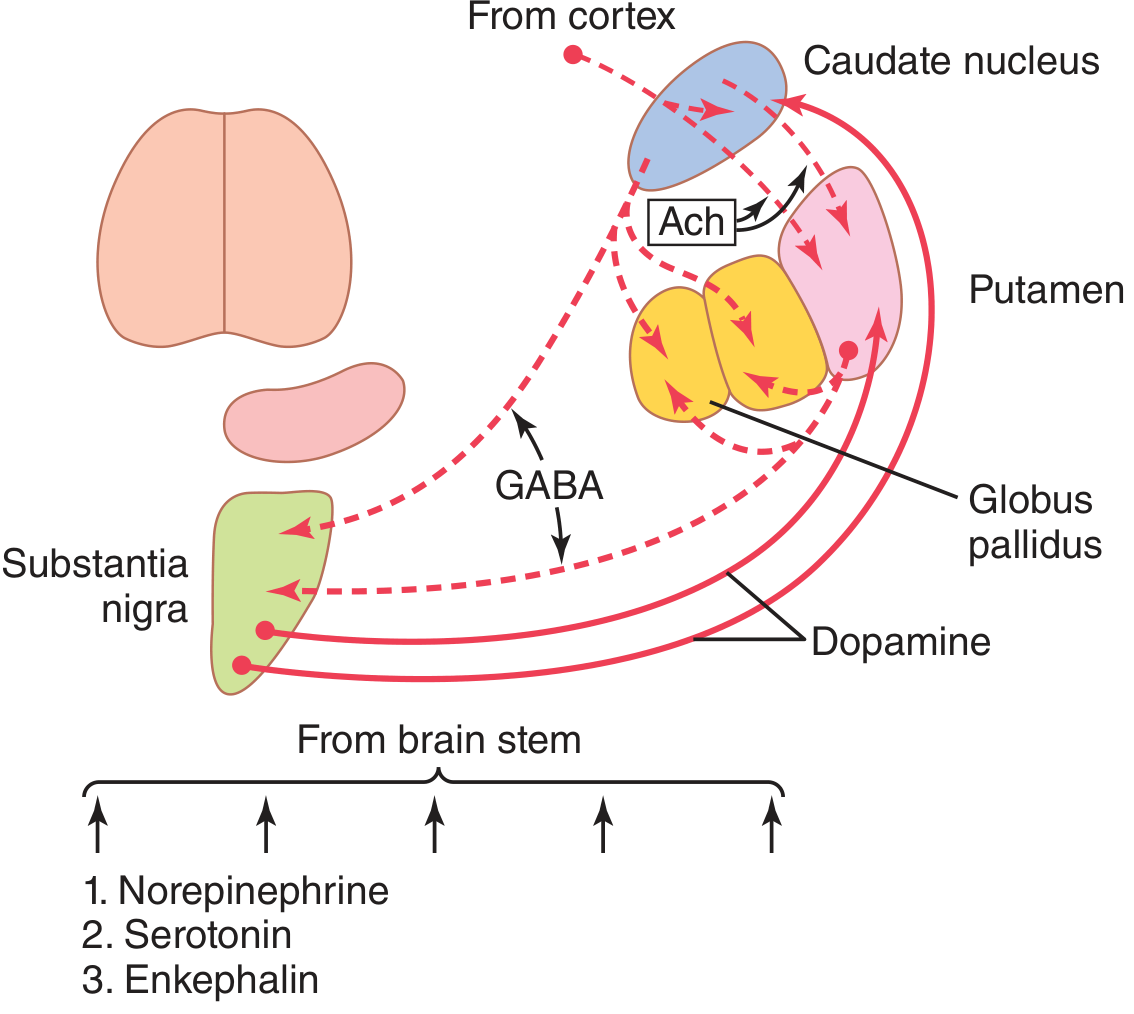
| SNc → Striatum | Dopamine | D1: excites direct; D2: inhibits indirect |
| Cortex → Striatum | Glutamate | Excitatory (main drive) |
| Striatum interneurons | Acetylcholine | Modulator |
| Brain stem inputs | NE, Serotonin, Enkephalin | Modulatory |
GABA is the dominant transmitter in the basal ganglia, making virtually all feedback loops negative feedback loops - lending stability to motor control.
Disorders of the Basal Ganglia
Classification: Hypo- vs. Hyperkinetic
| Type | Mechanism | Example |
|---|---|---|
| Hypokinetic | Increased GPi output → excess thalamic inhibition | Parkinson's disease |
| Hyperkinetic | Decreased GPi output → insufficient thalamic inhibition | Huntington's, Hemiballismus, Chorea |
1. Parkinson's Disease
Pathology: Degeneration of dopaminergic neurons in the substantia nigra pars compacta. Patients have lost >80% of these neurons by the time symptoms appear. Characterized by Lewy bodies (alpha-synuclein aggregates).
Mechanism:
- Dopamine loss → direct pathway underactive, indirect pathway overactive
- STN and GPi fire excessively → thalamus is over-inhibited
- SMA and motor cortex receive reduced drive → bradykinesia and akinesia
Classic Motor Features (TRAP):
- Tremor - resting (pill-rolling), 4-6 Hz; disappears with intentional movement (unlike cerebellar tremor)
- Rigidity - lead-pipe or cogwheel; due to overexcitation of motor system from disinhibited caudate/putamen
- Akinesia/Bradykinesia - most disabling; slowness initiating and executing movement
- Postural instability - loss of righting reflexes
Non-motor features: Sleep disturbances, depression/anxiety, autonomic dysfunction (constipation, orthostatic hypotension), and cognitive impairment in advanced disease.
Treatment:
-
L-Dopa (with carbidopa): crosses BBB; converted to dopamine; restores direct/indirect balance; most effective for rigidity and akinesia; does not slow disease progression
-
MAO-B inhibitors (e.g., selegiline): reduce dopamine breakdown; may slow neuronal degeneration
-
Dopamine agonists (e.g., pramipexole, ropinirole)
-
Deep Brain Stimulation (STN or GPi): high-frequency stimulation suppresses overactive circuits
-
Experimental: dopaminergic cell transplantation
-
Guyton and Hall, p. 712; Neuroscience: Exploring the Brain, p. 1356-1359
2. Huntington's Disease
Pathology: Autosomal dominant (chromosome 4, CAG trinucleotide repeat expansion) in the gene encoding huntingtin protein. Normal: 8-35 CAG repeats. Disease: >36 repeats. The abnormally long huntingtin aggregates and triggers progressive degeneration of medium spiny neurons in the caudate and putamen - especially those of the indirect pathway (GABA/enkephalin neurons → GPe).
Mechanism:
- Loss of indirect pathway neurons → GPe is disinhibited → STN is inhibited → GPi output reduced
- Reduced GPi inhibition of thalamus → thalamocortical pathway overactive
- Excess, unwanted motor output → choreiform movements
Features:
- Onset age 30-40 years; affects men and women equally
- Early: Flicking movements of individual muscles (chorea)
- Progressive: Severe distortional movements of the entire body (choreoathetosis)
- Dementia - due to loss of ACh-secreting neurons in cerebral cortex
- Death typically 15-20 years after onset
Genetics note: CAG repeats encode extra glutamine residues in huntingtin. The mutant protein misfolds, aggregates, and triggers programmed neuronal death - possibly by disrupting normal huntingtin's role in counteracting apoptosis signals.
- Guyton and Hall, p. 713; Neuroscience: Exploring the Brain, p. 1357-1359
3. Hemiballismus
Pathology: Lesion of the subthalamic nucleus (STN) - usually due to infarct.
Mechanism: Loss of STN → GPi is not driven → thalamus disinhibited → uncontrolled motor output.
Feature: Sudden, violent, flailing movements of one entire limb (hemi-ballism). One of the most dramatic hyperkinetic disorders.
- Guyton and Hall, p. 710
4. Athetosis
Pathology: Lesions of the globus pallidus.
Feature: Slow, writhing, continuous movements of a hand, arm, neck, or face. Often seen in cerebral palsy (neonatal asphyxia damaging the globus pallidus).
5. Chorea (not Huntington's)
Pathology: Multiple small lesions in the putamen (e.g., Sydenham's chorea following streptococcal infection; drug-induced chorea).
Feature: Rapid, random, involuntary flicking movements of the hands, face, and limbs. Less severe than hemiballismus.
6. Other Basal Ganglia-Related Disorders (Kandel model)
| Disorder | Proposed Mechanism |
|---|---|
| Schizophrenia | General failure to suppress non-selected behavioral options |
| ADHD / Tourette syndrome | Intrusion of non-selected motor/vocal options |
| OCD | Pathologically dominant, recurrent behavioral options that cannot be suppressed |
| Addiction | Disruption of reinforcement learning circuits; pathological habit formation |
Summary: Lesion-Phenotype Correlations
| Structure Damaged | Disorder | Movement Type |
|---|---|---|
| Substantia nigra pars compacta | Parkinson's disease | Hypokinesia, resting tremor, rigidity |
| Caudate + Putamen (GABA neurons) | Huntington's disease | Chorea + dementia |
| Subthalamic nucleus | Hemiballismus | Violent flailing limb movements |
| Globus pallidus | Athetosis | Slow writhing movements |
| Putamen (small lesions) | Chorea | Rapid flicking movements |
Sources: Guyton and Hall Textbook of Medical Physiology, pp. 709-713 | Neuroscience: Exploring the Brain, 5th Ed., pp. 1355-1360 | Kandel, Principles of Neural Science, 6th Ed., pp. 980-984 | Bradley and Daroff's Neurology in Clinical Practice
EEG and role of sleep
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from Guyton & Hall, Ganong's, and Neuroscience: Exploring the Brain. The EEG sleep stage image is excellent. Let me compile the full response.
EEG and the Role of Sleep
Part 1 - The Electroencephalogram (EEG)
What is the EEG?
The EEG (electroencephalogram) is a recording of the electrical activity of the brain measured from scalp electrodes through the unopened skull. First described in humans in 1929 by Austrian psychiatrist Hans Berger, who observed that waking and sleeping EEGs are distinctly different.
The EEG does not record action potentials. It records the summation of dendritic postsynaptic potentials from the densely packed, similarly oriented pyramidal neurons in the superficial layers of the cerebral cortex. When synaptic endings on dendrites become active, current flows into and out of these current sinks and sources, producing wavelike potential fluctuations in the extracellular volume. The cell body-dendrite relationship acts as a constantly shifting dipole.
-
When dendritic activity is negative relative to the cell body → neurons are depolarized and hyperexcitable
-
When dendritic activity is positive relative to the cell body → neurons are hyperpolarized and less excitable
-
Ganong's Review of Medical Physiology, 26th Ed., p. 280
Recording the EEG
- ~24 electrodes applied to standard scalp positions (10-20 system) using conductive paste
- Voltages measured between pairs of electrodes: 0-200 microvolts amplitude; 0.5 to 50+ Hz frequency
- Different electrode pairs examine anterior vs. posterior, left vs. right regions
Generation of Synchronous Rhythms: The Thalamo-Cortical Pacemaker
Rhythmic EEG waves are generated by the thalamus acting as a pacemaker. Individual thalamic neurons have voltage-gated ion channels that allow self-sustaining rhythmic discharges. These become synchronized via excitatory-inhibitory thalamic neuron networks, then transmitted to the cortex via thalamocortical axons - compelling large groups of cortical neurons to march to the thalamic beat.
- Neuroscience: Exploring the Brain, 5th Ed., p. 1719
The Four Brain Wave Types
| Wave | Frequency | Amplitude | State | Location |
|---|---|---|---|---|
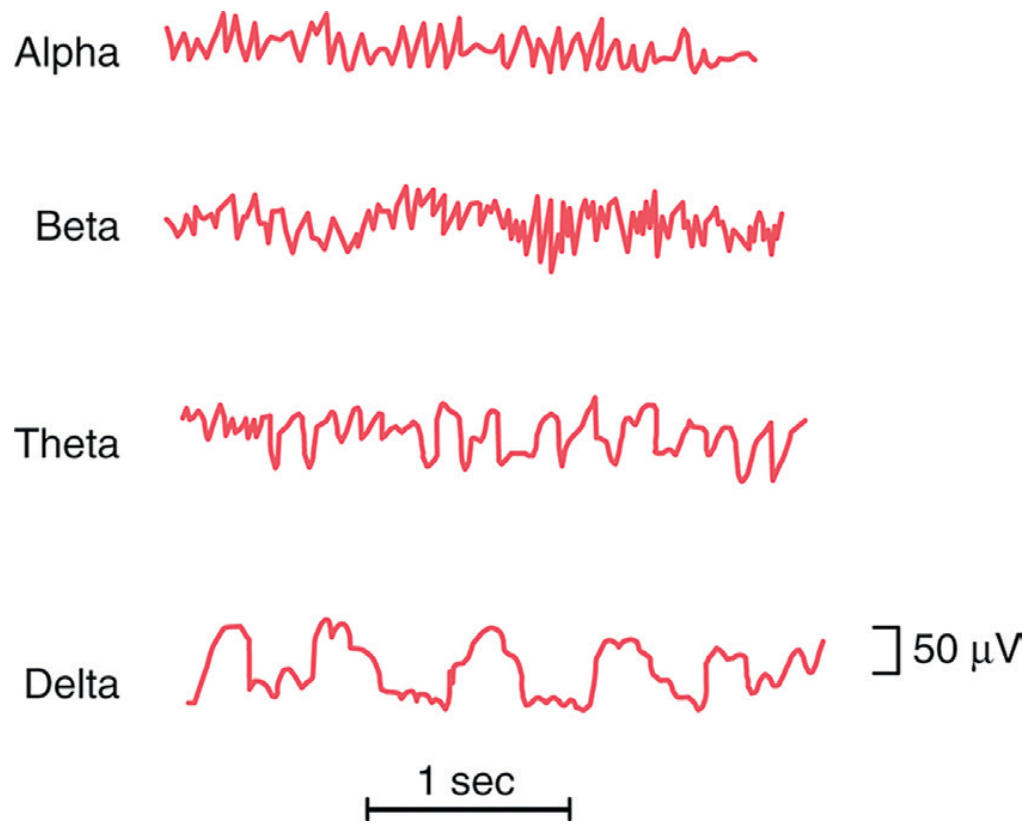
| Beta (β) | >14 Hz (up to 80 Hz) | Low (~20 µV) | Active thinking, focused attention, eyes open | Parietal, frontal |
| Alpha (α) | 8-13 Hz | ~50 µV | Awake, relaxed, eyes closed, quiet mental state | Occipital (mainly), parietal, frontal |
| Theta (θ) | 4-7 Hz | Medium | Children normally; emotional stress/drowsiness in adults; light sleep (Stage 1) | Parietal, temporal |
| Delta (δ) | <4 Hz (0.5-2 Hz) | High (>100 µV) | Deep sleep (Stages 3-4); coma; infants | Widespread |
Key clinical point: Opening the eyes in bright light immediately replaces alpha waves with low-voltage asynchronous beta waves - this is called alpha blocking or the alpha arousal response.
- Guyton and Hall Textbook of Medical Physiology, p. 745
Clinical Uses of the EEG
- Epilepsy - most important indication; seizures show characteristic high-voltage spike-wave discharges
- Focal brain lesions - subdural hematoma, tumor, abscess dampen activity over the affected area
- Sleep disorders - polysomnography uses EEG to stage sleep
- Brain death - electrocerebral silence (isoelectric EEG)
- Encephalopathy / coma staging - progressive slowing correlates with depth of coma
- Anesthesia monitoring - depth of surgical anesthesia
Part 2 - Sleep Physiology
Definition
Sleep is a state of unconsciousness from which a person can be aroused by sensory or other stimuli - distinguishing it from coma (from which the person cannot be aroused).
Two Fundamental Types of Sleep
Each night, sleep alternates between two distinct types in ~90-minute ultradian cycles:
| Feature | NREM (Slow-Wave Sleep) | REM (Paradoxical Sleep) |
|---|---|---|
| EEG | High voltage, slow (synchronized) | Low voltage, fast (desynchronized) - like waking! |
| Eye movements | Rare | Rapid (hence REM) |
| Muscle tone | Reduced | Extremely depressed (atonia); eye + respiratory muscles spared |
| Dreaming | Dull, logical, repetitive; rarely remembered | Vivid, illogical, bizarre; remembered if awakened |
| HR/RR | Regular, decreased | Irregular |
| Brain metabolism | Decreased | Increased up to 20% |
| Arousal threshold | Progressively harder | Very difficult to arouse, yet person wakes spontaneously in the morning |
| Proportion of night | ~75% | ~25% |
- Guyton and Hall, p. 741-742
NREM Sleep Stages (1 through 4)
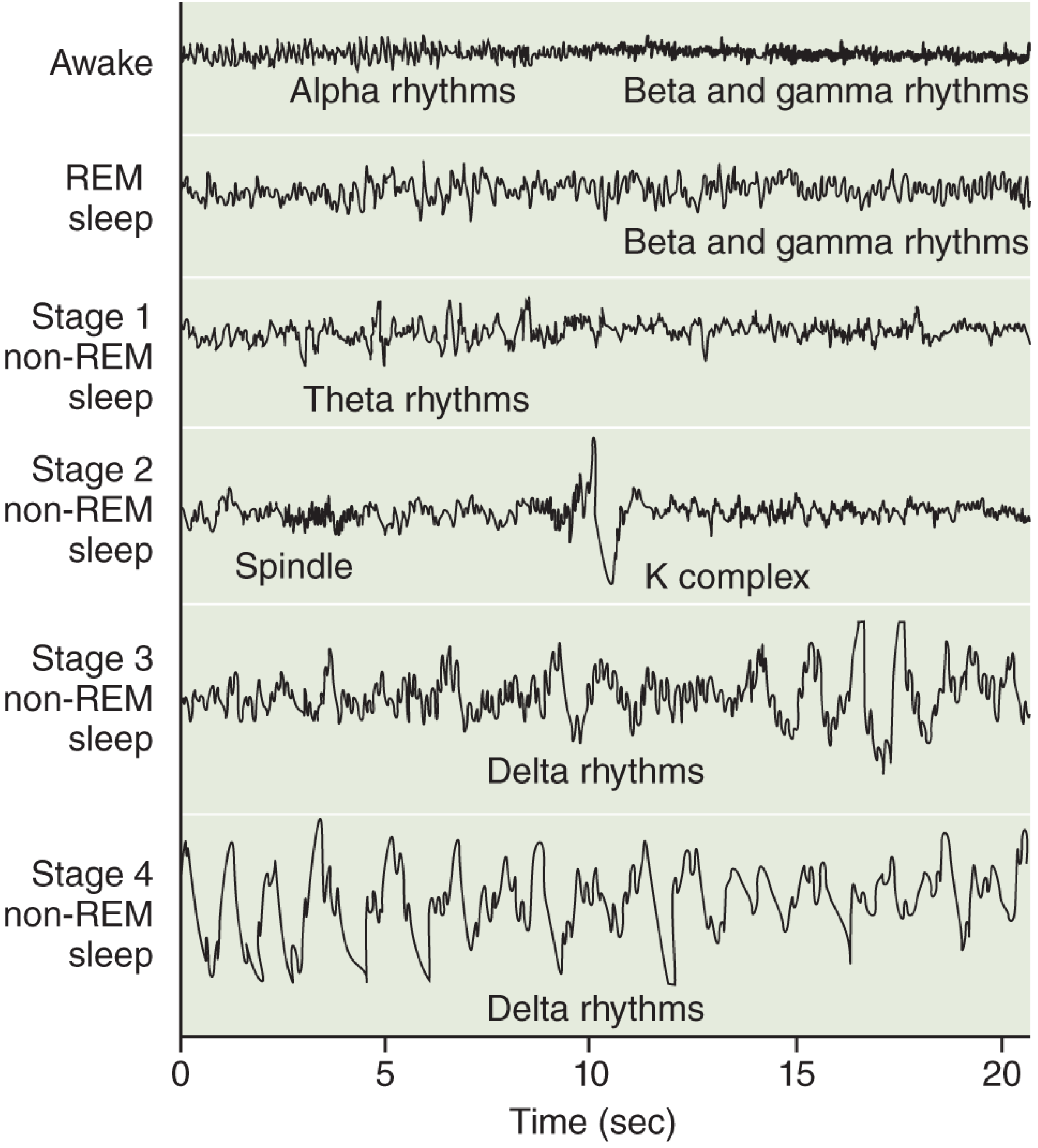
| Stage | EEG Pattern | Characteristics |
|---|---|---|
| Stage 1 | Theta waves (4-7 Hz), low voltage | Light sleep; transition from waking; easily aroused; hypnic jerks may occur |
| Stage 2 | Sleep spindles (12-14 Hz bursts) + K-complexes (sharp negative deflection followed by positive wave) | Definite sleep; harder to arouse; no eye movements |
| Stage 3 | Delta waves (<4 Hz) making up 20-50% of the EEG | Transition to deep sleep |
| Stage 4 | Delta waves >50% | Deepest NREM; most restorative; slowest HR, BP, RR; GH released here; hardest to arouse |
Stages 3 and 4 together = slow-wave sleep (SWS) or deep sleep - these predominate in the first third of the night.
The Sleep Cycle - Architecture Through the Night
A typical night:
- Sleep onset → Stage 1 → Stage 2 → Stage 3 → Stage 4 (takes ~30-45 min)
- Brief REM episode (~5-10 min)
- Return to NREM, then REM again
- Each cycle ~90 minutes; 4-6 cycles per night
As the night progresses:
-
Deep NREM (Stages 3-4) decreases - most occurs in the first 1/3 of night
-
REM duration increases - most REM (including periods of 30-50 min) occurs in the last third of the night
-
There is an obligatory ~30-min NREM refractory period between REM episodes
-
Neuroscience: Exploring the Brain, p. 1737
Neural Mechanisms of Sleep
Active Sleep Induction (Not Passive Fatigue)
Sleep is not simply the passive result of the brain "running out of energy." It is an actively induced state. Evidence: transecting the brain stem at the midpontine level creates a brain that never sleeps - a center below this level is required to actively inhibit wakefulness.
Sleep-Promoting Centers
- Raphe nuclei (lower pons, medulla) → secrete serotonin → widespread inhibition of thalamus, hypothalamus, limbic system, neocortex → promotes sleep. Blocking serotonin synthesis prevents sleep for days.
- Nucleus tractus solitarius (medulla) → also promotes sleep
- Ventrolateral preoptic area (VLPO) of hypothalamus → GABAergic inhibition of wakefulness systems
Wakefulness-Promoting Systems
- Reticular activating system (RAS) - mesencephalic and upper pontine reticular nuclei fire tonically during waking; positive feedback with cortex maintains arousal
- Locus coeruleus - norepinephrine; fires most during waking, silent during REM
- Raphe nuclei (paradoxically) - serotonin facilitates waking under some conditions
- Tuberomammillary nucleus (TMN) - histamine; strongly promotes wakefulness; antihistamines cause drowsiness by blocking these
- Orexin (Hypocretin) neurons (lateral hypothalamus) - fire during waking, nearly silent during sleep; loss causes narcolepsy (sudden attacks of sleep + cataplexy)
REM-ON / REM-OFF Flip-Flop Switch
The alternation between NREM and REM is controlled by antagonistic brain stem populations:
| Neuron type | Location | Transmitter | Fires during |
|---|---|---|---|
| REM-OFF | Locus coeruleus, raphe | NE, Serotonin | Waking, NREM; silent during REM |
| REM-ON | Pontine tegmentum (PPT, LDT) | Acetylcholine | Just before and during REM |
The increasing activity of REM-ON neurons triggers REM sleep, activating the forebrain and generating rapid eye movements. Their mutual inhibition of REM-OFF neurons creates the ~90-minute oscillation.
- Guyton and Hall, p. 744-745
Circadian Regulation
The suprachiasmatic nucleus (SCN) of the hypothalamus is the master circadian clock (24-hour rhythm), entrained by light via the retinohypothalamic tract. It controls the sleep-wake timing (when you sleep), but does not directly generate the REM/NREM cycle (the ~90-minute ultradian rhythm). The SCN drives the pineal gland to secrete melatonin at night, promoting sleep onset.
Part 3 - The Role of Sleep (Why We Sleep)
Sleep is Essential for Homeostasis
Sleep is universal across all mammals. After total sleep deprivation:
- Cognitive deterioration is rapid and severe
- Prolonged deprivation → irritability, psychosis, hallucinations
- Rats deprived of sleep for 2-3 weeks die
- "Rebound sleep" - after deprivation, the brain selectively recovers lost sleep stages (especially deep NREM and REM)
Proposed Functions of Sleep
| Function | Evidence |
|---|---|
| Neural/synaptic restoration | Sleep restores normal balance of neuronal excitability after waking |
| Memory consolidation | Both NREM (declarative/hippocampal memory) and REM (procedural, emotional memory) play roles |
| Synaptic homeostasis | "Forgetting" - targeted erasure of weak synapses to prevent informational overload (synaptic homeostasis hypothesis) |
| Glymphatic clearance | Brain's waste clearance system is most active during sleep; removes amyloid-β and tau - relevant to Alzheimer's disease |
| Neural maturation | Children and infants sleep far more; promotes synaptic development |
| Metabolic conservation | 10-30% reduction in BP, RR, and BMR during NREM |
| Immune function | Illness increases sleep; sickness-induced sleep diverts energy to fighting infection |
| Growth hormone release | Pulsatile GH secretion occurs predominantly during Stage 4 NREM sleep |
- Guyton and Hall, p. 744
- Neuroscience: Exploring the Brain, p. 1738
Functions of REM Sleep Specifically
- Processing emotional memories
- Procedural motor learning (skill consolidation)
- Creative insight and novel association
- Dreaming - the vivid, narrative-quality dreams of REM involve the amygdala, limbic cortex, and visual association cortex; frontal lobe is relatively suppressed (explaining why dreams are illogical but feel real)
Summary Comparison Table
| Parameter | Alert Waking | Relaxed Waking | NREM (Deep) | REM |
|---|---|---|---|---|
| EEG dominant wave | Beta | Alpha | Delta | Beta (desynchronized) |
| Frequency | >14 Hz | 8-13 Hz | <4 Hz | >14 Hz |
| Amplitude | Low | Medium | High | Low |
| Consciousness | Full | Full | Absent | Dreaming |
| Muscle tone | Normal | Normal | Reduced | Absent (atonia) |
| HR/BP | Normal/elevated | Normal | Reduced 10-30% | Irregular |
| Dreaming | No | No | Rarely (not recalled) | Yes (recalled) |
Sources: Guyton and Hall Textbook of Medical Physiology, pp. 741-748 | Ganong's Review of Medical Physiology, 26th Ed., p. 280 | Neuroscience: Exploring the Brain, 5th Ed., pp. 1702-1742
Functions of thalamus (physiology)
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
I now have rich content from multiple authoritative textbooks. Let me compile the complete answer.
Functions of the Thalamus (Physiology)
Overview
The thalamus (from Greek: "inner chamber") is a paired ovoid gray matter structure forming the largest part of the diencephalon, flanking the third ventricle. It is the major subcortical relay station for the entire cerebral cortex.
The central principle: Nearly all pathways projecting to the cerebral cortex do so via synaptic relays in the thalamus - including sensory, motor, limbic, and associative inputs. The single exception is olfaction, which reaches the cortex directly.
The thalamus is not a passive relay. It processes, filters, and gates information, and through massive reciprocal corticothalamic feedback (which actually outnumbers thalamocortical projections), it participates in attention, arousal, consciousness, and learning.
- Neuroanatomy through Clinical Cases, 3rd Ed., p. 306
- Costanzo Physiology, 7th Ed., p. 77
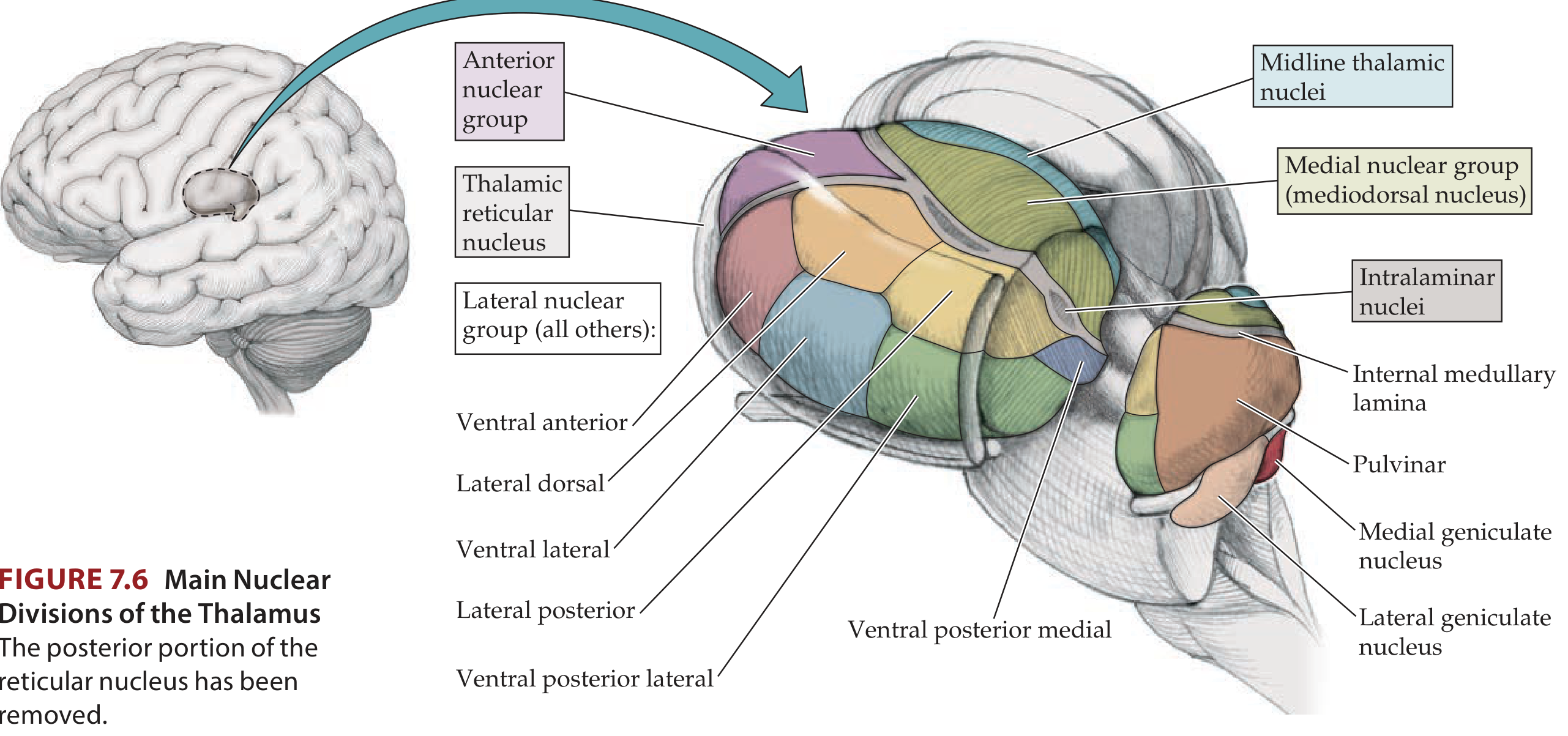
Anatomy: Nuclear Organization
The thalamus is divided by a Y-shaped internal medullary lamina into:
- Anterior nuclear group
- Medial nuclear group (mediodorsal nucleus)
- Lateral nuclear group (dorsal tier: lateral dorsal, lateral posterior, pulvinar; ventral tier: VA, VL, VPL, VPM, LGN, MGN)
Additional groups:
- Intralaminar nuclei (within the internal medullary lamina; largest: centromedian nucleus)
- Midline nuclei (adjacent to third ventricle; may fuse to form interthalamic adhesion)
- Thalamic reticular nucleus - a thin shell enveloping the lateral thalamus
Classification of Thalamic Nuclei by Function
There are three functional classes:
1. Specific Relay (First-Order) Nuclei
Receive driver inputs from ascending pathways and relay topographically to a single primary cortical area. Their projections are the most focal (+).
2. Association Relay (Higher-Order) Nuclei
Receive highly processed, multimodal inputs (often from cortical layer 5 pyramidal neurons) and project to association cortex areas (++).
3. Diffuse-Projection (Non-Specific) Nuclei
Receive diverse inputs and project widely to large cortical and subcortical territories (+++). Regulate general cortical excitability and arousal.
Thalamic Nuclei - Detailed Functions
Specific Sensory Relay Nuclei (Ventral Tier, Lateral Group)
| Nucleus | Main Afferents | Projection | Function |
|---|---|---|---|
| VPL (Ventral Posterolateral) | Medial lemniscus + spinothalamic tract | Primary somatosensory cortex (S1) | Relays somatosensory from body (touch, pain, temperature, proprioception, pressure) |
| VPM (Ventral Posteromedial) | Trigeminal lemniscus + trigeminothalamic tract + taste (NTS) | Primary somatosensory + taste cortex | Relays somatosensory from head/face; taste sensation |
| LGN (Lateral Geniculate Nucleus) | Optic tract (retina) | Primary visual cortex (V1, area 17) | Relay of visual information |
| MGN (Medial Geniculate Nucleus) | Inferior colliculus | Primary auditory cortex (A1) | Relay of auditory information |
Note on topography: Thalamic sensory relays are somatotopically organized. VPM receives input from the head; VPL receives input from the rest of the body. These project topographically to S1, creating the somatosensory homunculus.
Parallel submodality processing: Tactile/proprioceptive fibers (medial lemniscus) and pain/temperature fibers (spinothalamic tract) travel separately but both terminate in VPL/VPM - demonstrating parallel submodality processing even within the thalamus.
Motor Relay Nuclei
| Nucleus | Main Afferents | Projection | Function |
|---|---|---|---|
| VL (Ventral Lateral) | Dentate nucleus of cerebellum | Motor and premotor cortex | Relays cerebellar output to cortex; control of voluntary movement |
| VA (Ventral Anterior) | GPi (globus pallidus internal) + SNr + deep cerebellar nuclei | Prefrontal, premotor, motor, SMA | Relays basal ganglia output to cortex; motor planning and initiation |
These two nuclei are the critical link through which the cerebellum and basal ganglia influence voluntary motor control via the cortex.
Limbic / Memory-Related Nuclei
| Nucleus | Main Afferents | Projection | Function |
|---|---|---|---|
| Anterior nucleus | Mammillary bodies (hypothalamus) + hippocampal formation | Cingulate cortex, parahippocampal gyrus | Papez circuit; expression of emotion; learning and memory |
| Medial Dorsal (MD) | Amygdala, hypothalamus, brainstem | Prefrontal cortex, premotor, temporal cortex | Integration of emotional and cognitive inputs; mood, affect, judgment |
| Lateral Dorsal | Pretectal area | Cingulate cortex, retrosplenial cortex | Emotion expression; functions with anterior nucleus |
The anterior nucleus forms a key link in the Papez circuit for memory and emotion:
Hippocampus → Fornix → Mammillary bodies → Anterior thalamic nucleus → Cingulate cortex → Entorhinal cortex → back to Hippocampus
Damage to the anterior or mediodorsal thalamic nuclei (e.g., in Korsakoff syndrome from thiamine deficiency) causes thalamic amnesia.
Association Relay Nuclei (Polymodal)
| Nucleus | Afferents | Projection | Function |
|---|---|---|---|
| Pulvinar (largest thalamic nucleus) | Superior colliculus; visual, auditory, somatosensory cortices | Parieto-temporo-occipital association cortex | Behavioral orientation toward relevant stimuli; integration of multimodal sensory information; visual attention |
| Lateral Posterior | Superior colliculus, parietal cortex, precuneus | Parietal association cortex | Sensory integration |
Diffuse-Projection (Non-Specific) Nuclei
| Nucleus | Afferents | Projection | Function |
|---|---|---|---|
| Intralaminar nuclei (centromedian etc.) | Reticular formation, spinothalamic tract, globus pallidus | Basal ganglia + widespread cortex | General cortical arousal and activation; pain processing |
| Midline nuclei | Reticular formation, hypothalamus, striatum | Striatum, hippocampus, limbic cortex | Modulation of cortical excitability; visceral and limbic functions |
The Thalamic Reticular Nucleus (TRN) - The Thalamic Gatekeeper
The TRN is a thin shell of GABAergic inhibitory neurons completely surrounding the lateral thalamus. It is unique among thalamic nuclei because it:
- Does not project to the cortex
- Receives collateral inputs from both thalamocortical AND corticothalamic axons as they pass through it
- Projects back onto other thalamic relay nuclei with inhibitory (GABAergic) synapses
Function: The TRN acts as a thalamic gatekeeper. It samples both thalamic output to the cortex and cortical feedback, then uses this information to regulate (inhibit) thalamic relay activity. This gives the cortex a mechanism to actively suppress competing sensory inputs - the cellular basis of selective attention.
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 224
The Concept of Drivers vs. Modulators
A modern framework (refined from classical relay nuclei classification):
| Input Type | Source | Action |
|---|---|---|
| Drivers | Ascending sensory pathways (first-order) OR cortical layer 5 neurons (higher-order) | Determine the nature of the thalamic relay - what information is transmitted |
| Modulators | Cortical layer 6 feedback + monoaminergic (LC, raphe) + cholinergic (basal forebrain, PPT/LDT) brainstem inputs | Regulate how efficiently the relay transmits (gain control) |
Over half of thalamic circuits in primates are higher-order relays (cortex → thalamus → different cortical area), meaning the thalamus is not just a relay from periphery to cortex but also a major cortico-thalamo-cortical communication hub.
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 225
Broader Functional Roles of the Thalamus
1. Sensory Relay and Gating
Primary function for all senses (except olfaction) - receives, processes, and projects sensory information to the appropriate primary cortical areas with precise topographic organization.
2. Motor Control Interface
VL and VA relay cerebellar and basal ganglia outputs to the motor cortex, making the thalamus the essential intermediary in the cortico-basal ganglia-thalamo-cortical and cortico-cerebello-thalamo-cortical loops.
3. Arousal and Consciousness
The intralaminar and midline nuclei receive input from the ascending reticular activating system (ARAS) and project diffusely to the cortex to maintain wakefulness and arousal. Bilateral thalamic damage produces coma or disorders of consciousness. The thalamus acts as an "ON/OFF switch" for consciousness.
Evidence: Electrical stimulation of the centromedial thalamus can reverse anesthetic-induced unconsciousness and has produced behavioral improvement in patients with traumatic brain injury.
4. Selective Attention
Via the TRN's gating function and corticothalamic feedback, the thalamus filters which sensory streams reach cortical awareness - the neural substrate of selective attention.
5. Memory and Emotion
Anterior and mediodorsal nuclei form essential links in limbic circuits (Papez circuit). Thalamic lesions from stroke, hemorrhage, or Korsakoff syndrome cause thalamic amnesia and affective disorders.
6. Sleep-Wake Regulation
During NREM sleep, thalamic neurons shift from tonic firing (wakefulness) to burst firing (sleep) - generating sleep spindles and K-complexes seen on EEG. This burst firing prevents afferent stimuli from arousing the cortex, creating the sensory gate that keeps us asleep. The thalamus is the generator of the ~8-14 Hz sleep spindle oscillations.
7. Pain Processing
VPL/VPM relay sharp, discriminative pain (spinothalamic tract input); the intralaminar nuclei process the affective-motivational component of pain. This is why thalamotomy (surgical lesioning) can relieve chronic pain.
Key Sensory Pathways Through the Thalamus
| Modality | Spinal/Brainstem pathway | Thalamic relay | Cortical destination |
|---|---|---|---|
| Touch/Proprioception (body) | Dorsal columns → Medial lemniscus | VPL | S1 (parietal lobe) |
| Pain/Temperature (body) | Spinothalamic tract | VPL | S1 + anterior cingulate |
| Touch/Pain (face) | Trigeminal system | VPM | S1 (face area) |
| Taste | NTS → VPM | VPM | Gustatory cortex (insular/opercular) |
| Vision | Optic tract | LGN | V1 (occipital lobe) |
| Hearing | Inferior colliculus | MGN | A1 (temporal lobe) |
| Cerebellum output | Deep cerebellar nuclei | VL | Motor/premotor cortex |
| Basal ganglia output | GPi / SNr | VA/VL | Motor/premotor/prefrontal cortex |
Thalamic Lesions and Clinical Correlates
| Lesion | Structure Damaged | Deficit |
|---|---|---|
| VPL/VPM infarct | Contralateral hemibody sensory loss (pain, temp, touch) | Thalamic syndrome (Dejerine-Roussy): burning/aching contralateral pain |
| Anterior nucleus damage | Limbic circuit | Amnesia, emotional blunting |
| Mediodorsal nucleus damage (Korsakoff) | MD + mammillary bodies | Anterograde amnesia, confabulation |
| Bilateral intralaminar damage | ARAS → cortical arousal system | Coma, akinetic mutism |
| VL/VA damage | Cerebellar/BG output to cortex | Contralateral movement disorder |
| Pulvinar damage | Visual attention circuit | Hemineglect, visual inattention |
Sources: Neuroanatomy through Clinical Cases, 3rd Ed., pp. 306-313 | Kaplan & Sadock's Comprehensive Textbook of Psychiatry, pp. 223-230 | Costanzo Physiology, 7th Ed., p. 77 | Miller's Anesthesia, 10th Ed., pp. 694-695
What sare the important topics in neuro physiology 1st yr mbbs
Searching the Web
neurophysiology important topics 1st year MBBS NMC syllabus India 2024
Here is a comprehensive, well-organized guide to the important topics in Neurophysiology for 1st Year MBBS based on the NMC/CBME syllabus pattern and standard exam weightage:
Important Topics in Neurophysiology - 1st Year MBBS
Neurophysiology is covered under Physiology (Phase 1) and forms one of the highest-scoring and most conceptually rich sections of the 1st year MBBS examination. Based on NMC CBME pattern, university exam trends, and standard Guyton/Ganong coverage, here are the must-know topics organized by priority.
TIER 1 - Highest Exam Weightage (Must Know Thoroughly)
1. Nerve Physiology
- Resting membrane potential - ionic basis (Na⁺/K⁺ distribution, Goldman equation)
- Action potential - generation, phases (depolarization, overshoot, repolarization, after-potentials), ionic basis
- Refractory periods - absolute and relative, clinical significance
- Conduction velocity - factors affecting (myelination, fiber diameter, temperature)
- Classification of nerve fibers - A, B, C (Erlanger-Gasser); Ia, Ib, II, III, IV (Lloyd-Hunt)
- All-or-none law, saltatory conduction
2. Synapse
- Structure of a chemical synapse
- Synaptic transmission - step-by-step (quantal release, vesicle fusion, receptor activation)
- Neurotransmitters - types, release, reuptake
- Excitatory and inhibitory postsynaptic potentials (EPSP, IPSP)
- Summation - spatial vs. temporal
- Synaptic fatigue, facilitation, potentiation
- Types of inhibition - presynaptic, postsynaptic, feed-forward, feedback (Renshaw cell)
3. Sensory Physiology - Receptors and General Sensations
- Classification of sensory receptors
- Generator (receptor) potential vs. action potential
- Adaptation - rapidly adapting vs. slowly adapting
- Sensory coding - labeled line, frequency coding
- Somatic sensations - touch, pain, temperature, proprioception
- Pain - fast (A-delta) vs. slow (C fiber), referred pain (mechanism + examples), visceral pain
- Gate control theory of pain (Melzack and Wall)
- Anterolateral system (spinothalamic tract) vs. dorsal column-medial lemniscal pathway
4. Motor System
- Upper motor neuron (UMN) vs. lower motor neuron (LMN) - lesion features (classic exam question)
- Corticospinal (pyramidal) tract - origin, course, decussation, function
- Extrapyramidal system - components, functions
- Reflex arc - components, types
- Muscle spindle and Golgi tendon organ - structure, function, reflex role
- Stretch reflex (myotatic reflex) - mechanism, gamma motor neuron role
- Inverse stretch reflex (clasp-knife)
- Flexor withdrawal reflex, crossed extensor reflex
5. Cerebellum
- Functional divisions - vestibulocerebellum, spinocerebellum, cerebrocerebellum
- Functions - coordination, equilibrium, motor learning, feedforward control
- Cerebellar circuits - Purkinje cells, climbing fibers, mossy fibers, deep nuclei
- Features of cerebellar damage - dysmetria, ataxia, intention tremor, dysdiadochokinesia, dysarthria, hypotonia
6. Basal Ganglia
- Components - striatum (caudate + putamen), globus pallidus, subthalamic nucleus, substantia nigra
- Direct and indirect pathways - mechanism, dopamine role
- Disorders - Parkinson's disease (pathology, features, L-dopa treatment), Huntington's disease, hemiballismus, chorea
- Putamen circuit and caudate circuit
7. Thalamus
- Specific relay nuclei - VPL, VPM, LGN, MGN, VL, VA
- Non-specific (diffuse projection) nuclei - intralaminar, midline
- Thalamic reticular nucleus - gating and attention
- Functions - sensory relay, arousal, consciousness, pain
- Thalamic syndrome
TIER 2 - High Importance (Frequently Asked)
8. EEG and Sleep
- Brain wave types - alpha, beta, theta, delta (frequency, amplitude, state)
- EEG basis - summation of dendritic potentials
- Clinical uses - epilepsy, coma grading
- Sleep types - NREM (Stages 1-4) and REM
- Sleep cycle - 90-minute ultradian rhythm, architecture through the night
- REM features - paradoxical sleep, atonia, dreaming, brain metabolism
- Neural control of sleep - raphe nuclei (serotonin), locus coeruleus (NE), orexin/narcolepsy
- Functions of sleep - memory consolidation, glymphatic clearance, GH release
9. Higher Functions of the Nervous System
- Cerebral cortex - functional areas (motor, sensory, speech - Broca's, Wernicke's)
- Aphasia types - expressive (Broca's), receptive (Wernicke's), conduction
- Apraxia and agnosia - definitions
- Memory - types (declarative vs. non-declarative; short-term vs. long-term)
- Limbic system - components, functions (emotion, memory, behavior)
- Hypothalamus - thermoregulation, feeding, water balance, circadian rhythms
- Learning and long-term potentiation (LTP)
- Consciousness - ARAS, reticular activating system
10. Autonomic Nervous System (ANS)
- SNS vs. PNS - origin, ganglia location, neurotransmitters, receptors
- Adrenergic receptors - α1, α2, β1, β2 - locations and effects
- Cholinergic receptors - nicotinic vs. muscarinic - locations
- Autonomic effects on major organs - heart, blood vessels, GIT, eye, bladder
- Adrenal medulla as a modified sympathetic ganglion
- Autonomic reflexes - micturition, defecation, erection/ejaculation
11. Spinal Cord
- Organization - grey and white matter, laminae of Rexed
- Ascending tracts - dorsal columns, spinothalamic, spinocerebellar
- Descending tracts - corticospinal, rubrospinal, vestibulospinal, reticulospinal
- Brown-Séquard syndrome (hemisection features)
- Spinal shock - features, recovery
TIER 3 - Important but Less Frequently Asked
12. Special Senses
- Visual pathway - from retina to visual cortex; visual field defects at each level (very high yield!)
- Photoreceptors - rods vs. cones, phototransduction
- Accommodation reflex and pupillary light reflex - pathway
- Color vision - Young-Helmholtz trichromatic theory
- Auditory pathway - from cochlea to auditory cortex
- Vestibular system - semicircular canals, utricle/saccule, nystagmus
13. Neuromuscular Junction
- Structure - motor end plate, junctional folds
- Transmission - ACh release, binding, end-plate potential
- Myasthenia gravis - anti-AChR antibodies, clinical features, edrophonium test
- Curare and succinylcholine - mechanisms
14. Cerebrospinal Fluid (CSF)
- Formation - choroid plexus, rate (~500 mL/day, 150 mL volume)
- Circulation - lateral ventricles → 3rd ventricle → aqueduct → 4th ventricle → cisterns → arachnoid villi
- Composition and normal values - pressure (70-180 mmH₂O), protein, glucose, cells
- Lumbar puncture - normal vs. abnormal CSF
- Hydrocephalus - communicating vs. non-communicating
15. Blood-Brain Barrier (BBB)
- Structure - tight junctions of brain capillary endothelium + astrocytic feet
- Function - selective permeability, protection
- Circumventricular organs - areas lacking BBB (area postrema, median eminence)
- Clinical relevance - why L-dopa (not dopamine) works in Parkinson's
EXAM FORMAT TIPS
Long Questions (10 marks) - Most likely topics:
- Action potential - describe ionic basis and phases (diagram essential)
- Cerebellar functions and disorders
- Basal ganglia - pathways and Parkinson's disease
- Pain - types, pathways, referred pain, gate control theory
- Sleep - NREM vs. REM, neural mechanisms
- UMN vs. LMN lesion - features with comparison table
- Synaptic transmission
- Autonomic nervous system - comparison of SNS and PNS
Short Questions (5 marks) - Most likely topics:
- Resting membrane potential
- Thalamic nuclei and functions
- Muscle spindle
- EEG waves
- Gate control theory
- Stretch reflex
- Brown-Séquard syndrome
- CSF - formation and circulation
- Myasthenia gravis
- Neuromuscular junction
- Orexin/narcolepsy
- Visual pathway defects
MCQs - High-yield facts:
- Frequency of brain waves (alpha: 8-13 Hz; beta: >14 Hz; theta: 4-7 Hz; delta: <4 Hz)
- VPL relay: body somatosensory; VPM relay: face + taste
- LGN: vision; MGN: hearing
- Purkinje cells: only output of cerebellar cortex (inhibitory)
- Dopamine D1: direct pathway; D2: indirect pathway
- REM sleep: paradoxical, 25% of sleep, atonia
- Conduction velocity: A-alpha fastest (70-120 m/s); C fibers slowest (0.5-2 m/s)
- Renshaw cell: recurrent inhibition of alpha motor neurons
Recommended Books (1st Year MBBS)
| Book | Use |
|---|---|
| Guyton & Hall Textbook of Medical Physiology | Gold standard for concepts and mechanisms |
| Ganong's Review of Medical Physiology | Concise, excellent for revision |
| Sembulingam & Prema | India-specific, exam-oriented, good for quick revision |
| AK Jain | Popular in Indian medical colleges for MCQ preparation |
Topic Priority Summary by Marks Potential
★★★★★ Action potential, Synapse, Pain, Cerebellum, Basal ganglia
★★★★ UMN/LMN, Motor pathways, Thalamus, Sleep/EEG, ANS
★★★ Visual pathway, Muscle spindle reflexes, CSF, Memory/limbic
★★ Neuromuscular junction, Vestibular, Auditory pathway, BBB
The topics we already covered in this session - Cerebellum, Basal Ganglia, EEG/Sleep, and Thalamus - are all Tier 1-2 high-yield topics that together can fetch you 30-40 marks in the physiology examination. Covering those thoroughly and then building on the pain, synapse, and action potential chapters will give you a very strong neurophysiology preparation.
Upper motor lesions and lower motor lesions physiology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive content from Guyton & Hall, Ganong's, and Neuroanatomy through Clinical Cases. Let me compile the full detailed answer.
Upper Motor Neuron (UMN) and Lower Motor Neuron (LMN) Lesions
Part 1 - The Motor System: Overview
The voluntary motor system is organized into a two-neuron chain from cortex to muscle:
Cerebral Cortex (Motor Areas)
↓
UPPER MOTOR NEURON
(corticospinal tract)
↓
Anterior Horn (spinal cord)
↓
LOWER MOTOR NEURON
(peripheral nerve)
↓
Skeletal Muscle
This same two-neuron concept applies to the corticobulbar tract for cranial nerve motor nuclei (e.g., for face, tongue, pharynx).
Part 2 - Upper Motor Neuron (UMN)
Definition
Upper motor neurons are cortical and brainstem neurons whose axons descend to synapse on lower motor neurons (alpha motor neurons) in the anterior horn of the spinal cord (or cranial nerve nuclei in the brainstem). They do not directly contact muscle.
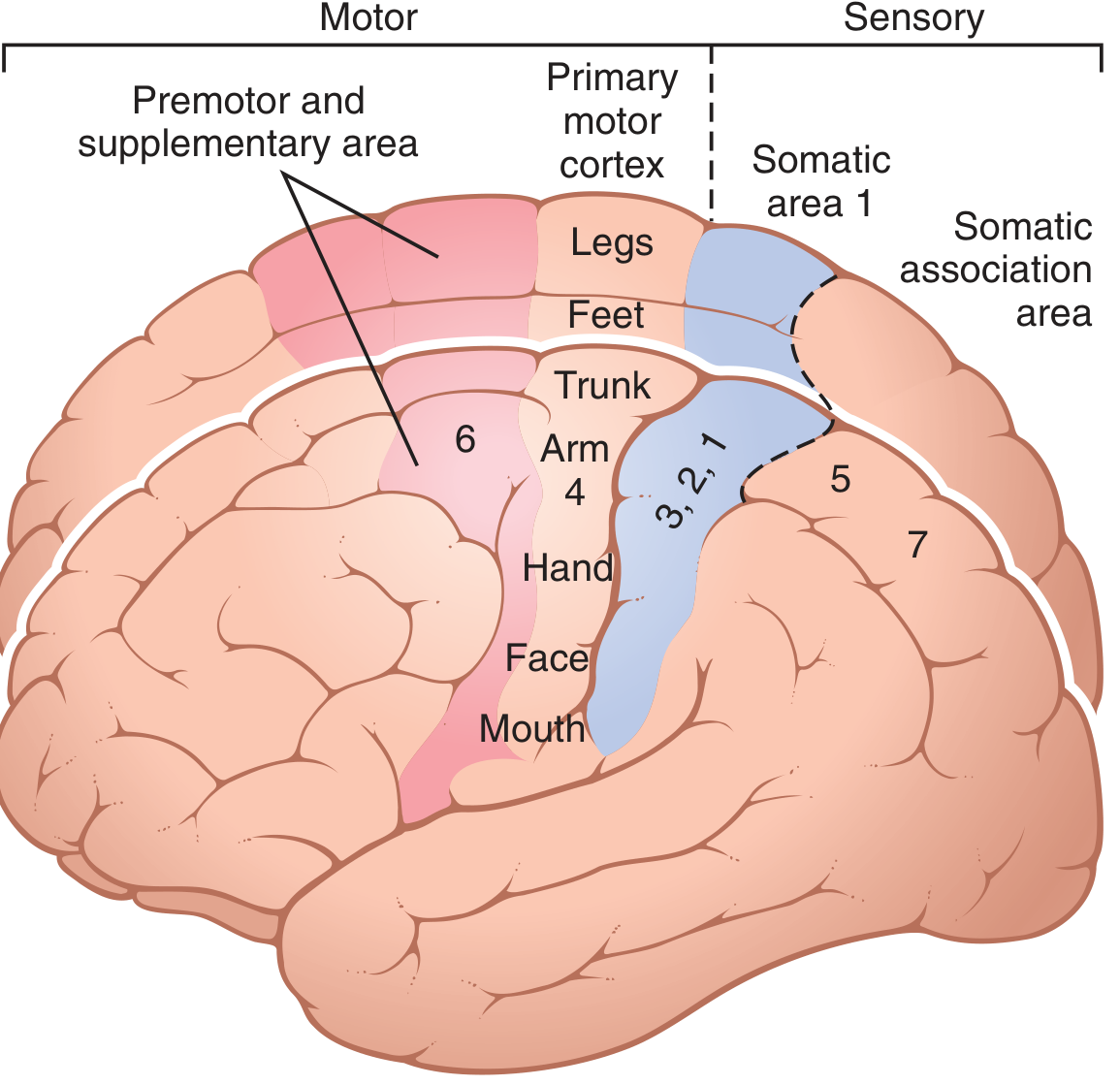
Origin of the Corticospinal (Pyramidal) Tract
- 30% from primary motor cortex (area 4) - Betz cells
- 30% from premotor and supplementary motor areas (area 6)
- 40% from somatosensory cortex (areas 3, 1, 2) posterior to central sulcus
Course of the Lateral Corticospinal Tract
- Arises from motor cortex (precentral gyrus)
- Passes through posterior limb of internal capsule
- Descends through cerebral peduncles (midbrain)
- Forms pyramids of the medulla oblongata
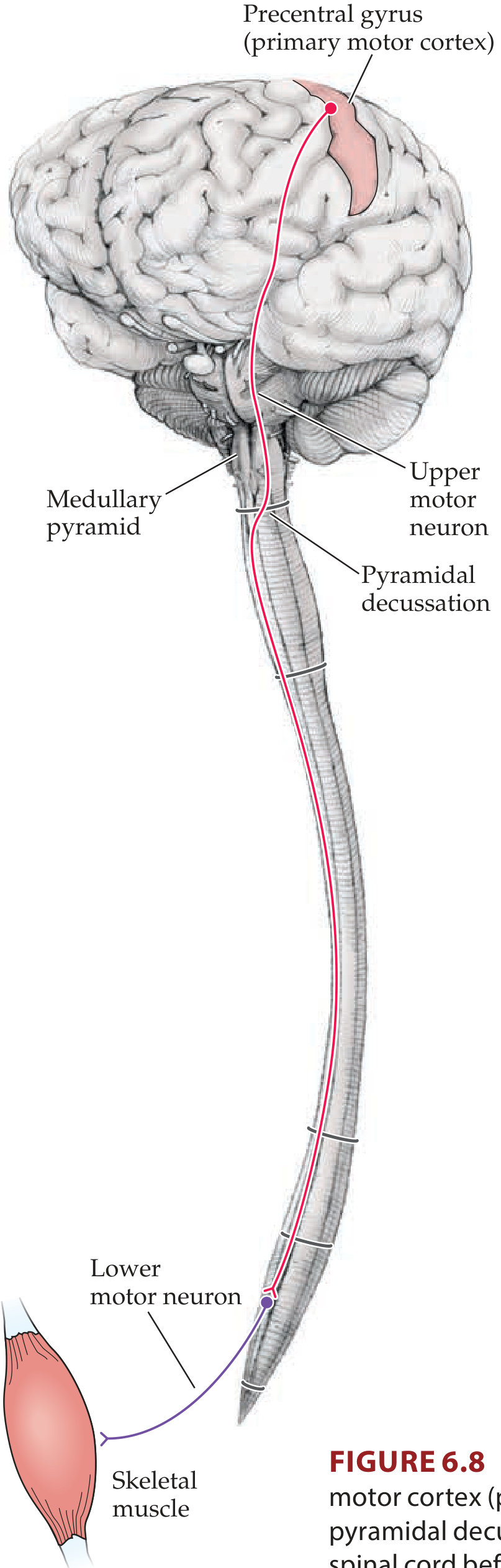
- Crosses (decussates) at the pyramidal decussation - cervicomedullary junction (medulla-spinal cord junction)
- Descends as the lateral corticospinal tract in the lateral funiculus of the spinal cord
- Synapses mainly on interneurons in the intermediate grey matter; some fibers synapse directly on alpha motor neurons
Key point: Because the tract decussates at the pyramidal decussation, a lesion above the decussation causes contralateral weakness; a lesion below the decussation causes ipsilateral weakness.
Betz Cells (Giant Pyramidal Cells)
-
Found only in the primary motor cortex
-
~60 µm in diameter; give rise to the largest myelinated fibers (~16 µm diameter)
-
Conduct at 70 m/sec (fastest signals from brain to cord)
-
Only ~34,000 per corticospinal tract (just 3% of the 1 million total fibers)
-
The other 97% are small fibers (<4 µm) carrying background tonic signals
-
Guyton and Hall, p. 689
Other Descending (Extrapyramidal) Tracts - Also "UMN"
| Tract | Origin | Decussation | Function |
|---|---|---|---|
| Rubrospinal | Red nucleus (midbrain) | Ventral tegmental decussation (midbrain) | Contralateral limb movements |
| Vestibulospinal (lateral) | Lateral vestibular nucleus | None (ipsilateral) | Balance; extensor muscle tone |
| Vestibulospinal (medial) | Medial vestibular nuclei | Bilateral | Head and neck positioning |
| Reticulospinal (pontine) | Pontine reticular formation | None | Facilitates extensors; posture |
| Reticulospinal (medullary) | Medullary reticular formation | None | Inhibits extensors; flexor movements |
| Tectospinal | Superior colliculus | Dorsal tegmental decussation | Head and eye coordination |
| Anterior corticospinal | Motor cortex/SMA | At cervical/thoracic cord level | Bilateral axial/girdle muscles |
These extrapyramidal tracts particularly control postural muscles (medial systems → trunk/proximal muscles; lateral systems → distal limb muscles).
Part 3 - Lower Motor Neuron (LMN)
Definition
Lower motor neurons are the alpha (α) motor neurons located in the anterior horn of the spinal cord grey matter (or motor nuclei of cranial nerves in the brainstem). Their axons exit via ventral nerve roots and travel in peripheral nerves to terminate directly on skeletal muscle fibers at the neuromuscular junction.
Key Facts
- The LMN is the "final common pathway" for all motor commands (Sherrington's term)
- All motor signals - voluntary (corticospinal), reflex (via interneurons), and postural (brainstem) - ultimately converge on the alpha motor neuron
- Each alpha motor neuron + all the muscle fibers it innervates = one motor unit
- LMN also includes gamma motor neurons (innervate intrafusal fibers of muscle spindles)
Part 4 - UMN Lesion vs. LMN Lesion: Complete Comparison
This is the most tested table in neurophysiology:
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Type of paralysis | Spastic (chronic) | Flaccid |
| Muscle tone | Increased (hypertonia, spasticity) | Decreased (hypotonia) |
| Muscle power/weakness | Present (paresis/paralysis) | Present (paresis/paralysis) |
| Muscle wasting/atrophy | Absent (or minimal, disuse) | Marked (denervation atrophy) |
| Fasciculations | Absent | Present (spontaneous firing of denervated motor units) |
| Deep tendon reflexes (DTRs) | Increased (hyperreflexia) | Decreased or absent (hyporeflexia/areflexia) |
| Clonus | Present | Absent |
| Babinski sign (plantar reflex) | Positive (extensor - great toe dorsiflexes, others fan) | Negative (normal flexor response or absent) |
| Abdominal reflexes | Absent | Present (unless LMN to abdominal muscles affected) |
| Cremasteric reflex | Absent | Present |
| Fibrillations (EMG) | Absent | Present |
| Distribution of weakness | Whole limb, contralateral to cortical lesion; distal > proximal | Muscles of specific nerve/root distribution; may be focal |
| Location of lesion | Brain or spinal cord (above anterior horn) | Anterior horn, ventral root, peripheral nerve, NMJ |
| Examples | Stroke, brain tumors, MS, cord compression, spinal cord injury (above anterior horn) | Polio, ALS (LMN component), Guillain-Barré, peripheral neuropathy, motor neuron disease |
Important Nuances
1. Acute UMN Lesion - "Spinal Shock" Phase
When a UMN lesion is acute (e.g., acute stroke, acute cord transection):
- There is initially flaccid paralysis with hypotonia and areflexia - mimicking LMN lesion!
- This is called spinal shock (for spinal cord injury) or cerebral shock (for stroke)
- Over hours to weeks to months, this converts to the classic UMN picture:
- Spasticity develops
- Reflexes become hyperactive
- Babinski sign appears
Key exam trap: A fresh stroke or acute cord injury initially shows flaccid paralysis - only later does spasticity appear.
2. Why Spasticity in UMN Lesion?
Spasticity is not simply due to loss of the corticospinal tract alone. Selective corticospinal tract lesions in experimental animals do not produce spasticity.
The true mechanism: UMN lesions typically damage both the corticospinal tract AND adjacent descending inhibitory pathways (particularly those from the reticular formation and premotor cortex). These inhibitory pathways normally suppress the vestibular and reticular brainstem nuclei. When they are damaged (disinhibited):
-
Vestibulospinal tract fires excessively → enhanced extensor tone
-
Reticulospinal tract activity becomes imbalanced → spasticity
-
Anterior horn cells become hyperexcitable → hyperreflexia
-
Guyton and Hall, p. 692; Neuroanatomy through Clinical Cases, p. 248
3. Why Fasciculations in LMN Lesion?
When the LMN is damaged or degenerating, denervated motor units fire spontaneously and irregularly, producing visible muscle twitches - fasciculations. They represent the random discharges of entire motor units. They are visible on the skin surface and confirmed on EMG.
4. The Babinski Sign - Mechanism
-
Normal (negative): Stroking the lateral sole → all toes plantarflex
-
Positive (UMN lesion): Great toe dorsiflexes (extends) + other toes fan out
-
Physiologically normal in infants (under age 2) because corticospinal tracts are not fully myelinated
-
Mechanism: Loss of cortical inhibitory control over the primitive withdrawal reflex - the dorsiflexion is actually a fragment of the flexor withdrawal pattern; normally suppressed by intact corticospinal projections
-
Ganong's Review of Medical Physiology, p. (Ganong)
5. Pattern of Weakness in UMN Lesion
UMN lesions produce a characteristic pattern of weakness because the corticospinal tract preferentially facilitates certain muscle groups:
- Upper limb: Flexors are relatively preserved; extensors weakened (arm tends to flex)
- Lower limb: Extensors are relatively preserved; flexors weakened (leg tends to extend)
- This produces the classic hemiplegic posture after stroke: arm flexed, leg extended
Part 5 - Descending Tracts Summary
Lateral Motor System (Controls Distal Limb Muscles)
- Lateral corticospinal tract - voluntary fine movements of distal extremities
- Rubrospinal tract - also distal limb movements
Medial Motor System (Controls Proximal/Trunk Muscles and Posture)
- Anterior corticospinal tract - bilateral axial/girdle
- Vestibulospinal tracts - balance and extensor tone
- Reticulospinal tracts - posture and automatic movements
- Tectospinal - head-eye coordination
Part 6 - Clinically Important Conditions
ALS (Amyotrophic Lateral Sclerosis / Lou Gehrig's Disease)
- Selective progressive degeneration of both UMN and LMN
- Shows combined features: weakness + wasting + fasciculations (LMN) + spasticity + hyperreflexia + Babinski (UMN)
- This combination of UMN + LMN signs in the same patient is the hallmark of ALS
- Caused by free radical accumulation (SOD-1 gene mutation in 40% of familial cases)
- Treatment: Riluzole (glutamate release inhibitor) - modestly slows progression
Stroke (Cerebrovascular Accident)
- Most common UMN lesion
- Contralateral hemiplegia/hemiparesis
- Acute phase: flaccid (spinal shock)
- Chronic phase: spastic hemiplegia, hyperreflexia, Babinski positive, clonus
Spinal Cord Hemisection (Brown-Séquard Syndrome)
At the level of the lesion: LMN signs (ipsilateral, segmental)
Below the level of the lesion: UMN signs (ipsilateral, from lateral corticospinal tract damage)
Sensory loss pattern: Ipsilateral proprioception/vibration loss; Contralateral pain/temperature loss
Poliomyelitis
- Selective destruction of anterior horn cells → pure LMN lesion
- Flaccid paralysis, areflexia, muscle wasting, no sensory loss
Part 7 - Quick Memory Aid
UMN lesion = "SHAVE" (Spastic, Hyperreflexia, Absent atrophy, Vivid (brisk) reflexes, Extensor plantar)
LMN lesion = "WAFF" (Wasting, Areflexia, Flaccid, Fasciculations)
Part 8 - Exam-Ready Comparison Diagram
CEREBRAL CORTEX (Motor Strip, Area 4)
|
[UMN Lesion]
= Spastic paralysis
= Hyperreflexia
= Positive Babinski
= No wasting
|
Internal capsule
|
Brainstem → Pyramidal decussation
|
Lateral corticospinal tract
|
ANTERIOR HORN (Spinal cord)
|
[LMN Lesion]
= Flaccid paralysis
= Areflexia
= Muscle wasting
= Fasciculations
= Negative Babinski
|
Peripheral nerve → NMJ → MUSCLE
Sources: Guyton and Hall Textbook of Medical Physiology, pp. 689-692 | Ganong's Review of Medical Physiology, 26th Ed., p. (LMN/UMN section) | Neuroanatomy through Clinical Cases, 3rd Ed., pp. 248-255
UMN and LMN lesions
We just covered UMN and LMN lesions in detail in the previous response! Here's a clean, consolidated summary for quick revision and exam use:
UMN vs LMN Lesions - Complete Revision Summary
The Two-Neuron Motor Chain
MOTOR CORTEX (Area 4 - Precentral Gyrus)
↓
┌─── UPPER MOTOR NEURON ───┐
│ Corticospinal tract │
│ → Internal capsule │ ← UMN LESION HERE
│ → Brainstem pyramids │
│ → Pyramidal decussation │
│ → Lateral CST in cord │
└──────────────────────────┘
↓
ANTERIOR HORN (Spinal Cord)
↓
┌─── LOWER MOTOR NEURON ───┐
│ Alpha motor neuron │ ← LMN LESION HERE
│ → Ventral root │
│ → Peripheral nerve │
│ → NMJ │
└──────────────────────────┘
↓
SKELETAL MUSCLE
The LMN is the "Final Common Pathway" - all motor commands converge here.
Master Comparison Table
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Paralysis type | Spastic (chronic) | Flaccid |
| Muscle tone | Increased (hypertonia) | Decreased (hypotonia) |
| Muscle wasting | Absent (or mild disuse) | Marked (denervation atrophy) |
| Fasciculations | Absent | Present |
| Deep tendon reflexes | Increased (hyperreflexia) | Decreased/Absent (hyporeflexia/areflexia) |
| Clonus | Present | Absent |
| Babinski sign | Positive (extensor plantar) | Negative/Absent |
| Abdominal reflex | Absent | Present |
| Cremasteric reflex | Absent | Present |
| Fibrillations on EMG | Absent | Present |
| Distribution | Whole limb, contralateral body | Focal - follows nerve/root/segment |
| Site of lesion | Brain or spinal cord (above ant. horn) | Ant. horn / root / peripheral nerve / NMJ |
Key Memory Aids
UMN = "SHAB"
- Spastic paralysis
- Hyperreflexia + Hypertonia
- Absent wasting, Absent fasciculations
- Babinski positive
LMN = "WAFF"
- Wasting (muscle atrophy)
- Areflexia
- Flaccid paralysis
- Fasciculations
The Babinski Sign
| Response | Meaning |
|---|---|
| Positive - great toe dorsiflexes, other toes fan out | UMN lesion (abnormal in adults) |
| Negative - all toes plantarflex | Normal |
| Normal in infants (<2 years) | Corticospinal tracts not yet myelinated |
Stimulus: Stroke lateral sole of foot with blunt object from heel toward little toe.
Corticospinal Tract Course (exam essential)
| Level | Event |
|---|---|
| Precentral gyrus | Origin (30% area 4, 30% area 6, 40% sensory cortex) |
| Internal capsule | Passes through posterior limb |
| Cerebral peduncle | Descends through midbrain |
| Basis pontis | Dispersed, reassembles |
| Pyramids (medulla) | Forms pyramid shape |
| Pyramidal decussation | 85-90% cross to opposite side |
| Lateral CST | Descends contralateral spinal cord |
| Anterior horn | Synapses (mainly via interneurons) on alpha motor neurons |
Lesion above decussation → contralateral weakness Lesion below decussation → ipsilateral weakness
Why Spasticity in UMN Lesion?
Spasticity is NOT from corticospinal tract damage alone. It results from damage to adjacent descending inhibitory pathways (reticulospinal, from premotor cortex) that normally suppress the vestibular and reticular brainstem nuclei.
When these inhibitory pathways are damaged:
-
Vestibulospinal tract fires excessively → enhanced extensor tone
-
Anterior horn cells become hyperexcitable → hyperreflexia + spasticity
-
Guyton and Hall, p. 692
Why Flaccidity + Fasciculations in LMN Lesion?
- Flaccidity - Loss of all excitatory input to muscle (no nerve signal at all)
- Atrophy - Muscle loses trophic influence of nerve; undergoes denervation atrophy
- Fasciculations - Damaged/dying motor neurons fire spontaneously and irregularly → visible twitches of whole motor units
- Areflexia - Reflex arc is broken at the efferent limb
Acute UMN Lesion - The Critical Exception
Acutely, UMN lesions produce FLACCID paralysis (not spastic), mimicking LMN:
| Phase | Findings |
|---|---|
| Acute (hours-days) | Flaccid paralysis, hypotonia, areflexia - called Spinal Shock |
| Subacute (weeks) | Reflexes gradually return |
| Chronic (weeks-months) | Classic UMN: spasticity, hyperreflexia, Babinski positive |
Exam trap: A stroke patient on Day 1 will have flaccid paralysis - not spastic!
Pattern of Weakness in Chronic UMN Lesion
Because the corticospinal tract preferentially drives certain muscle groups:
| Limb | Weak muscles | Relatively preserved |
|---|---|---|
| Upper limb | Extensors (triceps, wrist/finger extensors) | Flexors (arm tends to flex) |
| Lower limb | Flexors (hip flexors, dorsiflexors) | Extensors (leg tends to extend/stiffen) |
This produces the classic hemiplegic posture after stroke:
- Arm: adducted, internally rotated, elbow flexed, wrist/fingers flexed
- Leg: extended, circumducted during walking
Important Clinical Conditions
| Disease | UMN | LMN | Key Feature |
|---|---|---|---|
| Stroke (CVA) | ✓ | ✗ | Contralateral hemiplegia; acute flaccid → chronic spastic |
| Spinal cord injury | ✓ (below lesion) | ✓ (at level) | Spinal shock initially |
| ALS | ✓ | ✓ | BOTH UMN + LMN signs in same patient = hallmark |
| Poliomyelitis | ✗ | ✓ | Pure anterior horn destruction; no sensory loss |
| Multiple sclerosis | ✓ | ✗ | Demyelination of CNS white matter |
| Guillain-Barré | ✗ | ✓ | Peripheral nerve demyelination; ascending flaccid paralysis |
| Myasthenia gravis | ✗ | ✓ (NMJ) | Fatigable weakness; anti-AChR antibodies |
| Brown-Séquard | ✓ ipsilateral below | ✓ at level ipsilateral | Ipsilateral UMN + contralateral pain/temp loss |
ALS - Special Case (Both UMN + LMN)
ALS (Lou Gehrig's disease) destroys both UMN and LMN simultaneously:
| Signs from LMN loss | Signs from UMN loss |
|---|---|
| Muscle wasting | Spasticity |
| Fasciculations | Hyperreflexia |
| Flaccid weakness | Babinski positive |
| Areflexia in some areas | Clonus |
Treatment: Riluzole (blocks glutamate release, modestly slows progression); Baclofen for spasticity (GABA-B agonist); Botulinum toxin also used for spasticity.
Brown-Séquard Syndrome (Spinal Cord Hemisection)
A perfect example to test UMN/LMN understanding:
| Finding | Side | Level |
|---|---|---|
| LMN signs (flaccid, areflexia, wasting) | Ipsilateral | At the level of lesion |
| UMN signs (spastic, hyperreflexia, Babinski) | Ipsilateral | Below the level |
| Loss of proprioception/vibration | Ipsilateral | Below level |
| Loss of pain/temperature | Contralateral | Below level (crosses within 1-2 segments) |
Quick Reflexes Reference
| Reflex | Spinal Level | Present in UMN lesion? | Present in LMN lesion? |
|---|---|---|---|
| Biceps jerk | C5-C6 | Exaggerated | Absent |
| Triceps jerk | C7-C8 | Exaggerated | Absent |
| Knee jerk | L3-L4 | Exaggerated | Absent |
| Ankle jerk | S1-S2 | Exaggerated + clonus | Absent |
| Plantar (Babinski) | S1-S2 | Extensor (positive) | Flexor (normal) or absent |
| Abdominal reflex | T8-T12 | Absent | Present |
| Cremasteric | L1-L2 | Absent | Present |
Sources: Guyton and Hall Textbook of Medical Physiology, pp. 689-692 | Ganong's Review of Medical Physiology, 26th Ed. | Neuroanatomy through Clinical Cases, 3rd Ed., pp. 248-255
Corticospinal tracks
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent images retrieved. Now let me compile the comprehensive answer.
Corticospinal Tract (Pyramidal Tract)
Overview
The corticospinal tract (CST) is the principal voluntary motor pathway of the nervous system. It is also called the pyramidal tract because its fibers form the pyramids on the ventral surface of the medulla oblongata. It carries motor commands from the cerebral cortex directly to alpha motor neurons (or their interneurons) in the spinal cord, enabling fine, skilled, voluntary movements - especially of the distal extremities (hands, fingers).
Origin
The corticospinal tract arises from three cortical areas:
| Cortical Origin | Contribution | Area (Brodmann) |
|---|---|---|
| Primary motor cortex (precentral gyrus) | 30% | Area 4 |
| Premotor + Supplementary Motor Area | 30% | Area 6 |
| Somatosensory cortex (postcentral gyrus) | 40% | Areas 3, 1, 2 |
The somatosensory contribution (40%) modulates sensory input to the spinal cord - these fibers synapse on dorsal horn neurons and regulate incoming sensory information.
Betz Cells (Giant Pyramidal Cells)
-
Found only in the primary motor cortex (area 4)
-
Cell body diameter: ~60 µm (largest neurons in the CNS)
-
Axon diameter: ~16 µm (largest myelinated fibers in the CST)
-
Conduction velocity: 70 m/sec (fastest from brain to cord)
-
Number: only ~34,000 per tract (= just 3% of the 1 million total fibers)
-
The remaining 97% of fibers are small (<4 µm), carrying background tonic motor signals
-
Guyton and Hall, p. 689
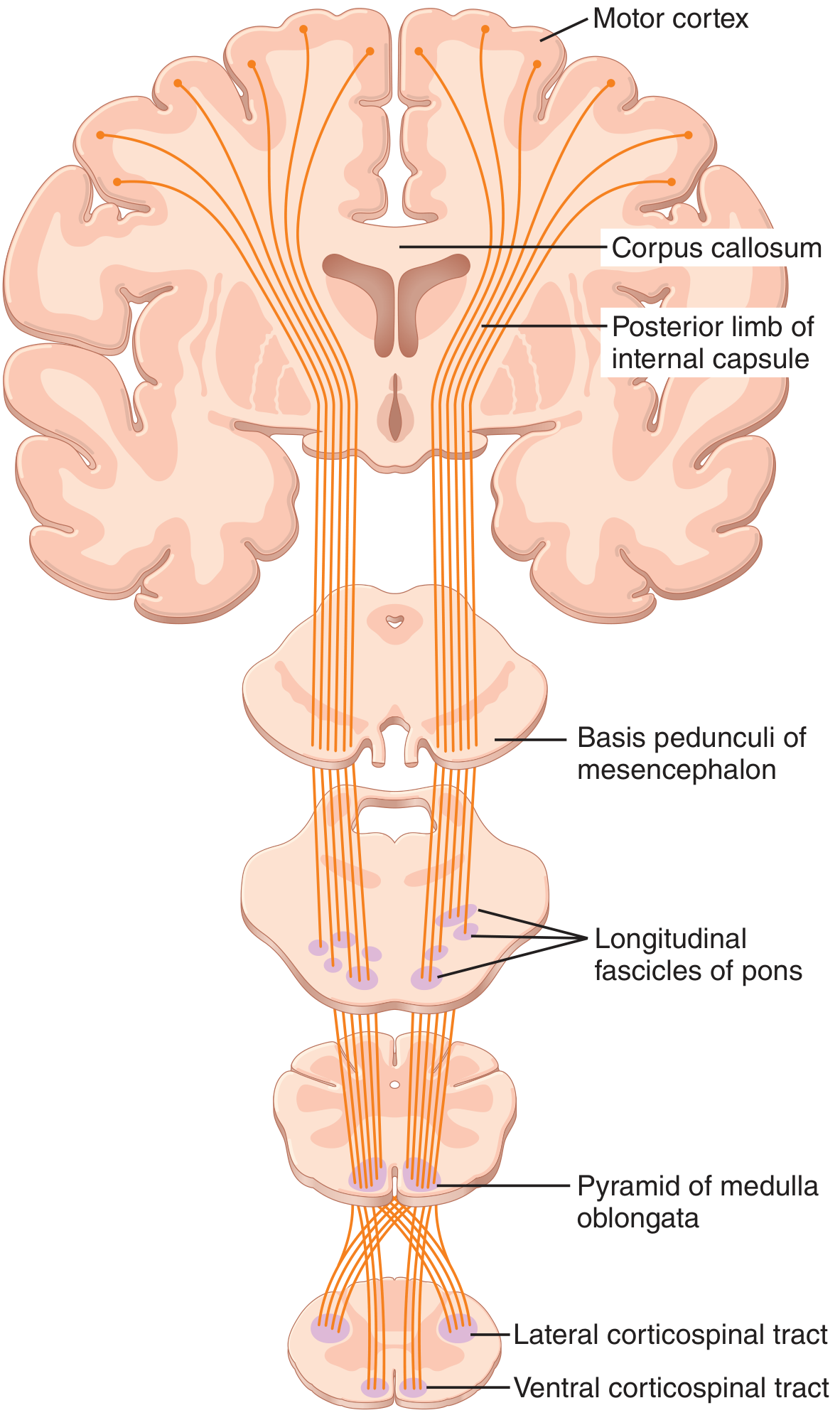
Complete Course - Step by Step
Step 1 - Cerebral Cortex → Corona Radiata
- Axons from motor cortex enter the corona radiata (fan-shaped white matter of cerebral hemisphere)
- All motor, sensory, and association fibers converge downward toward the internal capsule
Step 2 - Internal Capsule (Posterior Limb)
- CST fibers pass through the posterior limb of the internal capsule (between the caudate nucleus and the lentiform nucleus - putamen + globus pallidus)
- Somatotopic arrangement in internal capsule:
- Face fibers: most anterior (near genu)
- Arm fibers: middle of posterior limb
- Trunk: slightly posterior
- Leg fibers: most posterior
- Hand fibers: lateral and slightly anterior to foot fibers
- This is why a small internal capsule stroke (lacunar infarct) can cause dense contralateral hemiplegia - all the fibers are tightly packed here
Step 3 - Cerebral Peduncles (Midbrain)
- Fibers descend into the basis pedunculi (ventral portion of cerebral peduncle)
- In the cerebral peduncles: Face medial → Arm → Trunk → Leg lateral
- Corticobulbar fibers (to cranial nerve nuclei) travel alongside CST here
Step 4 - Pons (Basis Pontis)
- Fibers disperse into scattered fascicles as pontocerebellar fibers cross transversely
- Fibers are separated by transverse pontine fibers and pontine nuclei
- Somatotopic organization is maintained - fibers controlling proximal muscles are more dorsal
Step 5 - Medullary Pyramids
- Fascicles reconverge on the ventral surface of the medulla to form the medullary pyramids (two prominent bulges)
- This is where the tract gets the name "pyramidal tract"
- In the pyramids: lower extremity fibers are more lateral; upper extremity fibers more medial
Step 6 - PYRAMIDAL DECUSSATION (Most Critical Point)
- At the cervicomedullary junction (foramen magnum level, where medulla meets spinal cord)
- ~85-90% of fibers cross to the opposite side - this is the pyramidal decussation (also called Mistichelli's crossing)
- Lower extremity fibers decussate more rostrally; upper extremity fibers decussate slightly more caudally
- This decussation is why cortical lesions produce contralateral weakness
Step 7 - Lateral Corticospinal Tract (in Spinal Cord)
- The 85-90% of crossed fibers descend in the lateral funiculus (lateral white matter column) as the lateral corticospinal tract
- Somatotopic arrangement: Upper limb fibers medial, lower limb fibers lateral (clinically relevant in central cord syndrome)
- Fibers terminate at all spinal levels but predominantly at cervical and lumbosacral enlargements (for limb control)
- Most fibers synapse on interneurons in the intermediate grey (Rexed laminae V-VIII)
- Some fibers synapse directly on alpha motor neurons in the anterior horn (especially for fine hand movements)
- A few synapse on sensory relay neurons in the dorsal horn (sensory modulation)
Step 8 - Anterior Corticospinal Tract (in Spinal Cord)
- The ~15% of uncrossed fibers descend ipsilaterally in the anterior funiculus as the anterior corticospinal tract (Türck's bundle)
- These fibers eventually cross at cervical and upper thoracic spinal levels via the anterior white commissure
- Control bilateral axial and girdle (proximal) muscles
- Only about 2% of all corticospinal fibers remain truly ipsilateral throughout their course (Bundle of Barnes - controls trunk muscles)
Summary Table: Two Divisions of the CST
| Feature | Lateral CST | Anterior CST |
|---|---|---|
| Proportion | ~85-90% | ~15% |
| Decussation site | Pyramidal decussation (medulla) | At each spinal level (anterior commissure) |
| Location in cord | Lateral funiculus | Anterior funiculus |
| Muscles controlled | Contralateral distal limb muscles | Bilateral axial/proximal muscles |
| Clinical importance | Primary voluntary motor control | Postural/truncal movements |
Somatotopic Organization at Each Level
| Level | Arrangement |
|---|---|
| Motor cortex | Face lateral → Arm → Trunk → Leg medial (into longitudinal fissure) |
| Internal capsule | Face anterior → Arm → Trunk → Leg posterior |
| Cerebral peduncle | Face medial → Arm → Trunk → Leg lateral |
| Lateral CST (cord) | Upper limb medial → Lower limb lateral |
This somatotopy is clinically critical for lesion localization.
Termination in the Spinal Cord
The CST axons synapse at different levels:
| Target | Proportion | Function |
|---|---|---|
| Interneurons (laminae V-VIII) | Majority | Most voluntary commands pass via interneurons to motor neurons |
| Alpha motor neurons directly (lamina IX) | Minority | Direct monosynaptic drive; critical for fine distal movements |
| Sensory dorsal horn neurons (laminae I-IV) | Some | Modulate incoming sensory signals - "sensory gating" |
The direct cortico-motoneuronal connections (monosynaptic) are most developed in primates and are essential for independent finger movements. Damage to these produces loss of fine dexterity even without complete paralysis.
Corticobulbar Tract (Companion Pathway)
The corticobulbar tract runs parallel to the CST but terminates on cranial nerve motor nuclei (not spinal anterior horn). Key points:
- Travels in genu of internal capsule (CST is in posterior limb)
- Most cranial nerve nuclei receive bilateral corticobulbar input (from both hemispheres)
- Exception: The lower face (below orbicularis oculi) nucleus of CN VII receives predominantly contralateral input
- Clinical consequence: A UMN (cortical/internal capsule) lesion causes:
- Contralateral lower face weakness (central facial palsy)
- Forehead spared (bilateral upper face input preserved)
- This is different from peripheral (LMN) CN VII palsy which affects the entire ipsilateral face
Functions of the Corticospinal Tract
- Voluntary skilled movement - especially fine, precise, distal movements (hand/finger dexterity)
- Speed of movement - Betz cell fibers provide the fastest signal to the cord
- Fractionation of movement - ability to move individual fingers independently (requires direct cortico-motoneuronal connections)
- Sensory modulation - dorsal horn fibers gate incoming sensory information during movement
- Facilitation of spinal reflexes - provides tonic facilitory drive to anterior horn cells
Lesion Localization - Effect at Each Level
| Site of Lesion | Side of Weakness |
|---|---|
| Motor cortex | Contralateral |
| Internal capsule | Contralateral |
| Cerebral peduncle (midbrain) | Contralateral |
| Basis pontis | Contralateral |
| Medullary pyramid (above decussation) | Contralateral |
| Pyramidal decussation | Ipsilateral (rare "cruciate paralysis") |
| Spinal cord (below decussation) | Ipsilateral |
Pure Pyramidal Tract Lesion vs. CST Lesion in Stroke
An important distinction:
- A pure corticospinal tract lesion (e.g., selective pyramid lesion) causes contralateral weakness with hypotonia and hyporeflexia - NOT spasticity
- Spasticity requires additional damage to adjacent reticulospinal and other descending inhibitory pathways
- In clinical strokes, both CST and adjacent pathways are damaged simultaneously → classic UMN syndrome with spasticity
Clinical Correlates by Level
| Level | Lesion | Features |
|---|---|---|
| Motor cortex | Stroke/tumor | Contralateral monoplegia or hemiplegia; arm and face affected more than leg if MCA territory |
| Internal capsule | Lacunar infarct (small vessel) | Dense pure motor hemiplegia (entire contralateral body - face, arm, leg equally) because all fibers tightly packed |
| Brainstem | Crossed syndromes (e.g., Weber's) | Ipsilateral CN palsy + contralateral hemiplegia (CN affected at brainstem level; CST already descending) |
| Spinal cord | Compression, MS | Ipsilateral UMN signs below the level |
| Bilateral CST | ALS, MS | Spastic paraplegia or quadriplegia |
Weber's Syndrome (Classic Crossed Syndrome - Midbrain)
- Lesion in the midbrain cerebral peduncle
- Ipsilateral CN III palsy (ptosis, mydriasis, "down and out" eye)
- Contralateral hemiplegia (CST damage before decussation)
Key Facts for MCQs
| Fact | Answer |
|---|---|
| Origin of CST | 30% area 4, 30% area 6, 40% sensory cortex |
| Betz cell diameter | 60 µm |
| Betz cell axon diameter | 16 µm |
| Betz cell conduction velocity | 70 m/sec |
| Total CST fibers | >1 million per tract |
| Betz cell fibers (%) | 3% |
| Site of decussation | Pyramidal decussation (cervicomedullary junction) |
| Proportion that crosses | ~85-90% |
| Lateral CST location in cord | Lateral funiculus |
| Anterior CST location in cord | Anterior funiculus |
| Primary function | Fine voluntary movement, distal limb dexterity |
| Internal capsule - CST location | Posterior limb |
| Corticobulbar - internal capsule | Genu |
Sources: Guyton and Hall Textbook of Medical Physiology, pp. 281-292 | Neuroanatomy through Clinical Cases, 3rd Ed., pp. 255-260 | Localization in Clinical Neurology, 8th Ed., pp. 27-28
This is a shared conversation. Sign in to Orris to start your own chat.