Renal biopsy indication,take reference of standard textbook including harrison
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive data from multiple authoritative textbooks. Let me compile the full, well-structured answer.
Renal Biopsy: Indications, Contraindications, and Pre-Procedure Assessment
Overview
Renal biopsy has become a fundamental component of modern clinical nephrology. It changes patient management in up to 74% of cases and reveals unsuspected diagnostic information in two-thirds of patients. There are no universally binding formal guidelines, but accepted indications are well-defined across textbooks.
- Brenner and Rector's The Kidney, Box 26.1 / Chapter 26
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 55
- Goldman-Cecil Medicine, Ch. 100
Indications for Renal Biopsy
From Brenner & Rector's The Kidney (Box 26.1) - The Standard Reference
The four cardinal indications are:
| # | Indication |
|---|---|
| 1 | Significant proteinuria (>1 g/day or protein-to-creatinine ratio >100 mg/mmol) |
| 2 | Microscopic hematuria with any degree of proteinuria |
| 3 | Unexplained renal impairment (native or transplant kidney) |
| 4 | Renal manifestations of systemic disease |
Detailed Breakdown by Clinical Scenario
1. Nephrotic Syndrome
- Adults with idiopathic nephrotic syndrome - biopsy is almost always indicated (Goldman-Cecil).
- Children: Biopsy is generally reserved for:
- Steroid-resistant nephrotic syndrome (SRNS) - near-universal agreement
- Steroid-dependent nephrotic syndrome (in some centers)
- Infants (age <1 year) with nephrotic syndrome - early biopsy recommended
- Persistent elevated serum creatinine, hypocomplementemia, or gross hematuria alongside nephrotic syndrome
- Children who fail initial empiric steroid therapy
- Before starting calcineurin inhibitors (cyclosporine, tacrolimus) to establish baseline scarring
- Biopsy is not routinely indicated during the first episode of acute nephrotic syndrome in children (Tintinalli's).
2. Glomerulonephritis / Hematuria
- RBC casts in urine = indication for early renal biopsy (Harrison's 22E). RBC casts have critical implications for diagnosis, prognosis, and treatment.
- Hematuria without RBC casts can also indicate glomerular disease - phase contrast microscopy for dysmorphic RBCs ("acanthocytes") helps refine this.
- Microscopic hematuria with any degree of proteinuria = biopsy indication (Brenner).
3. Acute Kidney Injury (AKI)
- AKI without an identifiable inciting cause - a clear indication (Goldman-Cecil).
- Notable exception: Hospital-acquired kidney failure rarely meets this threshold.
- AKI in specific settings (e.g., suspected rapidly progressive GN, vasculitis, allergic interstitial nephritis with eosinophilia) warrants urgent biopsy.
- Atheroembolic renal failure: Biopsy can confirm diagnosis but is often unnecessary when other stigmata are present (Harrison's 22E).
4. Systemic Disease with Renal Involvement
- Lupus nephritis - biopsy required to classify histological class (I-VI), which guides immunosuppressive therapy (Firestein's Rheumatology, Brenner).
- Repeat biopsy indicated when there is increased disease activity or change in histologic class.
- Vasculitis (ANCA-associated, anti-GBM disease) - biopsy for classification and severity assessment.
- Henoch-Schonlein Purpura / IgA vasculitis - when hypertension, hematuria, or proteinuria present.
- Diabetic nephropathy - biopsy rarely required UNLESS another cause is suspected (Goldman-Cecil). Kimmelstiel-Wilson nodular glomerulosclerosis is the classic finding but seen in only ~25% of cases.
5. Chronic Kidney Disease (CKD) of Unknown Cause
- Unexplained CKD warrants biopsy - important to exclude treatable causes.
- Full exome genetic testing also has ~20% diagnostic yield in CKD of unknown cause and complements (does not replace) biopsy.
6. Transplant Kidney
- Unexplained deterioration of transplant function - biopsy for rejection classification.
- For management of BK virus nephropathy (threshold: viruria 4-6 log₁₀ on serum testing, then biopsy considered).
Contraindications
Absolute Contraindications
- Uncontrollable bleeding diathesis / uncorrectable coagulopathy
- Uncooperative patient (inability to lie still / follow breath-hold instructions)
- Solitary functioning kidney (relative - open/laparoscopic approach preferred)
- Renal neoplasm / cyst at biopsy site
- Active urinary tract infection (UTI)
- Severe uncontrolled hypertension (BP ≥160/100 mm Hg significantly doubles bleeding risk)
Relative Contraindications
- Thrombocytopenia or prolonged clotting time (can be corrected with FFP, platelets, or DDAVP)
- Hemoglobin <11 g/dL (transfuse to >10 g/dL prior to procedure)
- Solitary kidney (prefer open/laparoscopic approach)
- Small echogenic kidneys (advanced CKD - biopsy yield low, risk:benefit unfavorable)
- Anatomical abnormalities / horseshoe kidney (CT-guided or open biopsy preferred)
- Recent NSAID use (e.g., naproxen within 24 hours)
- Pregnancy after 32 weeks (increased bleeding risk - biopsy complications significantly higher postpartum)
Pre-Biopsy Assessment (Biopsy Flowchart - Brenner & Rector)
Before proceeding to percutaneous biopsy, the following must be confirmed:
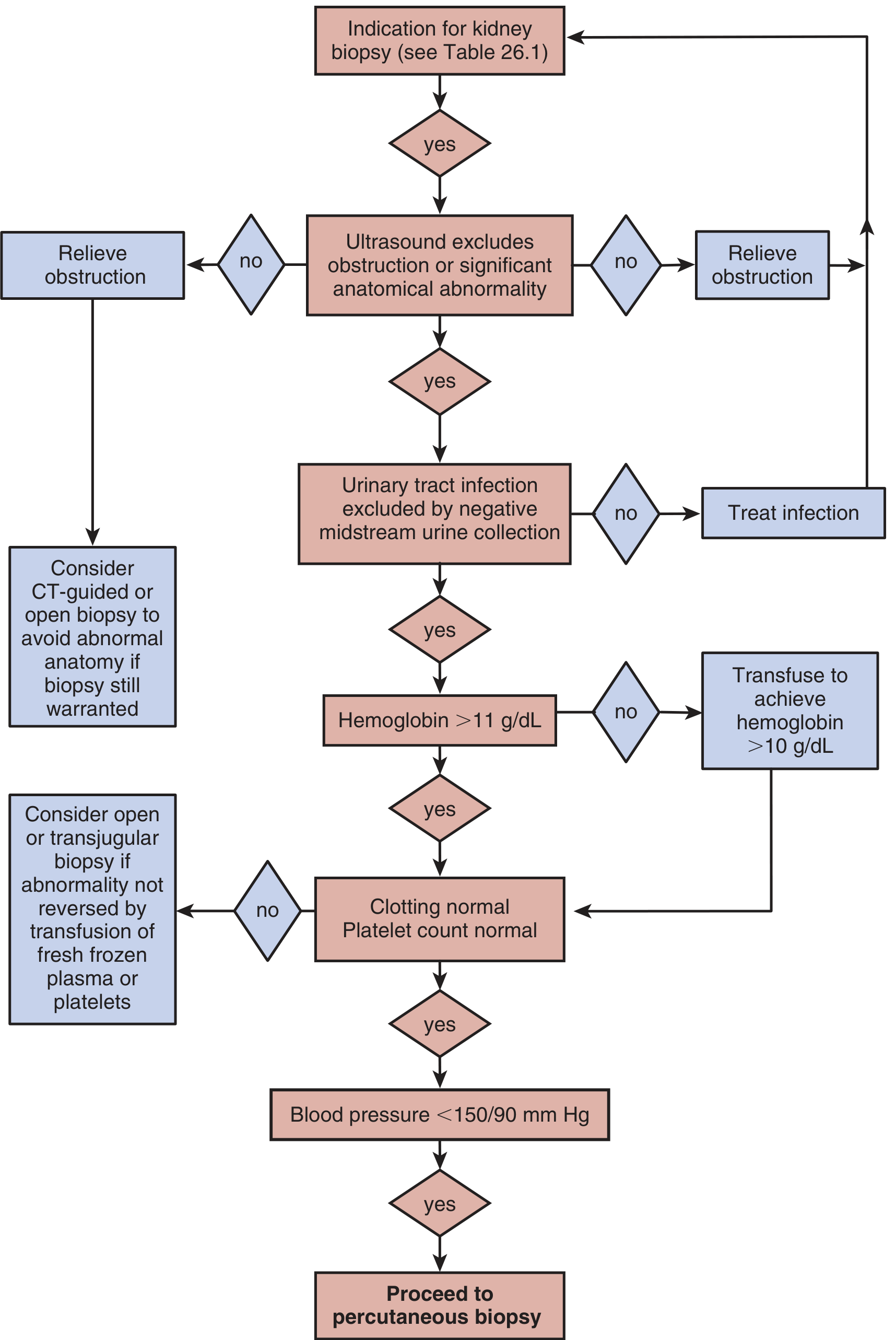
- Ultrasound excludes obstruction or significant anatomical abnormality
- UTI excluded by negative midstream urine culture (treat infection first if present)
- Hemoglobin >11 g/dL (transfuse to achieve >10 g/dL if not met)
- Clotting normal, platelet count normal (correct with FFP/platelets if abnormal; consider transjugular/open biopsy if uncorrectable)
- Blood pressure <150/90 mmHg (control hypertension first)
- If all above met → Proceed to percutaneous biopsy
Alternative Biopsy Approaches
| Method | Indications | Disadvantages |
|---|---|---|
| Transjugular | Bleeding diathesis, ventilated patients, combined liver-renal biopsy | Risk of capsular perforation; inadequate tissue in up to 24% |
| Open surgical | Solitary kidney, abnormal anatomy, high bleeding risk | General/spinal anesthesia required; longer recovery |
| Laparoscopic | Abnormal anatomy, high bleeding risk | General anesthesia required; longer recovery |
Complications of Renal Biopsy
- Overall complication rate: 3.5-13% (majority minor)
- Bleeding: ~50% of patients have a hemoglobin drop post-biopsy; ~1/3 develop hematoma
- Significant bleeding requiring intervention: ≤7%
- Transfusion rate (without coagulopathy): ~1-2% (Goldman-Cecil)
- Arteriovenous fistula: usually asymptomatic, spontaneously resolves
- Sepsis: rare
- Mortality: <0.2% (from uncontrolled hemorrhage in largest series)
- DDAVP (0.3 mcg/kg SC) may reduce post-biopsy bleeding complications, particularly in lower-risk patients
Post-Biopsy Observation
- Minimum 6-8 hours bed rest
- Overnight stay recommended: identifies 85-95% of complications at 12 hours, 89-98% at 24 hours
- Monitor: BP, pulse, urine color for hematuria
Summary Table: Indications at a Glance
| Clinical Presentation | Biopsy Indicated? | Notes |
|---|---|---|
| Adult idiopathic nephrotic syndrome | Yes | Standard practice |
| Child steroid-resistant NS | Yes | Near-universal consensus |
| Child first episode NS | No (usually) | Empiric steroids first |
| AKI without identified cause | Yes | Clear indication |
| Hospital-acquired AKI | Rarely | Usually identifiable cause |
| RBC casts in urine | Yes (urgent) | Glomerulonephritis/vasculitis |
| Hematuria + proteinuria | Yes | Any degree of proteinuria |
| Lupus nephritis | Yes | For histological classification |
| Diabetic nephropathy | Rarely | Only if atypical features |
| Unexplained CKD | Yes | Exclude treatable causes |
| Transplant dysfunction | Yes | Rejection classification |
References:
- Brenner and Rector's The Kidney, 2-Volume Set - Box 26.1, Chapter 26 (Salama & Cook)
- Harrison's Principles of Internal Medicine 22E (2025) - Chapter 55 (Intrinsic Renal Disease / Hematuria approach)
- Goldman-Cecil Medicine, International Edition - Chapter 100 (Renal Biopsy)
- Comprehensive Clinical Nephrology, 7th Edition
- Smith and Tanagho's General Urology, 19th Edition
USG thyroid scoring detail, TiRaD
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a complete, authoritative answer with the full ACR TI-RADS scoring system, the beautiful chart images, and comprehensive textbook content. Let me compile the full response.
Thyroid Ultrasound Scoring: TI-RADS (Thyroid Imaging Reporting and Data System)
What is TI-RADS?
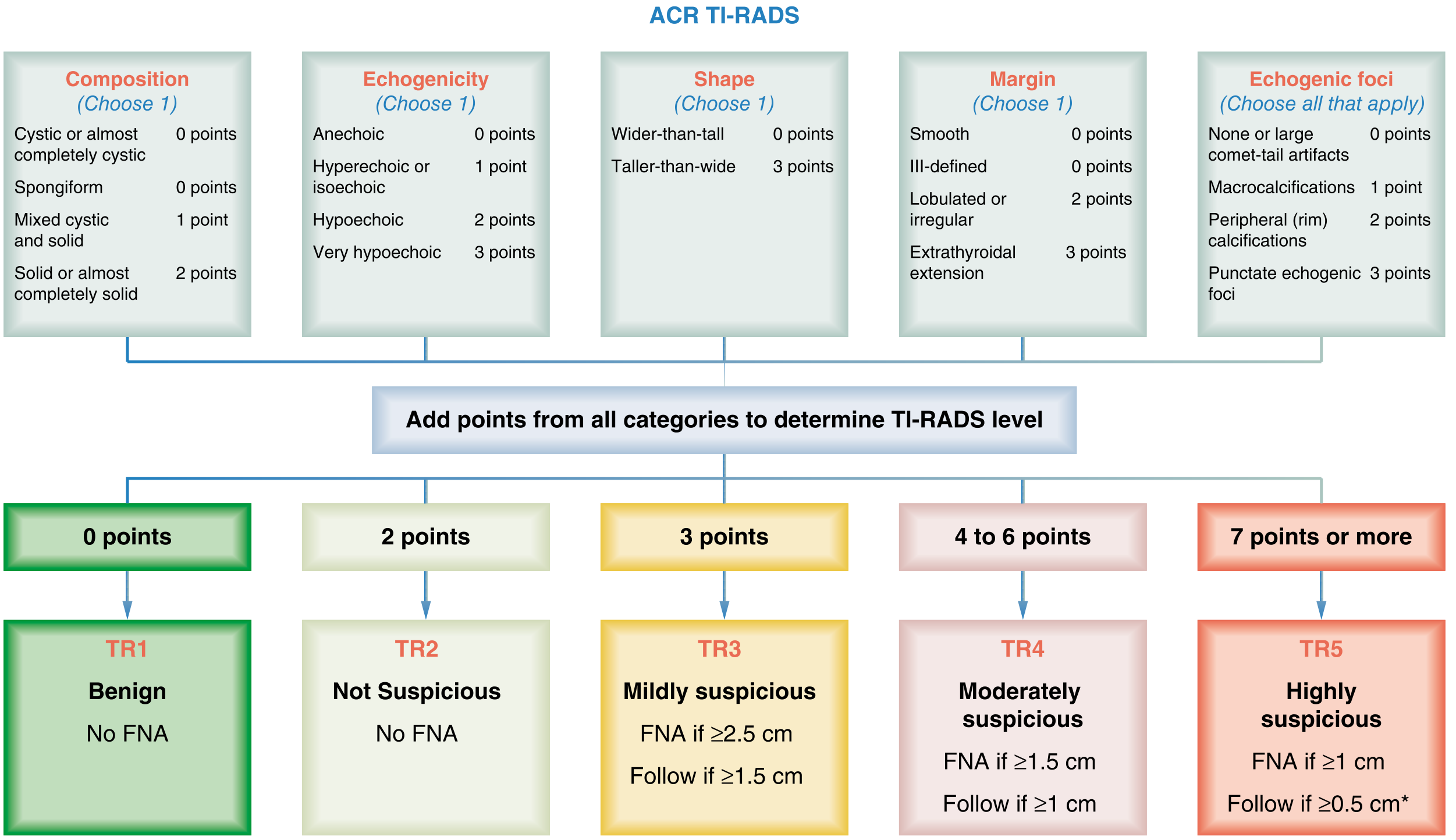
The Thyroid Imaging Reporting and Data System (TI-RADS) is a structured ultrasound reporting system that assigns thyroid nodules a risk category to guide the decision of whether to perform Fine Needle Aspiration (FNA) biopsy. The most widely used version in the United States is the ACR TI-RADS (American College of Radiology), published in 2017 by Tessler et al. (J Am Coll Radiol. 2017;14:587-595).
All validated risk stratification systems reduce unnecessary FNAs by at least 45%, in part due to the recommendation not to perform FNA for spongiform nodules. - Harrison's Principles of Internal Medicine 22E (2025)
ACR TI-RADS: The Point-Based Scoring System
ACR TI-RADS scores a nodule across 5 categories. Points from all 5 categories are summed to determine the TR level.
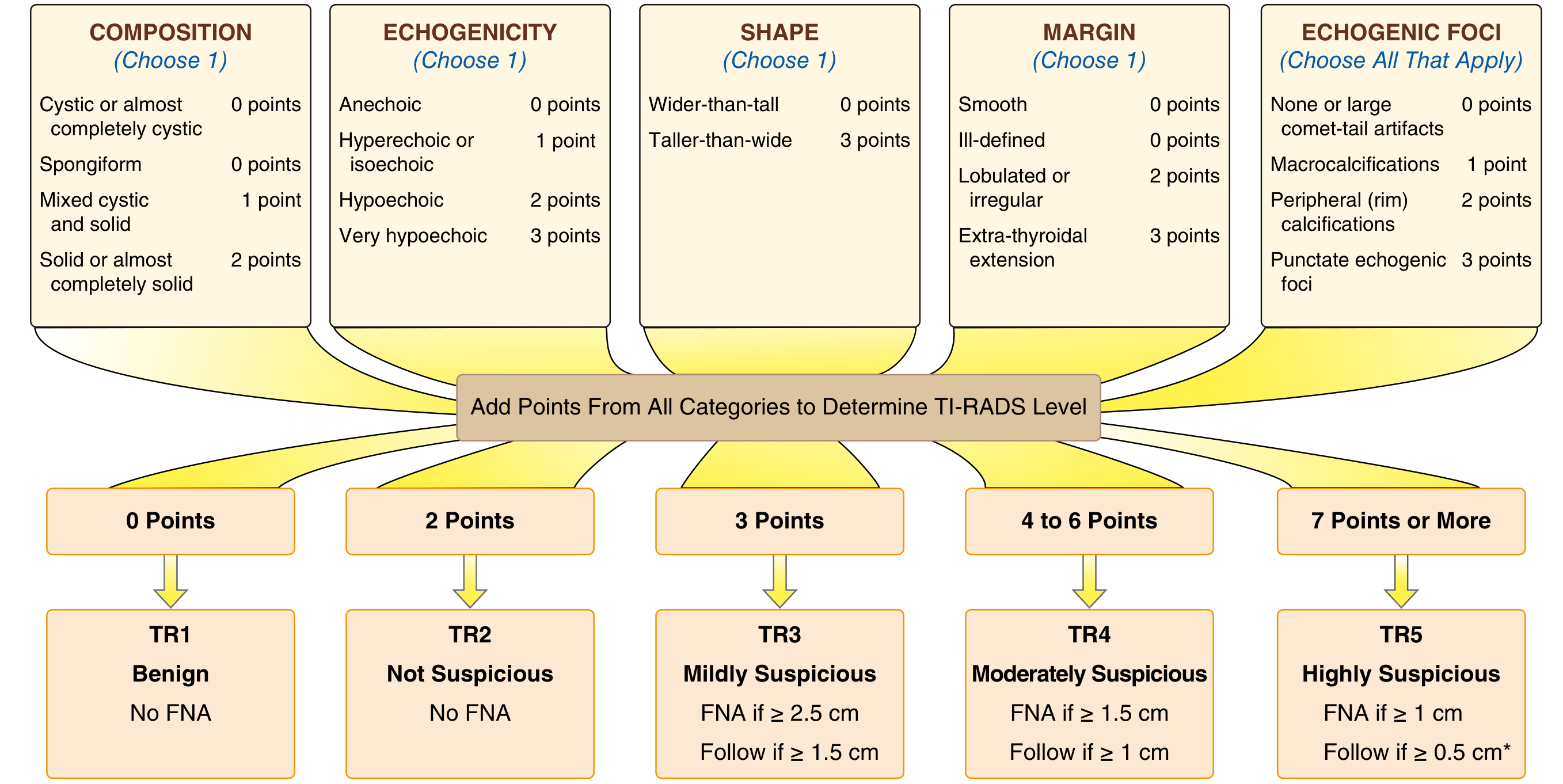
Category 1: COMPOSITION (Choose ONE)
| Finding | Points |
|---|---|
| Cystic or almost completely cystic | 0 |
| Spongiform (>50% small cystic spaces) | 0 |
| Mixed cystic and solid | 1 |
| Solid or almost completely solid | 2 |
Key notes:
- Spongiform: If a nodule is spongiform, stop here - do NOT add further points from other categories
- Assign 2 points if composition cannot be determined due to calcification
Category 2: ECHOGENICITY (Choose ONE)
| Finding | Points |
|---|---|
| Anechoic (for cystic/almost completely cystic) | 0 |
| Hyperechoic or isoechoic | 1 |
| Hypoechoic (compared to adjacent parenchyma) | 2 |
| Very hypoechoic (more hypoechoic than strap muscles) | 3 |
Assign 1 point if echogenicity cannot be determined
Category 3: SHAPE (Choose ONE)
| Finding | Points |
|---|---|
| Wider-than-tall | 0 |
| Taller-than-wide | 3 |
Assessment: Measured on transverse image - height parallel to sound beam, width perpendicular. Usually assessable by visual inspection.
Category 4: MARGIN (Choose ONE)
| Finding | Points |
|---|---|
| Smooth | 0 |
| Ill-defined | 0 |
| Lobulated or irregular (jagged, spiculated, sharp angles) | 2 |
| Extrathyroidal extension | 3 |
- Lobulated = protrusions into adjacent tissue
- Extrathyroidal extension (obvious invasion) = strong indicator of malignancy
- Assign 0 points if margin cannot be determined
Category 5: ECHOGENIC FOCI (Choose ALL that apply)
| Finding | Points |
|---|---|
| None, or large comet-tail artifacts (V-shaped >1 mm in cystic component) | 0 |
| Macrocalcifications (cause acoustic shadowing) | 1 |
| Peripheral (rim) calcifications (complete or incomplete along margin) | 2 |
| Punctate echogenic foci (may have small comet-tail artifacts) | 3 |
This is the only multi-select category - add points for each echogenic focus type present
TI-RADS Level Classification (TR1-TR5)
| TR Level | Total Points | Category | FNA Recommendation |
|---|---|---|---|
| TR1 | 0 | Benign | No FNA |
| TR2 | 2 | Not Suspicious | No FNA |
| TR3 | 3 | Mildly Suspicious | FNA if ≥2.5 cm; Follow if ≥1.5 cm |
| TR4 | 4-6 | Moderately Suspicious | FNA if ≥1.5 cm; Follow if ≥1 cm |
| TR5 | 7 or more | Highly Suspicious | FNA if ≥1 cm; Follow if ≥0.5 cm* |
*For TR5 nodules 5-9 mm (papillary microcarcinomas), refer to specific papillary microcarcinoma management guidelines.
Key Lexicon Definitions
| Feature | Definition |
|---|---|
| Spongiform | Composed predominantly (>50%) of small cystic spaces |
| Very hypoechoic | More hypoechoic than the strap (neck) muscles |
| Taller-than-wide | AP diameter > transverse diameter on axial image |
| Irregular margin | Jagged, spiculated, or sharp angulated edges |
| Macrocalcifications | Large calcifications causing posterior acoustic shadowing |
| Peripheral/rim calcifications | Complete or incomplete calcification along nodule margin |
| Punctate echogenic foci | Tiny bright spots, may have small comet-tail artifacts (microcalcifications) |
| Large comet-tail artifacts | V-shaped reverberation artifacts >1 mm in cystic spaces (benign, colloid) |
Ultrasound Features Suspicious for Malignancy
From Cummings Otolaryngology (Box 114.1):
- Microcalcifications (punctate echogenic foci)
- Absence of peripheral halo
- Irregular border
- Hypoechoic / very hypoechoic texture
- Taller than wide on transverse imaging
- Marked intranodular vascularity on color Doppler
- Extrathyroidal extension
ATA (American Thyroid Association) Risk Stratification - Companion System
The ATA uses pattern-based (not point-based) risk stratification (Goldman-Cecil, Table 207-7):
| ATA Pattern | Sonographic Features | Malignancy Risk | FNA Threshold |
|---|---|---|---|
| High suspicion | Solid hypoechoic + one or more of: irregular margins, microcalcifications, taller-than-wide, rim calcification with soft tissue component, ETE | 70-90% | ≥1 cm |
| Intermediate suspicion | Hypoechoic solid nodule, smooth margins, no microcalcifications/ETE/taller-than-wide | 10-20% | ≥1 cm |
| Low suspicion | Isoechoic or hyperechoic solid nodule, or partially cystic with eccentric solid area, no suspicious features | 5-10% | ≥1.5 cm |
| Very low suspicion | Spongiform or partially cystic, no suspicious features | <3% | >2 cm or observe |
| Benign | Purely cystic (no solid component) | <1% | No biopsy |
"The American Thyroid Association system is based on ultrasonographic patterns, unlike ACR TI-RADS which is based on a point system." - Goldman-Cecil Medicine
European TI-RADS (EU-TIRADS) - Brief Overview
EU-TIRADS classifies nodules into 5 categories similar to ACR but uses a simpler qualitative approach without point assignment. All systems have been shown to reduce unnecessary FNAs by at least 45% compared to no structured criteria (Harrison's 22E).
Workflow: How to Use TI-RADS Clinically
Thyroid nodule detected (palpation or incidental imaging)
↓
Measure TSH
↓ (if TSH suppressed) → Radionuclide scan → Hot nodule → No FNA needed
↓ (TSH normal or elevated)
Thyroid ultrasound with TI-RADS scoring
↓
Assign TR1-TR5 based on point total
↓
TR1/TR2: Observe, no biopsy
TR3: FNA if ≥2.5 cm
TR4: FNA if ≥1.5 cm
TR5: FNA if ≥1 cm
↓
FNA result → Bethesda classification (I-VI) guides surgery/observation
Additional Points from Harrison's 22E
- ACR TI-RADS is the most widely used RSS in the United States
- A spongiform nodule (TR1) has <3% chance of cancer - observation recommended
- 10-20% of solid hypoechoic nodules with smooth borders (TR4) are malignant
- No RSS recommends routine FNA for any nodule <1 cm unless metastatic cervical lymph nodes are present
- Thyroid nodules are present in up to 50% of individuals >50 years on ultrasound
- 18FDG-PET hypermetabolic thyroid nodules carry ~35% malignancy risk and should be biopsied if ≥1 cm (Goldman-Cecil)
References:
- Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill) - Chapter 397: Thyroid Nodules
- Goldman-Cecil Medicine, International Edition - Chapter 207: Thyroid / ACR TIRADS section (citing Tessler et al. 2017)
- Sabiston Textbook of Surgery, 8th Edition - Chapter 73 (Fig. 73.16)
- Cummings Otolaryngology Head and Neck Surgery - Box 114.1
- Tietz Textbook of Laboratory Medicine, 7th Edition - Imaging the Thyroid
- Tessler FN et al. ACR TI-RADS White Paper. J Am Coll Radiol. 2017;14:587-595.
This is a shared conversation. Sign in to Orris to start your own chat.