hernia .. (elaborate)
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hernia" AND "repair"
Searching Images
hernia types anatomy inguinal femoral umbilical
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have everything needed for a comprehensive, well-illustrated answer. Here it is:
Hernia — Comprehensive Overview
Definition
A hernia is the protrusion of any viscus (or part of it) from its normal cavity through an abnormal opening. In abdominal hernias, intraabdominal contents — usually bowel or omentum — protrude through a defect in the musculoaponeurotic abdominal wall.
"Hernias can develop along a congenital tract that fails to close (e.g., indirect inguinal or umbilical hernias), or along an area of weakness in the muscular and fascial layers (e.g., direct inguinal, ventral, or incisional hernias). This weakness may be the result of aging and the accompanying loss of tissue elasticity, increased intraabdominal pressure, failure of proper healing, or trauma." — Roberts and Hedges' Clinical Procedures in Emergency Medicine
Epidemiology
- Hernias develop in approximately 5% of men and 2% of women
- 75% of all abdominal hernias occur in the groin
- Hernias have been recognized and treated since 1550 BC
Anatomy of a Hernia
Every hernia has three components:
| Component | Description |
|---|---|
| Sac | A diverticulum of peritoneum with a neck, body, and fundus |
| Contents | Bowel (enterocele), omentum (epiplocele/omentocele), bladder (cystocele), or other viscera |
| Coverings | The layers of abdominal wall through which the hernia passes |
Classification
By Reducibility
| Type | Definition |
|---|---|
| Reducible | Contents return spontaneously or with gentle pressure |
| Irreducible / Incarcerated | Contents cannot be returned to the abdomen; no vascular compromise |
| Obstructed | Bowel within the sac is obstructed but not yet strangulated |
| Strangulated | Blood supply to the hernia contents is compromised — a surgical emergency |
| Richter's hernia | Only part of the bowel wall (anti-mesenteric side) is incarcerated; complete obstruction may be absent |
By Etiology
- Congenital — due to a pre-formed peritoneal sac (e.g., patent processus vaginalis in indirect inguinal hernia)
- Acquired — due to progressive weakness of the abdominal wall (e.g., direct inguinal hernia, incisional hernia)
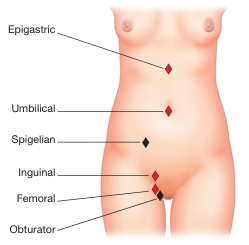
Anatomical Types
1. Inguinal Hernia
The most common hernia, accounting for ~75% of all hernias. Far more common in males.
Indirect (Oblique) Inguinal Hernia
- Comprises >80% of inguinal hernias
- The hernia passes through the deep inguinal ring, which lies lateral to the inferior epigastric vessels
- Follows the inguinal canal obliquely, can descend all the way into the scrotum along the processus vaginalis
- Two subtypes:
- Congenital — patent processus vaginalis (the funicular process fails to obliterate after testicular descent); reaches the scrotal bottom quickly
- Acquired — no pre-formed sac; progresses gradually
- Extent classification: Bubonocele (within canal) → Incomplete (through superficial ring, not reaching scrotum) → Complete (reaches bottom of scrotum)
Direct (Medial) Inguinal Hernia
- Always acquired; more common in elderly patients
- Protrudes through Hesselbach's triangle (bounded medially by rectus abdominis, laterally by inferior epigastric vessels, below by inguinal ligament)
- Wall at this point consists only of transversalis fascia + external oblique aponeurosis
- Broadly based → unlikely to strangulate
- Spherical shape; little tendency to enter scrotum
- The bladder can be pulled into a direct hernia
Pantaloon (Saddle-bag) Hernia
- Simultaneous presence of both direct and indirect hernias straddling the inferior epigastric vessels
- Difficult to reduce in the ED; often discovered at surgical exploration
European Hernia Society Classification
- Primary (P) or Recurrent (R)
- Lateral (L), Medial (M) or Femoral (F)
- Defect size in fingerbreadths (<1.5 cm = 1; 1.5–3 cm = 2; >3 cm = 3)
2. Femoral Hernia
- Protrusion inferior to the inguinal ligament through a defect in transversalis fascia
- Contents enter the femoral canal — the space medial to the femoral vein, lateral to the lacunar ligament
- More common in women (female-to-male ~10:1)
- The small fascial defect means it incarcerates in up to 40–45% of cases — highest strangulation risk of all groin hernias
- Presents as a medial thigh mass below the inguinal ligament (below and lateral to the pubic tubercle)
- All femoral hernias should be urgently referred for surgical repair — Tintinalli's
3. Umbilical Hernia
- Traverses the fibromuscular ring at the umbilicus
- In infants: usually closes spontaneously by age 2–3; if persistent or symptomatic, surgical repair is indicated
- In adults: associated with obesity, pregnancy, ascites, chronic raised intra-abdominal pressure
- Incarceration of small bowel or omentum is common; strangulation occurs in ~1/3 of umbilical hernias — Goldman-Cecil Medicine
- Mesh repair is preferred over suture repair
4. Incisional Hernia
- Occurs in up to 1 in 5 patients after abdominal surgery
- Poor wound healing, infection, and obesity predispose
- Carries a recurrence rate of 20–50% after repair
- Larger defects paradoxically have a lower incarceration risk (wider neck)
5. Epigastric Hernia
- Protrudes through the linea alba, between xiphisternum and umbilicus
- Usually contains pre-peritoneal fat; rarely contains bowel
- Complications (pancreatitis, bowel strangulation) are rare but reported
6. Spigelian Hernia
- Occurs at the Spigelian fascia — the lateral border of the rectus abdominis, at or below the arcuate line
- Interparietal: lies between muscle layers, so it may not produce a visible external swelling
- Risk of incarceration is significant due to the tight fascial ring
7. Obturator Hernia
- Passes through the superolateral aperture of the obturator foramen (where obturator vessels and nerve exit)
- Predominantly affects elderly, thin women
- Hausmann's sign: pain referred to the inner thigh (along the obturator nerve)
- Richter's type incarceration is common; diagnosis often delayed → high mortality
8. Hiatal Hernia
- Part of the stomach herniates through the esophageal hiatus of the diaphragm
- Types:
- Type I (Sliding): GEJ and fundus slide upward; most common; associated with GERD
- Type II (Rolling/Paraesophageal): GEJ remains in place; fundus herniates alongside esophagus
- Type III (Mixed): Both GEJ and fundus herniate
- Type IV: Other abdominal organs (colon, spleen) also herniate
9. Internal Hernias
Herniation through mesenteric or peritoneal defects inside the abdominal cavity:
- Paraduodenal hernia (most common internal hernia)
- Hernia through the foramen of Winslow (posterior to porta hepatis)
- Mesenteric window hernias
- Particularly important in post-bariatric surgery patients (Roux limb, Petersen's space, mesocolic window)
Clinical Features
History
- Groin/abdominal mass that appears on standing, coughing, or straining; reduces on lying down
- Aching/dragging discomfort; referred pain to scrotum, testis, or inner thigh
- Sudden pain + irreducibility → strangulation until proven otherwise
Examination
- Patient examined standing first, then supine
- Indirect hernia: pyriform shape, stalk at external inguinal ring, extends to scrotum; reduces obliquely
- Direct hernia: spherical; pushes directly forward; rarely enters scrotum
- Cough impulse: transmits expansile impulse to the examining finger in the inguinal canal
- Inguinal occlusion test: blocking the deep ring with a finger prevents indirect hernia from descending on coughing; direct hernia still protrudes
- Percussion: resonant (enterocele) vs. dull (epiplocele/omentocele)
Key Differential Diagnoses (groin bulge)
Lymph nodes, lymphoma, lipoma of cord, hydrocele, varicocele, ectopic/undescended testis, femoral artery aneurysm, psoas abscess
Complications
| Complication | Description |
|---|---|
| Irreducibility | Contents cannot be reduced; common in femoral, obturator |
| Incarceration/Obstruction | Bowel obstructed within sac |
| Strangulation | Vascular compromise; pain, tenderness, systemic toxicity |
| Recurrence | After surgical repair; highest with suture repair (20–50% incisional) |
| Chronic pain | Most common complication of open flat mesh repair |
"For years, surgeons have been taught that all hernias should be repaired at diagnosis to prevent a hernia accident, which is defined as a bowel obstruction or incarceration with strangulation." — Mulholland & Greenfield's Surgery
Treatment
Emergency Management (ED)
- Determine: truly a hernia? Reducible? Strangulated?
- Easily reducible → discharge for elective repair
- Incarcerated → attempt careful manual reduction (Trendelenburg position + gentle sustained pressure)
- Strangulated → surgical emergency; do not attempt reduction — risk of reducing gangrenous bowel
Surgical Options
Herniotomy
- Children with indirect hernia: simply excise and ligate the sac (high ligation at deep ring)
- In adults: herniotomy alone has high recurrence — herniorrhaphy required
Open Suture Repair
- Bassini repair (1890): approximates conjoint tendon to inguinal ligament — the foundation of hernia surgery for 100 years
- Shouldice repair: transversalis fascia opened and double-breasted; expert centres report <2% lifetime failure; technically demanding
- Maloney darn: continuous non-absorbable suture darned between conjoint tendon and inguinal ligament; most common in resource-limited settings
- Desarda repair: uses a strip of external oblique aponeurosis as a natural tissue reinforcement
Open Flat Mesh Repair — Lichtenstein
- Gold standard for elective inguinal hernia repair in adults
- Polypropylene mesh laid flat over the posterior wall of the inguinal canal, sutured to inguinal ligament and conjoint tendon
- Lower recurrence than suture repair at 2 years
- Main complication: chronic inguinodynia (nerve entrapment)
Laparoscopic Repair
- TAPP (Transabdominal Pre-Peritoneal): enters peritoneal cavity, places mesh in preperitoneal space
- TEP (Totally Extraperitoneal): entirely preperitoneal approach, avoids peritoneal entry

A 2024 Cochrane meta-analysis (PMID 38963034) comparing TAPP vs. TEP found no significant difference in outcomes. Robotic-assisted ventral hernia repair also shows comparable outcomes to laparoscopic repair per a 2025 systematic review (PMID 39966282).
| Approach | Advantages | Disadvantages |
|---|---|---|
| Open (Lichtenstein) | Simple, low cost, local anaesthesia possible | Higher chronic pain rate |
| Laparoscopic (TEP/TAPP) | Faster recovery, less chronic pain, bilateral repair in one sitting | Steeper learning curve, general anaesthesia required |
Mesh in Emergency Repair
- Contaminated field or bowel resection → avoid permanent synthetic mesh; use tissue repair, reserve mesh for recurrence
Paediatric Hernia
- High-ligation technique (no mesh in young children)
- Bilateral exploration may be warranted due to high rate of contralateral patent processus vaginalis
Special Hernia Variants
| Variant | Feature |
|---|---|
| Sliding hernia | Retroperitoneal organ (sigmoid colon on left, caecum on right) forms part of the sac wall itself — beware during dissection |
| Littre's hernia | Contains Meckel's diverticulum |
| Maydl's hernia | Two loops of bowel in sac with the connecting loop inside the abdomen (W-hernia); strangulation of the intra-abdominal segment |
| Richter's hernia | Only anti-mesenteric bowel wall incarcerated; no complete obstruction but high risk of silent strangulation |
| Amyand's hernia | Appendix within the hernia sac |
| De Garengeot hernia | Appendix within a femoral hernia sac |
Key Anatomical Danger Zones (Laparoscopic Surgery)
- Triangle of Doom: bounded by vas deferens medially and testicular vessels laterally → contains external iliac vessels → no staples/clips here
- Triangle of Pain: lateral to testicular vessels → contains genitofemoral nerve and lateral femoral cutaneous nerve → avoid dissection
Summary
| Hernia Type | Site | Common in | Strangulation Risk | Key Feature |
|---|---|---|---|---|
| Indirect inguinal | Deep ring, lateral to IEA | All ages, males | Moderate | Patent processus vaginalis in young |
| Direct inguinal | Hesselbach's triangle | Elderly males | Low (broad neck) | Always acquired |
| Femoral | Femoral canal | Women | Very high (40–45%) | Below inguinal ligament |
| Umbilical | Umbilical ring | Infants, obese adults | High in adults | Strangulation in ~1/3 |
| Incisional | Previous surgical scar | Post-op patients | Variable with size | 20% after any laparotomy |
| Hiatal | Esophageal hiatus | Adults | Low | GERD, reflux |
| Obturator | Obturator foramen | Elderly thin women | High | Inner thigh pain (Hausmann) |
| Spigelian | Lateral rectus border | Middle-aged | Moderate | May be occult (interparietal) |
Sources: Bailey and Love's Short Practice of Surgery 28th Ed. | S Das Manual on Clinical Surgery 13th Ed. | Roberts and Hedges' Clinical Procedures in Emergency Medicine | Mulholland and Greenfield's Surgery 7th Ed. | Schwartz's Principles of Surgery 11th Ed. | Goldman-Cecil Medicine | Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.