Explain hypovolemic shock
Reading File
Finding Sources
Searching PubMed
"hypovolemic shock" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material to write a thorough, well-organized answer. Let me compile it.
Hypovolemic Shock
Hypovolemic shock is the most common form of shock encountered in surgical and emergency practice. It occurs when a reduction in intravascular volume falls to a level where the heart can no longer pump sufficient blood to meet the metabolic demands of vital organs. More than 20% of circulating blood volume must typically be lost before the full syndrome develops.
Definition & Core Mechanism
The fundamental derangement is reduced preload - less blood returning to the right heart - which, by the Frank-Starling mechanism, causes a fall in cardiac output. Since mean arterial pressure (MAP) = cardiac output × total peripheral resistance (TPR), falling cardiac output produces hypotension and tissue hypoperfusion.
MAP falls → inadequate oxygen delivery → anaerobic metabolism → lactic acidosis → organ dysfunction.
- Guyton and Hall Textbook of Medical Physiology, p. 299
Causes
Hemorrhagic (most common):
- Trauma, gastrointestinal bleeding, ruptured aortic aneurysm, obstetric hemorrhage
Non-hemorrhagic:
- Plasma loss: severe burns (loss through denuded skin), intestinal obstruction (capillary leak into bowel wall), peritonitis ("third spacing")
- Total body fluid depletion: severe vomiting/diarrhea, excessive sweating, osmotic diuresis (DKA), adrenal insufficiency (loss of aldosterone-driven Na/water reabsorption)
- Traumatic: capillary disruption from tissue contusion even without overt hemorrhage
Note: plasma loss carries an additional complication - the increased red cell concentration raises blood viscosity, further impairing microvascular flow. - Guyton and Hall, p. 304
Compensatory (Neurohormonal) Responses
When arterial pressure falls, three major compensatory arms are activated simultaneously:
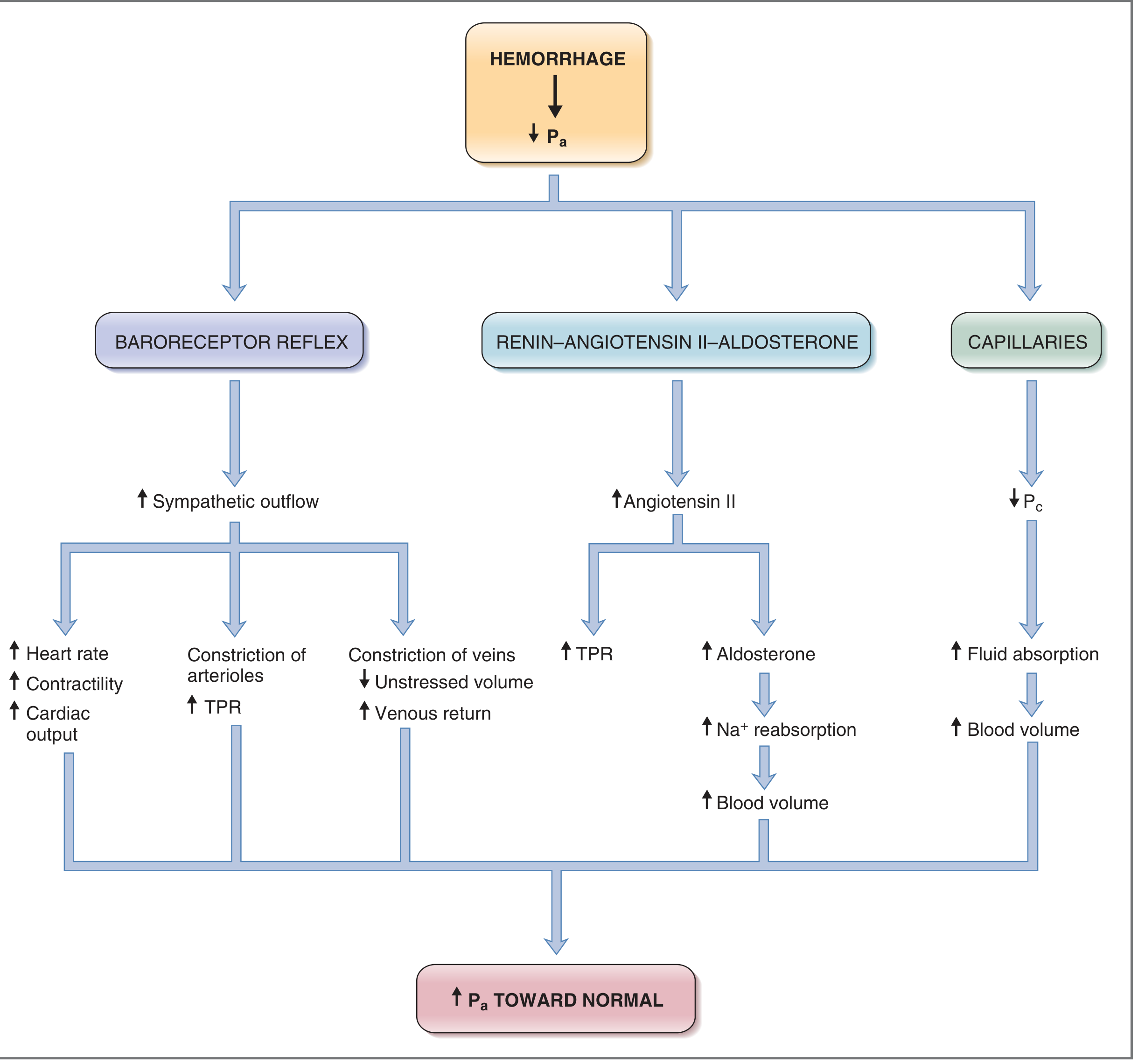
1. Baroreceptor Reflex (Rapid - seconds)
- Aortic arch and carotid sinus baroreceptors detect the fall in stretch
- Increased sympathetic outflow → tachycardia, increased myocardial contractility, arteriolar vasoconstriction (↑TPR), and venous constriction (↓unstressed volume, ↑venous return)
- Coronary and cerebral vessels are spared from sympathetic constriction - their autoregulation protects flow down to ~70 mmHg MAP
2. Renin-Angiotensin-Aldosterone System (Minutes to hours)
- Renal hypoperfusion → renin release → angiotensin II → peripheral vasoconstriction + aldosterone release → renal Na⁺ and water retention → gradual blood volume restoration
3. Capillary Fluid Shift (Hours)
- Fall in capillary hydrostatic pressure (Pc) favors reabsorption of interstitial fluid into the vascular compartment, helping restore blood volume
4. ADH / Vasopressin
- Released from posterior pituitary in response to low blood pressure and increased plasma osmolality → renal free water retention + mild vasoconstriction
5. CNS Ischemic Response ("Last Stand")
- When MAP falls below ~50 mmHg, the ischemic brainstem triggers extreme sympathetic discharge - visible as the "second plateau" on arterial pressure recordings
These reflexes extend survivable blood loss from ~15-20% (without reflexes) to ~30-40% (with intact reflexes). - Guyton and Hall, p. 300
ATLS Classification of Hemorrhagic Shock
| Class | Blood Loss | Volume (70 kg adult) | Clinical Features | Treatment |
|---|---|---|---|---|
| I | up to 15% | up to ~750 mL | No measurable changes; normal cap refill | Self-correcting; minimal treatment |
| II | 15-30% | 800-1,500 mL | Tachycardia, tachypnea, narrowed pulse pressure, mild anxiety, reduced UO (20-30 mL/hr) | Crystalloid; some may need blood |
| III | 30-40% | up to ~2,000 mL | Marked tachycardia, hypotension, confusion/combativeness, delayed cap refill | Crystalloid + blood transfusion |
| IV | >40% | >2,000 mL | Life-threatening; severe tachycardia, very low BP, cold/pale skin, negligible UO, depressed mental status | Immediate transfusion + surgical/interventional hemorrhage control |
Class III is the minimum loss that consistently produces systolic hypotension. - Mulholland & Greenfield's Surgery, p. 530-531
Individual susceptibility varies with age, pregnancy, beta-blocker use, pre-existing disease, and other poorly characterized factors.
Progressive vs. Non-progressive Shock
This is one of the most important distinctions:
- Nonprogressive (compensated) shock: Blood loss below a critical threshold. Compensatory mechanisms are sufficient; the patient gradually recovers with treatment.
- Progressive shock: Blood loss exceeds a critical threshold (arterial pressure falls below ~45 mmHg in experimental models). Shock itself generates more shock in a vicious cycle:
- Cardiac ischemia → reduced contractility
- Tissue acidosis → vascular smooth muscle unresponsiveness
- Capillary stasis → microthrombi formation (DIC)
- Intestinal ischemia → bacterial translocation and endotoxin release
- Irreversible shock: So much cellular and organ damage has accumulated that even restoration of normal blood volume cannot prevent death.
Clinical Features (Summary)
| System | Signs |
|---|---|
| Cardiovascular | Tachycardia, hypotension, narrowed pulse pressure, weak pulses |
| Skin | Cool, pale, clammy; delayed capillary refill |
| Renal | Oliguria or anuria (UO < 0.5 mL/kg/hr) |
| Neurological | Anxiety → confusion → combativeness → obtundation → coma |
| Respiratory | Tachypnea (compensating for metabolic acidosis) |
| Labs | Metabolic acidosis, elevated lactate, rising BUN/creatinine, hemoconcentration (in plasma loss) |
Hemodynamic profile: low CO, high SVR - this is a "cold shock." - Sabiston Textbook of Surgery, p. 2886
Treatment Principles
Hemorrhagic Shock
- Control the source of bleeding (surgical, endovascular, or procedural) - this is the definitive step
- Two large-bore IV lines (14-16G antecubital); intraosseous access if venous access fails
- Permissive hypotension before hemorrhage control (target MAP ~50 mmHg in penetrating trauma to avoid clot dislodgement) - but maintain higher pressures with TBI
- Blood products - in hemorrhagic shock, crystalloids alone worsen anemia and dilutional coagulopathy:
- 1:1:1 ratio - fresh frozen plasma : packed red blood cells : platelets (massive transfusion protocol, or MTP)
- Whole blood - emerging evidence suggests superiority over component therapy when available
- Viscoelastic testing (TEG or ROTEM) - can guide targeted component replacement; may offer mortality benefit in massive transfusion (>10 units pRBC)
- Tranexamic acid (TXA) - stabilizes clot by inhibiting fibrinolysis; should be given within 3 hours of injury (CRASH-2 trial data); adult dose 1g IV over 10 min, then 1g over 8 hours
- Vasopressors (norepinephrine, vasopressin) - a temporizing measure only, not a substitute for volume; vasopressin-deficient state may respond specifically to vasopressin
Non-hemorrhagic Hypovolemic Shock
- Crystalloid resuscitation (lactated Ringer's or normal saline) is the primary treatment
- Adult: 1-2L bolus and reassess; pediatric: 20 mL/kg bolus, repeat once, then 10 mL/kg pRBC if no improvement
- Identify and treat the underlying cause (vomiting, diarrhea, burns, etc.)
Monitoring Resuscitation Endpoints
- Urine output ≥0.5 mL/kg/hr (adult), ≥1 mL/kg/hr (child)
- Normalization of lactate and base deficit
- MAP ≥65 mmHg
- Heart rate returning to normal
Sources
- Mulholland & Greenfield's Surgery, 7th ed., pp. 530-533
- Guyton and Hall Textbook of Medical Physiology, pp. 299-305
- Costanzo Physiology, 7th ed., pp. 186-188
- Sabiston Textbook of Surgery, pp. 2886-2894
- Rosen's Emergency Medicine, pp. 2207-2223
Recent evidence note: A 2025 systematic review (PMID 40603759) confirmed point-of-care ultrasound (POCUS) has good diagnostic accuracy for differentiating shock types, supporting its use in early evaluation of suspected hypovolemic shock.
This is a shared conversation. Sign in to Orris to start your own chat.