
IMG_2776.jpg
Explain me about each and everything in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Here is a full, detailed breakdown of every topic on your Neuroscience Syllabus:
🧠 Neuroscience Syllabus - Complete Explanation
1. Receptors & Pathways → Pyramidal vs. Extrapyramidal (Spinothalamic)
Pyramidal Tract
The pyramidal tract (corticospinal + corticobulbar tracts) is the primary voluntary motor pathway. Neurons originate in the motor cortex, travel through the internal capsule, pass through the medullary pyramids (giving the tract its name), and synapse on lower motor neurons (LMN) in the spinal cord anterior horn. It controls fine, skilled, voluntary movement.
- Corticospinal tract: controls limb movements
- Corticobulbar tract: controls facial/tongue/throat muscles via cranial nerve nuclei
Extrapyramidal Tract
The extrapyramidal system does NOT pass through the medullary pyramids. It includes the rubrospinal, pontine reticulospinal, medullary reticulospinal, tectospinal, and vestibulospinal tracts. It is heavily influenced by the basal ganglia and cerebellum and regulates muscle tone, posture, automatic movements, and the background control of voluntary motion. - Costanzo Physiology
Spinothalamic Tract (listed as a subtype of sensory extrapyramidal pathways)
The spinothalamic tract is the primary sensory pathway for pain, temperature, and crude touch. It crosses to the opposite side at the spinal cord level and ascends to the thalamus (VPL nucleus), then to the somatosensory cortex.
2. Parkinson's Disease
Parkinson's disease (PD) is a neurodegenerative movement disorder caused by the loss of dopaminergic neurons in the substantia nigra pars compacta of the basal ganglia. - Costanzo Physiology
Pathophysiology
- Normal function: dopamine from the substantia nigra activates the direct pathway (promotes movement) and inhibits the indirect pathway (suppresses unwanted movement)
- In PD: dopamine loss tips the balance - the indirect pathway dominates → excessive inhibition of the thalamus → reduced motor output → hypokinesia
- Result: increased tonic and oscillatory GABAergic activity in basal ganglia output nuclei (GPi, SNr), which inhibit the thalamus - Eric Kandel Principles of Neural Science
Classic Tetrad of Symptoms (TRAP)
| Symptom | Description |
|---|---|
| Tremor | Resting tremor ("pill-rolling"), 4-6 Hz, disappears with movement |
| Rigidity | "Cogwheel" or "lead pipe" stiffness |
| Akinesia/Bradykinesia | Slowness and poverty of movement |
| Postural instability | Shuffling gait, festination, falls |
Treatment
- Levodopa (L-DOPA) - crosses the blood-brain barrier and converts to dopamine in the brain. First-line treatment. - Katzung Pharmacology
- Dopamine agonists, MAO-B inhibitors, COMT inhibitors as adjuncts
3. Tremors
A tremor is a rhythmic, involuntary oscillatory movement. Types include:
| Type | When Occurs | Cause |
|---|---|---|
| Resting tremor | At rest, disappears with movement | Parkinson's disease |
| Intention tremor | During purposeful movement, worsens near target | Cerebellar disease |
| Postural/Essential tremor | Holding a posture (outstretched arms) | Essential tremor (most common overall) |
| Physiologic tremor | Normal low-amplitude tremor | Anxiety, caffeine, thyrotoxicosis |
4. Glial Cells
Glial (or neuroglial) cells are the support cells of the nervous system - they outnumber neurons. There are 4 main types in the CNS: - Junqueira's Histology; Eric Kandel Principles of Neural Science
| Cell Type | Location | Key Functions |
|---|---|---|
| Astrocytes | CNS | Structural support, blood-brain barrier maintenance, neurotransmitter recycling (glutamate uptake), ion buffering, scar formation after injury |
| Oligodendrocytes | CNS | Produce myelin in the CNS (each cell myelinates multiple axons). Loss → Multiple Sclerosis |
| Schwann Cells | PNS | Produce myelin in the PNS (each cell myelinates one axon segment). Loss → Guillain-Barré |
| Microglia | CNS | The brain's resident immune cells - surveillance, phagocytosis of debris and pathogens |
| Ependymal cells | CNS | Line ventricles and central canal; produce and circulate CSF |
5. Excitatory & Inhibitory Neurotransmitters
Major Excitatory Neurotransmitters
| NT | Receptor | Role |
|---|---|---|
| Glutamate | NMDA, AMPA, Kainate, mGluR | Main excitatory NT of CNS; involved in learning, memory (LTP), and excitotoxicity in stroke |
| Acetylcholine (ACh) | Nicotinic, Muscarinic | Excitatory at NMJ; involved in memory (hippocampus), autonomic function |
| Norepinephrine | Alpha, Beta adrenergic | Arousal, attention, "fight or flight" |
| Dopamine | D1-D5 | Reward, movement, motivation |
| Serotonin (5-HT) | 5-HT1-7 | Mood, sleep, appetite; can be excitatory or inhibitory depending on receptor subtype - Stahl's Psychopharmacology |
Major Inhibitory Neurotransmitters
| NT | Receptor | Role |
|---|---|---|
| GABA | GABA-A (ionotropic), GABA-B (metabotropic) | Main inhibitory NT of CNS; anticonvulsant, anxiolytic (benzodiazepines enhance GABA-A) |
| Glycine | Glycine receptor (Cl⁻ channel) | Inhibitory in spinal cord and brainstem |
Clinical note: Glutamate (excitatory) drives burst firing of dopaminergic neurons; GABA (inhibitory) causes tonic, low-level basal firing. Balance between the two is key to normal brain function. - Goodman & Gilman's
6. Hemorrhages & Strokes + CT Presentations
Types of Intracranial Hemorrhage
| Type | Location | Cause | CT Appearance |
|---|---|---|---|
| Epidural hematoma | Between skull and dura | Middle meningeal artery tear (temporal bone fracture) | Biconvex (lens-shaped) hyperdense bleed |
| Subdural hematoma | Between dura and arachnoid | Bridging vein tear (elderly, anticoagulated) | Crescent-shaped hyperdense bleed |
| Subarachnoid hemorrhage (SAH) | Subarachnoid space | Ruptured berry aneurysm | Blood in sulci/cisterns ("star pattern"), worse headache of life |
| Intracerebral hemorrhage (ICH) | Brain parenchyma | Hypertension (lenticulostriate arteries), AVM | Hyperdense blob in basal ganglia/thalamus |
Strokes by Territory
| Artery | Territory Supplied | Deficits When Occluded |
|---|---|---|
| ACA (Anterior Cerebral Artery) | Medial frontal & parietal lobes | Contralateral leg > arm weakness/sensory loss; behavioral changes, urinary incontinence |
| MCA (Middle Cerebral Artery) | Lateral frontal, parietal, temporal lobes | Contralateral face + arm > leg weakness/sensory loss; aphasia (dominant side); hemineglect (non-dominant); contralateral homonymous hemianopia |
| PCA (Posterior Cerebral Artery) | Occipital lobe, thalamus | Contralateral homonymous hemianopia (with macular sparing); thalamic sensory loss; alexia without agraphia |
| Lacunar infarcts | Small penetrating arteries (basal ganglia, internal capsule, thalamus, pons) | Pure motor hemiplegia, pure sensory stroke, ataxic hemiparesis, clumsy-hand dysarthria |
Predispositions to stroke → Cardioembolic events: Atrial fibrillation is the #1 cardioembolic cause. Afib causes stasis in the left atrial appendage → thrombus formation → emboli → MCA most commonly occluded.
7. Headaches
| Type | Character | Key Features |
|---|---|---|
| Migraine | Unilateral, throbbing, moderate-severe | Nausea, photophobia, phonophobia; may have aura (visual scotomas) |
| Tension-type | Bilateral, band-like pressure | Most common headache overall; no nausea |
| Cluster | Severe periorbital/unilateral | Horner's syndrome, tearing, rhinorrhea; occurs in clusters |
| Subarachnoid | "Thunderclap" worst of life | Sudden onset, stiff neck, photophobia |
| Raised ICP | Worse in morning, with coughing | Papilledema, vomiting without nausea |
8. Consciousness & Types
Consciousness requires two components:
- Arousal (wakefulness) - maintained by the Reticular Activating System (RAS) in the brainstem/thalamus
- Awareness (content) - maintained by cortical networks
Levels of Impaired Consciousness
| State | Description |
|---|---|
| Confusion | Impaired attention/cognition, oriented |
| Delirium | Acute onset, fluctuating, disorientation, +/- hallucinations |
| Obtundation | Reduced wakefulness, responds to stimulation |
| Stupor | Requires vigorous/painful stimuli to respond |
| Coma | No response to stimuli; GCS ≤ 8 |
| Vegetative state | Sleep-wake cycles preserved, no awareness |
| Brain death | No brainstem reflexes, no spontaneous respiration |
9. Seizures & Epilepsy Types
A seizure is a transient, abnormal, excessive, or hypersynchronous neuronal electrical discharge in the brain.
Epilepsy = 2 unprovoked seizures >24 hours apart, OR 1 seizure with high recurrence risk.
ILAE Classification (2017):
Focal (partial) seizures - arise from one hemisphere:
- Focal aware (consciousness intact) - formerly "simple partial"
- Focal impaired awareness (consciousness altered) - formerly "complex partial"
- Focal to bilateral tonic-clonic
Generalized seizures - involve both hemispheres from onset:
| Type | Description |
|---|---|
| Tonic-clonic | Stiffening (tonic) then jerking (clonic); post-ictal confusion |
| Absence | Brief staring (3Hz spike-wave on EEG); no post-ictal phase; common in children |
| Myoclonic | Brief shock-like muscle jerks |
| Atonic | Sudden loss of muscle tone ("drop attacks") |
| Tonic | Sustained muscle stiffening |
| Clonic | Repetitive rhythmic jerking |
- Bradley & Daroff's Neurology; Lippincott Pharmacology
10. Vertigo
Vertigo = illusion of movement (spinning sensation) of self or environment. It is NOT just dizziness - it implies vestibular system dysfunction.
Peripheral vs. Central Vertigo
| Feature | Peripheral (inner ear/CN VIII) | Central (brainstem/cerebellum) |
|---|---|---|
| Cause | BPPV, Menière's, vestibular neuritis | Stroke (PICA/AICA), MS, tumor |
| Nystagmus | Horizontal, fatigues | Vertical or direction-changing, does NOT fatigue |
| Severity | Severe but benign | Less severe but dangerous |
| Hearing loss | May be present (Menière's) | Absent |
| Romberg | Falls toward lesion | Variable |
BPPV (Benign Paroxysmal Positional Vertigo) - most common cause; treated with Epley maneuver (repositioning otoliths).
11. Paralysis & Paresis
- Paresis = partial weakness (incomplete loss of motor function)
- Paralysis (plegia) = complete loss of motor function
Patterns:
| Term | Meaning |
|---|---|
| Monoplegia | One limb |
| Hemiplegia | Same-side arm + leg |
| Paraplegia | Both legs (spinal cord) |
| Tetraplegia/Quadriplegia | All four limbs |
| Diplegia | Bilateral, legs > arms (cerebral palsy) |
12. Stereognosis & Graphesthesia
These are cortical sensory functions - tested to assess parietal lobe (specifically the somatosensory association cortex):
- Stereognosis = ability to recognize an object by touch alone (e.g., identifying a key placed in the hand with eyes closed). Loss = astereognosis → parietal lobe lesion
- Graphesthesia = ability to recognize numbers/letters traced on the skin. Loss = agraphesthesia → parietal lobe lesion
13. UMN vs. LMN Lesions - Signs & Tests
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Location | Brain/spinal cord (above anterior horn) | Anterior horn cell, nerve root, peripheral nerve, NMJ, muscle |
| Tone | Increased (spasticity) | Decreased (flaccidity) |
| Reflexes | Hyperreflexia | Hyporeflexia/areflexia |
| Babinski sign | Positive (extensor plantar response) | Absent (normal flexor response) |
| Fasciculations | Absent | Present |
| Atrophy | Late, mild (disuse) | Early, severe (denervation) |
| Clonus | Present | Absent |
| Weakness pattern | Contralateral face+arm+leg (cortex) or ipsilateral (spinal cord) | Focal/segmental |
- Frameworks for Internal Medicine; Neuroanatomy through Clinical Cases
14. Cranial Nerves (CN) - Functions
| CN | Name | Function |
|---|---|---|
| I | Olfactory | Smell |
| II | Optic | Vision |
| III | Oculomotor | Eye movement (superior, inferior, medial recti, inferior oblique), pupil constriction (pupillary light reflex), lid elevation |
| IV | Trochlear | Superior oblique (eye moves down+in) |
| V | Trigeminal | Facial sensation (3 divisions); mastication muscles |
| VI | Abducens | Lateral rectus (abducts eye) |
| VII | Facial | Facial expression, taste (anterior 2/3 tongue), lacrimal/salivary glands |
| VIII | Vestibulocochlear | Hearing + balance |
| IX | Glossopharyngeal | Taste (posterior 1/3 tongue), gag reflex (afferent), parotid gland |
| X | Vagus | Gag reflex (efferent), heart rate, GI, larynx/pharynx |
| XI | Spinal Accessory | Sternocleidomastoid + trapezius |
| XII | Hypoglossal | Tongue movement |
Bell's Palsy vs. Facial Nerve Palsy
Bell's palsy = idiopathic LMN facial nerve (CN VII) palsy.
- Affects entire ipsilateral face (forehead + lower face) - patient cannot close eye or raise eyebrow
- Compare with UMN lesion (e.g., stroke): spares the forehead (forehead receives bilateral cortical innervation)
Facial palsy is a sign. Bell's palsy is the diagnosis when no other cause found (presumed viral - HSV-1 reactivation). Treatment: prednisolone + acyclovir.
15. EEG Graphs & Waves
An EEG (Electroencephalogram) records the brain's electrical activity. Key waveforms:
| Wave | Frequency | State |
|---|---|---|
| Delta (δ) | < 4 Hz | Deep sleep (NREM 3), coma, infants |
| Theta (θ) | 4-8 Hz | Drowsiness, early sleep, meditation |
| Alpha (α) | 8-12 Hz | Relaxed wakefulness, eyes closed, occipital |
| Beta (β) | 13-30 Hz | Alert, active thinking, frontal |
| Gamma (γ) | > 30 Hz | Higher cognitive processing |
EEG in epilepsy:
- Absence seizure = 3 Hz spike-and-wave discharges (generalized)
- Focal seizures = localized spike activity
- Hypsarrhythmia = chaotic pattern in infantile spasms (West syndrome)
16. Aphasias
Aphasia = acquired language disturbance (not just speech). Typically from lesions in the dominant (usually left) hemisphere.
| Type | Fluency | Comprehension | Repetition | Lesion Location |
|---|---|---|---|---|
| Broca's (Expressive) | Non-fluent | Intact | Impaired | Left frontal lobe (Broca's area, BA 44/45) |
| Wernicke's (Receptive) | Fluent (but meaningless) | Impaired | Impaired | Left temporal lobe (Wernicke's area, BA 22) |
| Conduction | Fluent | Intact | Severely impaired | Arcuate fasciculus (connects Broca's + Wernicke's) |
| Global | Non-fluent | Impaired | Impaired | Large left MCA territory |
| Transcortical Motor | Non-fluent | Intact | Intact | Frontal lobe (anterior to Broca's) |
| Anomic | Fluent | Intact | Intact | Various; angular gyrus |
- Eric Kandel Principles of Neural Science
17. Functions of the Lobes
| Lobe | Key Functions | Lesion Signs |
|---|---|---|
| Frontal | Voluntary motor (precentral gyrus), executive function, personality, Broca's speech area, working memory, inhibition | Contralateral hemiplegia, personality change, disinhibition, expressive aphasia, perseveration |
| Parietal | Somatosensory (postcentral gyrus), spatial integration, stereognosis, graphesthesia, body image | Contralateral sensory loss, astereognosis, agraphesthesia, neglect (non-dominant), Gerstmann syndrome (dominant) |
| Temporal | Auditory cortex, memory (hippocampus), Wernicke's speech area, emotion (amygdala) | Receptive aphasia, memory loss, auditory hallucinations, déjà vu |
| Occipital | Visual cortex (primary + association) | Contralateral hemianopia, visual agnosia, cortical blindness |
| Limbic system | Emotion, memory consolidation, olfaction | Amnesia (bilateral hippocampal damage), personality/emotional changes |
18. Horner's Syndrome (Triad)
Horner's syndrome results from disruption of the oculosympathetic pathway (3 neurons from hypothalamus → spinal cord → superior cervical ganglion → orbit).
Classic Triad:
- Ptosis (drooping eyelid) - from paralysis of superior tarsal muscle (Müller's muscle)
- Miosis (constricted pupil) - loss of sympathetic mydriasis
- Anhidrosis (loss of sweating) - on the ipsilateral face (if lesion is pre-ganglionic)
Sometimes a 4th sign is added: enophthalmos (sunken eyeball - more apparent than real)
Causes by Level:
- Central (1st order): Stroke (lateral medullary/Wallenberg syndrome), syringomyelia, MS
- Pre-ganglionic (2nd order): Pancoast tumor (lung apex), cervical rib, neck dissection
- Post-ganglionic (3rd order): Carotid artery dissection, cavernous sinus thrombosis
19. Anisocoria
Anisocoria = unequal pupil sizes. The key clinical question is: which pupil is abnormal?
| Scenario | Abnormal Pupil | Cause |
|---|---|---|
| Anisocoria worse in light | Larger pupil (fails to constrict) | CN III palsy (posterior communicating artery aneurysm, herniation), pharmacologic mydriasis |
| Anisocoria worse in dark | Smaller pupil (fails to dilate) | Horner's syndrome |
| Bilateral fixed dilated | Both | Brainstem herniation, atropine poisoning, death |
| Bilateral fixed constricted | Both | Opioid toxicity, pontine hemorrhage |
20. Glasgow Coma Scale (GCS)
The GCS quantifies level of consciousness. Minimum score = 3 (deep coma), Maximum = 15 (normal).
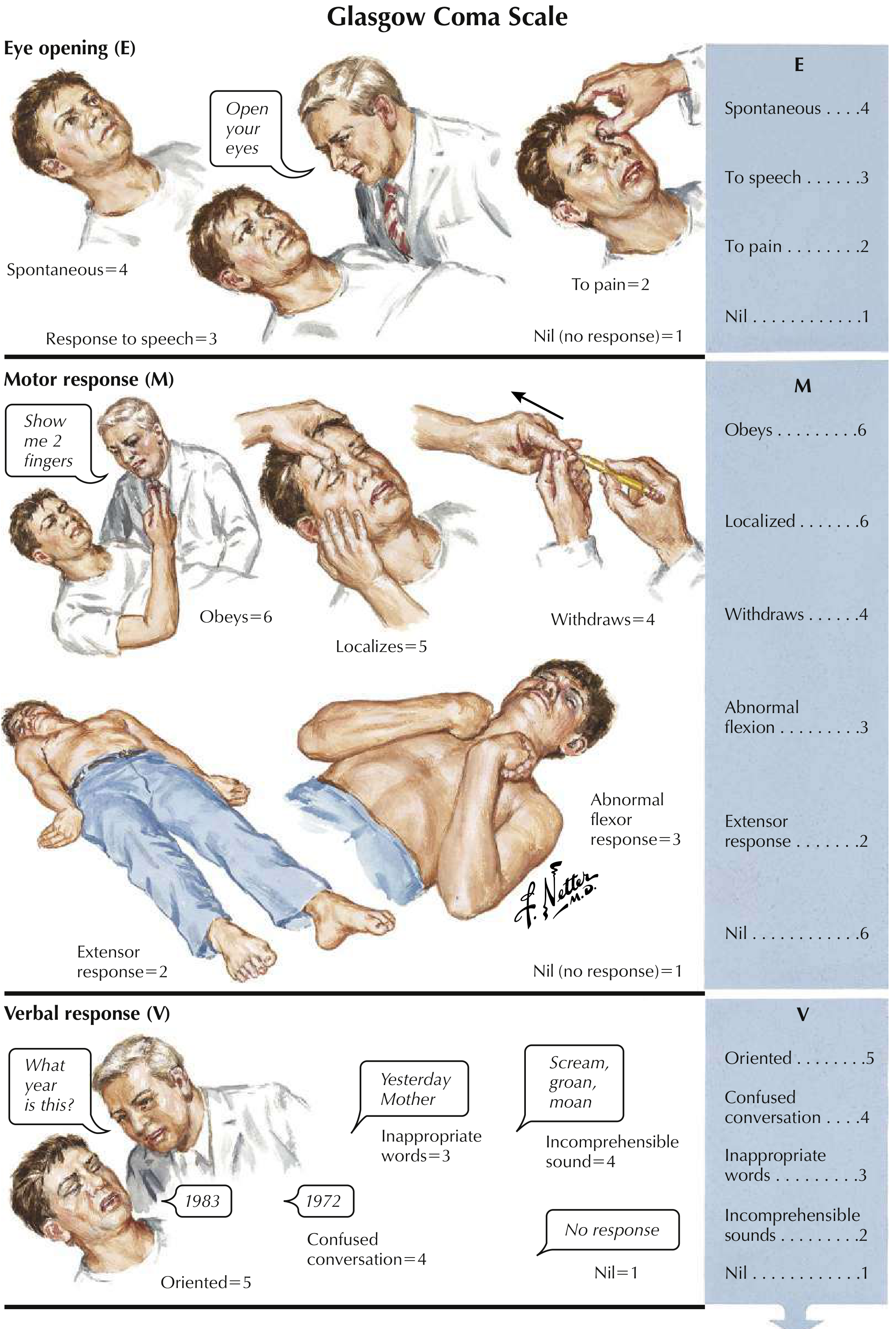
GCS = E + M + V
| Domain | Response | Score |
|---|---|---|
| Eye (E) | Spontaneous | 4 |
| To speech | 3 | |
| To pain | 2 | |
| None | 1 | |
| Motor (M) | Obeys commands | 6 |
| Localizes pain | 5 | |
| Withdraws | 4 | |
| Abnormal flexion (decorticate) | 3 | |
| Extension (decerebrate) | 2 | |
| None | 1 | |
| Verbal (V) | Oriented | 5 |
| Confused | 4 | |
| Inappropriate words | 3 | |
| Incomprehensible sounds | 2 | |
| None | 1 |
Clinical cutoffs:
-
GCS ≤ 8 = coma → consider intubation
-
GCS 9-12 = moderate head injury
-
GCS 13-15 = mild head injury
-
Tintinalli's Emergency Medicine; Gray's Anatomy for Students; Rosen's Emergency Medicine
Summary Map
NEUROSCIENCE SYLLABUS
│
├── Motor Pathways: Pyramidal (voluntary) vs. Extrapyramidal (tone/posture)
│ └── Spinothalamic = sensory (pain/temp)
│
├── Movement Disorders
│ ├── Parkinson's → dopamine loss → basal ganglia dysfunction
│ └── Tremors → resting (PD), intention (cerebellum), postural (essential)
│
├── Support Cells: Glial cells (Astrocytes, Oligodendrocytes, Microglia, Ependymal)
│
├── Neurotransmitters: Glutamate/ACh (excitatory) ↔ GABA/Glycine (inhibitory)
│
├── Vascular Neurology
│ ├── Hemorrhages: Epidural / Subdural / SAH / ICH
│ └── Strokes: ACA (leg), MCA (face+arm), PCA (vision), Lacunar
│ └── Predisposition: Atrial fibrillation → cardioembolic
│
├── Headaches: Migraine, Tension, Cluster, SAH, ICP
│
├── Consciousness: Arousal (RAS) + Awareness (cortex)
│
├── Seizures & Epilepsy: Focal vs. Generalized (absence, tonic-clonic, etc.)
│
├── Vertigo: Peripheral (BPPV, Menière's) vs. Central (stroke)
│
├── Motor Deficits: Paralysis/Paresis → UMN vs. LMN signs
│
├── Cortical Sensation: Stereognosis, Graphesthesia (parietal lobe)
│
├── Cranial Nerves (I-XII) + Bell's palsy (CN VII LMN)
│
├── EEG Waves: Delta/Theta/Alpha/Beta/Gamma
│
├── Aphasias: Broca's (frontal), Wernicke's (temporal), Conduction (arcuate fasciculus)
│
├── Lobe Functions: Frontal/Parietal/Temporal/Occipital
│
├── Horner's Syndrome: Ptosis + Miosis + Anhidrosis (sympathetic chain disruption)
│
├── Anisocoria: Which pupil is abnormal? (light vs. dark test)
│
└── Glasgow Coma Scale: E(4) + M(6) + V(5) = 15 max; ≤8 = coma
This covers every item on your neuroscience syllabus. Let me know if you want any specific topic expanded further with diagrams, clinical cases, or drug treatments!
Tell me about receptors
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Here is a detailed, comprehensive breakdown of all Sensory Receptors in neuroscience:
🧠 Sensory Receptors - Complete Guide
Sensory receptors are specialized structures that convert (transduce) physical or chemical stimuli from the environment into electrical nerve signals (action potentials) that the brain can interpret. They are classified by the type of stimulus they detect.
Overview: Classification by Stimulus Type
| Category | Stimulus Detected | Examples |
|---|---|---|
| Mechanoreceptors | Mechanical force (touch, pressure, vibration, stretch) | Pacinian, Meissner, Ruffini, Merkel, hair follicles |
| Thermoreceptors | Temperature changes | Warm receptors (TRPV), Cold receptors (TRPM8) |
| Nociceptors | Tissue-damaging/painful stimuli | A-delta fibers, C fibers |
| Proprioceptors | Body position and muscle length/tension | Muscle spindles, Golgi tendon organs, joint receptors |
| Chemoreceptors | Chemical stimuli | Taste buds (gustatory), olfactory receptors, carotid body |
| Photoreceptors | Light | Rods and cones (retina) |
| Osmoreceptors | Osmotic pressure | Hypothalamic neurons |
| Baroreceptors | Blood pressure/vessel stretch | Carotid sinus, aortic arch |
Key Concept: Adaptation
Before the individual receptors, you must understand adaptation - how receptors respond to a sustained constant stimulus:
- Phasic receptors (rapidly adapting): Fire at onset and offset of stimulus, then go silent. They detect change and movement.
- Tonic receptors (slowly adapting): Keep firing as long as stimulus persists. They encode intensity and duration.
"Phasic receptors detect onset and offset of stimulus. Tonic receptors encode stimulus intensity: the greater the intensity, the larger the depolarizing receptor potential, and the more likely action potentials are to occur." - Costanzo Physiology
1. Mechanoreceptors
Mechanoreceptors detect touch, pressure, vibration, and stretch. They are found in both hairy and non-hairy (glabrous) skin.
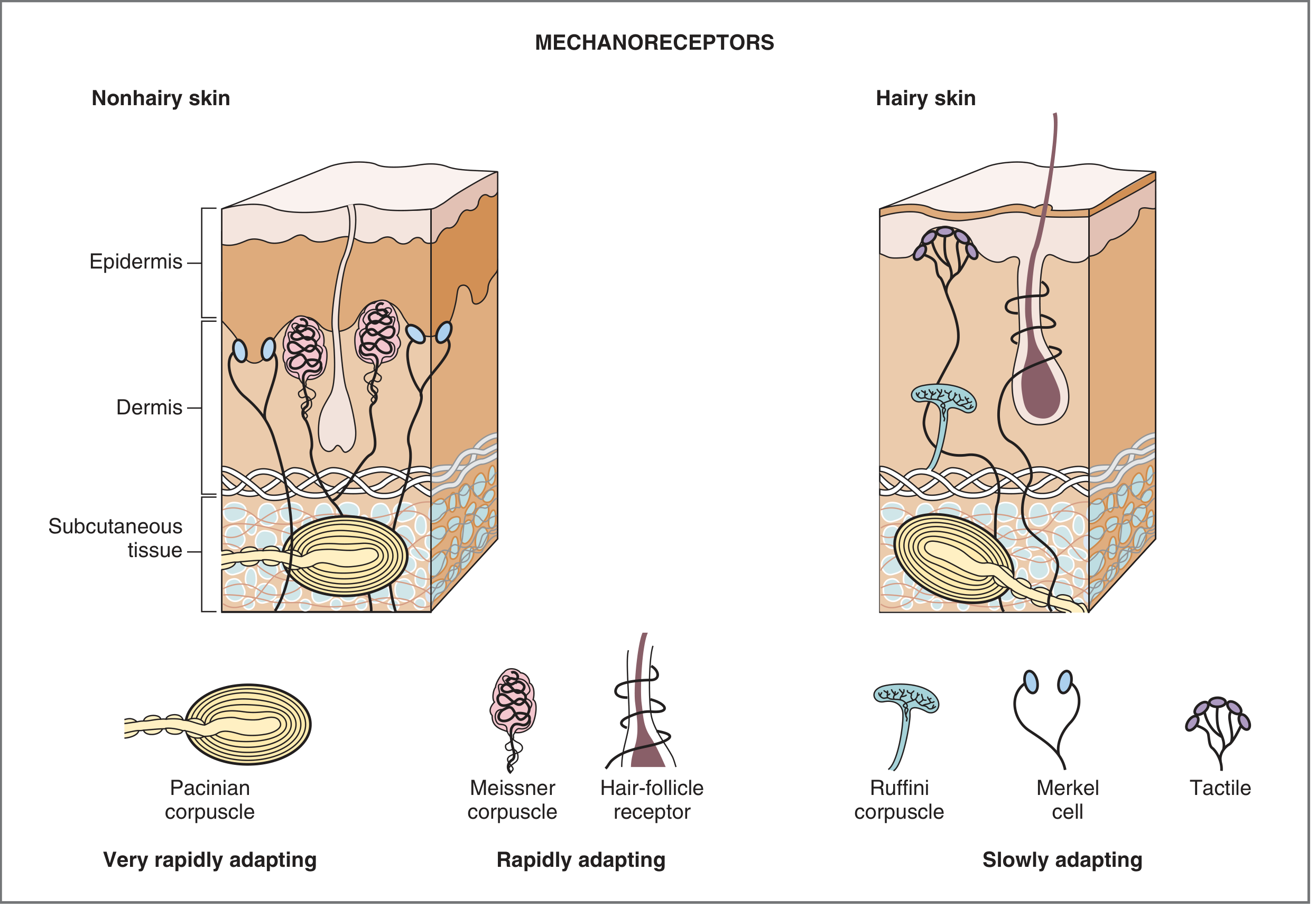
The 6 Cutaneous Mechanoreceptors
| Receptor | Location | Adaptation | Receptive Field | Sensation Encoded |
|---|---|---|---|---|
| Pacinian corpuscle | Deep dermis/subcutaneous, in muscle | Very rapidly | Large | Vibration, tapping, deep pressure |
| Meissner corpuscle | Dermis of non-hairy skin (fingertips, lips) | Rapidly | Small | Light touch, two-point discrimination, flutter |
| Hair follicle receptor | Around hair follicles in hairy skin | Rapidly | Medium | Velocity and direction of movement |
| Ruffini corpuscle | Dermis of hairy + non-hairy skin, joint capsules | Slowly | Large | Skin stretch, joint rotation |
| Merkel receptor (Merkel cell) | Epidermis of non-hairy skin | Slowly | Small | Steady pressure, vertical indentation, fine texture |
| Tactile disc | Hairy skin | Slowly | Small | Vertical indentation of skin |
- Costanzo Physiology; Neuroscience: Exploring the Brain
Details on Each
1. Pacinian Corpuscle
- Largest mechanoreceptor (up to 2 mm long!)
- Onion-like layered capsule surrounding a nerve ending
- Located deep in dermis, subcutaneous tissue, and even inside muscles
- ~2,500 in each human hand
- Detects vibration (best at 200-300 Hz) and rapid changes in pressure
- Because they adapt so rapidly, they fire only at onset AND offset of a stimulus (on-off detectors)
2. Meissner's Corpuscle
- Encapsulated, located in dermis of non-hairy (glabrous) skin - fingertips, lips, palms
- Only about 1/10th the size of Pacinian corpuscles
- Small receptive fields → excellent two-point discrimination
- Best for detecting texture, tapping, flutter (~5-40 Hz)
- Most dense in fingertips - why fingertips are so sensitive to fine textures
3. Hair Follicle Receptors
- Networks of nerve fibers wrapping around hair follicles
- Activated when hair is bent or displaced
- Rapidly adapting → detect velocity and direction of stimulus moving across skin
- Even a light breeze over arm hair activates these
4. Ruffini's Corpuscle
- Elongated, spindle-shaped encapsulated receptor
- Found in both hairy and non-hairy skin, and in joint capsules
- Large receptive fields - a stimulus from a distance can still activate them
- Slowly adapting → detects sustained skin stretch, joint rotation and angle
- Important for hand grip and knowing joint position
5. Merkel's Disk (Merkel Cell)
- A nerve terminal ending + a specialized epithelial cell (the Merkel cell)
- In the epidermis of non-hairy skin
- Small receptive field → good spatial resolution
- Slowly adapting → fires continuously with sustained pressure
- Best for fine spatial detail and texture discrimination (e.g., reading braille)
6. Tactile Disc
- Similar to Merkel receptors but found in hairy skin
Two-Point Discrimination
Because receptive field size varies, body parts with many small-field receptors (Meissner + Merkel) have the best two-point discrimination (ability to tell two nearby touches apart):
- Fingertip: ~2 mm
- Lip: ~3 mm
- Back: ~40-70 mm (fewest fine receptors)
2. Thermoreceptors
Thermoreceptors are slowly adapting receptors that detect temperature changes in the skin. There are two functional classes:
| Type | Active Range | Molecular Channel | Activated By |
|---|---|---|---|
| Warm receptors | 30-45°C (quiescent below 36°C) | TRPV1 (vanilloid family) | Heat, capsaicin (chili peppers feel "hot"!) |
| Cold receptors | 10-35°C (quiescent above 36°C) | TRPM8 | Cold, menthol (menthol "feels cold"!) |
Key points:
- At ~36°C both types overlap in activity
- Above 45°C: warm receptors shut off → nociceptors (TRPV1) take over - this is when heat becomes painful
- Below freezing: cold receptors shut off → nociceptors take over - freezing cold = painful
- TRP channels = Transient Receptor Potential channels - ion channels that open in response to physical/chemical stimuli
"Transduction of cold temperatures involves TRPM8, which is also opened by menthol (which gives a cold sensation)." - Costanzo Physiology
3. Nociceptors (Pain Receptors)
Nociceptors respond to tissue-damaging or potentially damaging stimuli (mechanical, thermal, chemical). They are free nerve endings - bare, unencapsulated.
Two Major Types
| Type | Fiber | Myelination | Speed | Pain Quality |
|---|---|---|---|---|
| Thermal/Mechanical nociceptor | A-delta (Aδ) | Thin myelinated | Fast (5-30 m/s) | Sharp, pricking, first pain - well-localized |
| Polymodal nociceptor | C fiber | Unmyelinated | Slow (0.5-2 m/s) | Burning, aching, second pain - poorly localized |
- Aδ fibers carry the "first pain" - the immediate, sharp sensation you feel right when you stub your toe
- C fibers carry the "second pain" - the throbbing, burning pain that lingers afterward
Inflammatory Sensitization (Hyperalgesia)
When tissue is damaged, many chemicals are released that sensitize nociceptors:
- Bradykinin - directly activates nociceptors
- Prostaglandins - lower pain threshold (why NSAIDs/aspirin/ibuprofen work - they block prostaglandin synthesis)
- Substance P - released by nociceptors themselves; causes vasodilation and mast cell degranulation
- Histamine (from mast cells) - directly activates nociceptors
- K⁺ and H⁺ (from damaged cells) - depolarize nociceptor membranes
Result: Hyperalgesia = a normally painful stimulus hurts MORE than usual; or a normally non-painful stimulus becomes painful (allodynia).
"Damaged skin releases a variety of chemicals including bradykinin, prostaglandins, substance P, K+, and H+ which initiate the inflammatory response... Mast cells release histamine, which directly activates nociceptors." - Costanzo Physiology
4. Proprioceptors (Position Sense)
Proprioceptors tell the brain about muscle length, tension, and joint position - essential for coordinated movement without looking at your limbs.
Muscle Spindle
- Located inside skeletal muscle (intrafusal fibers), parallel to regular muscle fibers (extrafusal fibers)
- Detects change in muscle length (stretch)
- Afferent fibers:
- Ia (primary): wraps around nuclear bag fibers → detects rate of change (velocity) of stretch → phasic response
- II (secondary): wraps around nuclear chain fibers → detects sustained stretch → tonic response
- Controls the stretch reflex (myotatic reflex): muscle stretches → spindle fires → Ia fibers → alpha motor neuron → muscle contracts back
- Gamma motor neurons set the sensitivity of the spindle by contracting the intrafusal fibers
Golgi Tendon Organ (GTO)
- Located at the muscle-tendon junction, in series with muscle fibers
- Detects muscle tension (force, not length)
- Afferent fiber: Ib
- When tension is too high → Ib fibers → inhibitory interneuron → motor neuron inhibited → muscle relaxes
- This is the inverse stretch reflex (protective mechanism to prevent tendon/muscle tear)
- Ganong's Physiology
| Feature | Muscle Spindle | Golgi Tendon Organ |
|---|---|---|
| Location | Inside muscle | Muscle-tendon junction |
| Arrangement | Parallel to extrafusal fibers | In series with fibers |
| Detects | Length (stretch) | Tension (force) |
| Fiber | Ia and II | Ib |
| Reflex | Stretch reflex (contraction) | Inverse stretch reflex (relaxation) |
| Purpose | Maintains muscle length | Protects against excess tension |
Joint Receptors
- Free nerve endings and Ruffini-like endings in joint capsules and ligaments
- Detect joint angle, velocity of joint movement, pressure
5. Chemoreceptors
Peripheral Chemoreceptors
- Carotid body (at carotid bifurcation) and aortic bodies: detect ↓PO₂, ↑PCO₂, ↓pH in blood → stimulate breathing
- Afferent via CN IX (glossopharyngeal) for carotid body, CN X (vagus) for aortic bodies
Central Chemoreceptors
- In the medulla oblongata: detect ↑PCO₂ and ↓pH in CSF → most powerful drive for ventilation
Taste (Gustatory) Receptors
- On taste buds (tongue, palate, epiglottis)
- 5 basic tastes: sweet, salty, sour, bitter, umami
- Receptor cells are modified epithelial cells, not neurons
Olfactory Receptors
- Located in the olfactory epithelium of the nasal roof
- Only sensory neurons that directly regenerate and have direct access to the brain (CN I → olfactory bulb → piriform cortex)
- ~400 types of receptors → can distinguish thousands of odors by combination
6. Photoreceptors (Retinal Receptors)
Located in the retina of the eye:
| Receptor | Number | Location | Function | Pigment |
|---|---|---|---|---|
| Rods | ~120 million | Peripheral retina | Night/dim light vision, black & white | Rhodopsin |
| Cones | ~6 million | Central retina (fovea) | Daytime/color vision, fine detail | Photopsins (red, green, blue) |
Signal cascade: Light → photopigment bleaching → ↓cGMP → closing of Na⁺ channels → hyperpolarization (unusual - receptors hyperpolarize rather than depolarize!) → less glutamate released onto bipolar cells
7. Baroreceptors & Osmoreceptors
Baroreceptors (Stretch Receptors in Blood Vessels)
- Carotid sinus baroreceptors: in the wall of internal carotid artery → detect blood pressure via vessel wall stretch
- Aortic arch baroreceptors: similar function
- When BP rises → baroreceptors fire more → via CN IX/X → brainstem (nucleus tractus solitarius) → reflex bradycardia + vasodilation to lower BP
- Bainbridge reflex: atrial stretch → ↑ heart rate
Osmoreceptors
- In the anterior hypothalamus (organum vasculosum of lamina terminalis, OVLT)
- Detect ↑ plasma osmolarity → stimulate ADH (vasopressin) release + thirst
Sensory Pathways: How Receptor Signals Reach the Brain
All sensory signals travel via a 3-neuron chain:
1st Order Neuron → 2nd Order Neuron → 3rd Order Neuron → Cortex
(DRG/cranial ganglion) (spinal cord/brainstem) (Thalamus, VPL)
Two Major Pathways:
| Pathway | Carries | Crosses Midline | Tract |
|---|---|---|---|
| Dorsal Column - Medial Lemniscal | Fine touch, vibration, 2-point discrimination, proprioception | At the medulla (decussates) | Fasciculus gracilis (legs) + fasciculus cuneatus (arms) |
| Anterolateral (Spinothalamic) | Pain, temperature, crude touch | At the spinal cord level (within 1-2 segments) | Lateral spinothalamic tract |
Clinical pearl: A right-sided spinal cord lesion → right side loses fine touch/proprioception but left side loses pain/temperature (crossed at different levels). This pattern is called Brown-Séquard syndrome.
Quick Summary Table
| Receptor | Type | Adapts | Detects | Fiber |
|---|---|---|---|---|
| Pacinian corpuscle | Encapsulated | Very rapidly | Vibration | Aβ |
| Meissner's corpuscle | Encapsulated | Rapidly | Light touch, 2-point | Aβ |
| Hair follicle | Unencapsulated | Rapidly | Movement direction | Aβ |
| Ruffini's corpuscle | Encapsulated | Slowly | Stretch, joint angle | Aβ |
| Merkel's disk | Unencapsulated | Slowly | Sustained pressure, texture | Aβ |
| Warm receptor | Free ending | Slowly | 30-45°C heat | Aδ/C |
| Cold receptor | Free ending | Slowly | 10-35°C cold | Aδ/C |
| A-delta nociceptor | Free ending | - | Sharp/pricking pain | Aδ |
| C fiber nociceptor | Free ending | - | Burning/aching pain | C |
| Muscle spindle | Encapsulated | Both | Muscle length (stretch) | Ia, II |
| Golgi tendon organ | Encapsulated | Tonic | Muscle tension | Ib |
| Photoreceptors (rod/cone) | Specialized | - | Light | CN II |
| Carotid body | Specialized | - | O₂/CO₂/pH | CN IX |
This covers all sensory receptor types in the neuroscience context. Let me know if you want to go deeper on any specific receptor or its clinical relevance!
This is a shared conversation. Sign in to Orris to start your own chat.