Multiple apex beat how to find clinically apex beat?
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough, textbook-based answer covering how to find the apex beat clinically and what a multiple (double/triple) apex beat means.
Apex Beat: Clinical Examination & Multiple Apex Beat
1. What is the Apex Beat?
The apex beat (apical impulse) is the outermost and lowest point of visible or palpable cardiac pulsation on the chest wall. It represents the brief outward thrust of the left ventricular (LV) apex against the chest wall during isovolumic contraction.
- Normal location: 5th intercostal space (ICS), midclavicular line (MCL)
- Normal size: area < 3 cm in diameter (roughly 1 fingerbreadth)
- Normal character: brief, outward tap occupying only the first two-thirds of ventricular systole
2. How to Find the Apex Beat - Clinical Technique
Step 1: Inspect First
- Look at the chest wall with tangential lighting (patient at 30° supine)
- A visible pulsation at the expected location is normal in thin adults
- Any pulsation outside the 5th ICS/MCL is abnormal
Step 2: Palpate
Starting position: Patient supine at 30°. Examine directly on bare skin - never through clothes.
- Broad hand sweep: Place the entire right hand flat over the precordium, starting at the inframammary area, to locate the impulse.
- In women: Use the left hand to gently displace the breast laterally, then palpate the inframammary fold with the right hand.
- Once located: Use the finger pads (not fingertips) of 2-3 fingers to precisely characterize the impulse.
- If not palpable supine: Turn the patient to the left lateral decubitus (LLD) position with the left arm tucked under the pillow - this brings the heart closer to the chest wall. Ask for held expiration (heart moves anteriorly).
Note: LLD position shifts the apex laterally by 2-3 cm, so it should not be used to judge location, only to improve palpation of contour and character.
What to Assess Once Found:
| Feature | Normal | Abnormal |
|---|---|---|
| Location | 5th ICS, MCL | Displaced laterally/inferiorly (LV dilatation); laterally (RV enlargement) |
| Size | < 3 cm | > 3 cm = diffuse (LV dilatation) |
| Character/Duration | Brief, tapping, ends well before S2 | Sustained (pressure overload, AS, HCM); heaving/forceful |
| Number of impulses | Single | Double or triple (see below) |
3. Multiple Apex Beat (Double / Triple Ripple)
A "multiple" apex beat means more than one distinct outward impulse is felt per cardiac cycle at the apex. This is an important clinical sign.
Double Apex Beat (Two impulses per cycle)
Two components can be felt:
- Presystolic component (palpable S4): Due to forceful atrial contraction into a non-compliant, stiff LV. Felt just before the main LV systolic impulse. Corresponds to an audible (or sometimes silent) 4th heart sound. Seen in: LV hypertrophy, hypertrophic cardiomyopathy (HCM), aortic stenosis, hypertension.
- Double systolic beat (bisferiens character at apex): Two peaks within systole itself, as in severe HCM with LVOT obstruction or aortic regurgitation.
In HCM without obstruction, Goldman-Cecil Medicine describes: "poorly compliant... left (S4 gallop, double-apex beat) ventricles" - the double beat reflects a palpable atrial impulse followed by LV contraction.
In HCM with LVOT obstruction, the apex beat is "sustained or double (reflecting a palpable atrial impulse followed by left ventricular contraction)" - Goldman-Cecil Medicine.
Triple Apex Beat ("Triple Ripple") - Classic of HOCM
The hallmark of hypertrophic obstructive cardiomyopathy (HOCM):
Three distinct impulses are felt per cycle:
- Presystolic (S4) - due to atrial kick into stiff LV
- Early systolic peak - initial LV ejection before LVOT obstruction kicks in
- Late systolic peak - second systolic impulse after the obstruction causes a brief withdrawal then re-thrust
Fuster & Hurst's The Heart describes this as: "the so-called triple ripple... palpable systolic impulse in early and midsystole, separated by withdrawal of the apical impulse related to dynamic outflow obstruction; a palpable atrial contraction corresponds to the third impulse."
Harrison's adds: "HOCM may very rarely cause a triple cadence beat at the apex with contributions from a palpable S4 and the two components of the bisferiens systolic pulse."
The Washington Manual confirms: "forceful double or triple apical impulse" associated with HOCM.
4. Apical Impulse Contour Diagram
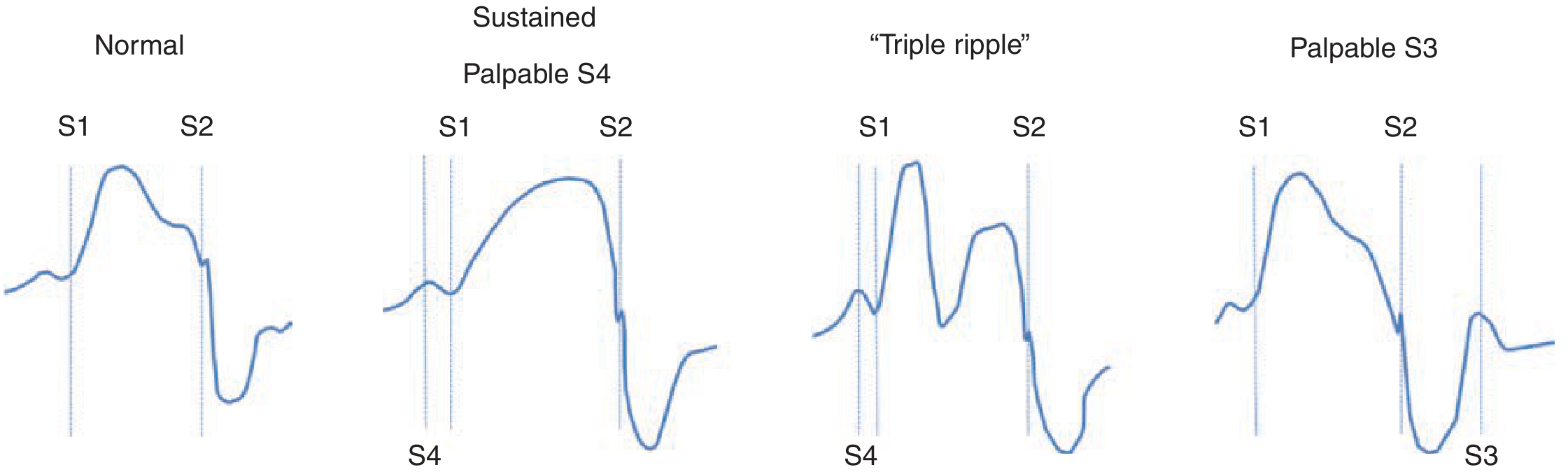
Figure: Apical impulse contour in normal, sustained with palpable S4, "triple ripple" (HOCM), and palpable S3. - Fuster & Hurst's The Heart, 15th Ed.
5. Causes of Multiple Apex Beat - Summary
| Type | Description | Classic Cause |
|---|---|---|
| Double apex beat | Presystolic (S4) + systolic impulse | HCM (non-obstructive), LV hypertrophy, aortic stenosis |
| Double apex beat | Two peaks within systole | HCM with LVOT obstruction, severe AR |
| Triple ripple | S4 + two systolic peaks | HOCM (classic and most specific sign) |
| Palpable S3 + systole | Systolic + early diastolic rebound | Dilated cardiomyopathy, severe MR/AR with heart failure |
6. Shifts of Apex Beat (Causes of Displacement)
- Pushed to opposite side: Pleural effusion, tension pneumothorax, hemothorax (space-occupying lesion)
- Pulled to same side: Massive collapse (lobar or total lung collapse), fibrosis
- Displaced left + downward: LV cavity dilatation (volume overload: AR, MR, DCM)
- Laterally only: RV enlargement pushing LV apex
Sources:
- Fuster & Hurst's The Heart, 15th Ed. (Palpation section)
- Harrison's Principles of Internal Medicine, 22E - Cardiovascular Examination
- Goldman-Cecil Medicine, International Ed. - HCM Diagnosis
- The Washington Manual of Medical Therapeutics - Physical Examination in HCM
- S Das: A Manual on Clinical Surgery, 13th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.