I have pain on left side thigh mid and lateral only when I touch that with mild pressure from years and I tell this by elicited with same pressure on opposite side thigh
Reading File
Finding Sources
Finding Sources
Searching the Web
lateral thigh pain only on touch pressure allodynia meralgia paresthetica diagnosis
Reading File
Reading File
Reading File
Loading Image
Here is a thorough breakdown of your symptom pattern:
Most Likely Diagnosis: Meralgia Paresthetica (Bernhardt-Roth Syndrome)
Your description fits this condition almost perfectly:
- Pain only when touched (not spontaneous) on the left lateral/mid thigh
- Unilateral (left side only)
- Years of duration (can be chronic)
- Confirmed by comparison to the other side - the right thigh feels normal with the same pressure
This type of pain-on-touch is called allodynia - pain triggered by a stimulus (light pressure) that would not normally cause pain. It is the hallmark of a sensory nerve problem, not a muscle or bone problem.
What Is Meralgia Paresthetica?
It is caused by entrapment (compression) of the Lateral Femoral Cutaneous Nerve (LFCN), a purely sensory nerve with no motor function. It supplies feeling to the anterolateral (front and outer) portion of the thigh.
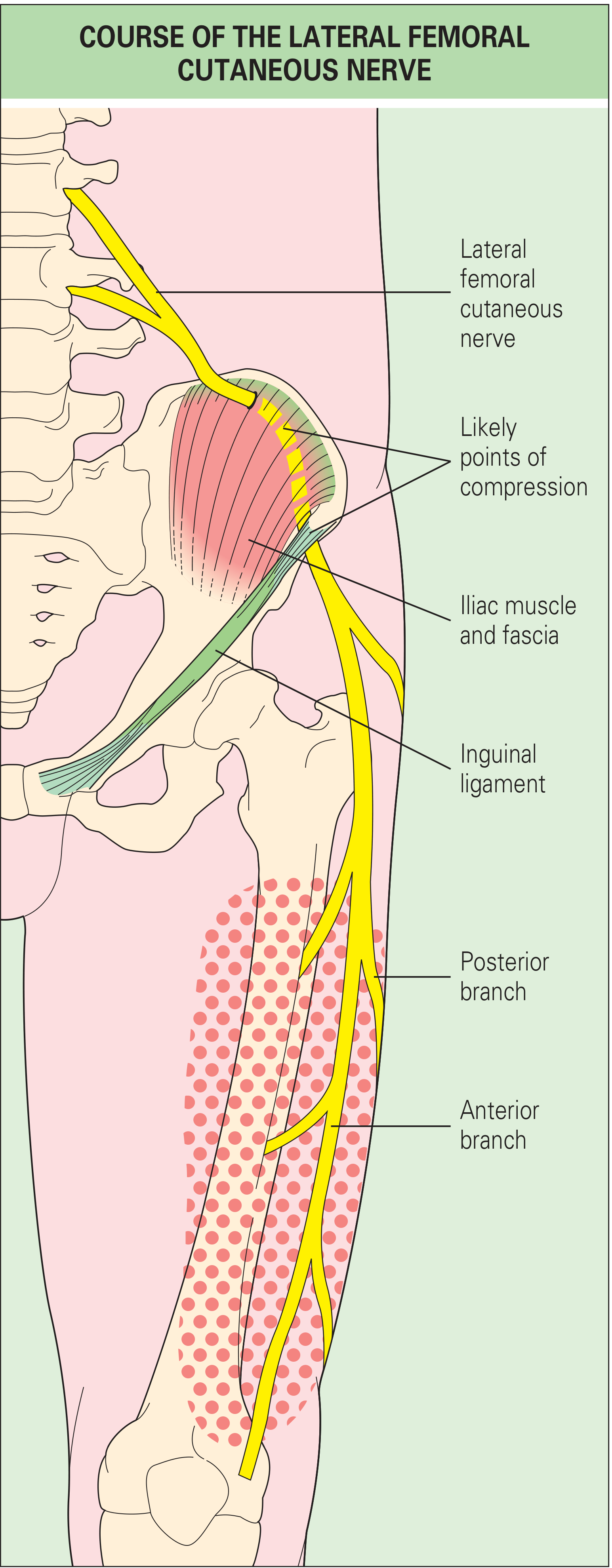
The nerve originates from spinal roots L2-L3, travels along the psoas muscle and ilium, then passes under or through the inguinal ligament just inside the anterior superior iliac spine (ASIS, the bony bump at the front of your hip). That passage is the most common site of entrapment.
Why Your Symptoms Match So Well
| Feature | Your Symptom | Meralgia Paresthetica |
|---|---|---|
| Location | Left mid and lateral thigh | Anterolateral thigh (LFCN distribution) |
| Trigger | Touch / mild pressure | Allodynia - classic feature |
| Spontaneous pain | No (only on touch) | Often absent or mild in chronic cases |
| Duration | Years | Can be long-standing / chronic |
| Side | Unilateral (left) | Usually unilateral |
| Leg weakness | None mentioned | None - nerve is purely sensory |
As stated in Rheumatology (2022, Elsevier): "Patients with meralgia paresthetica typically complain of burning pain and dysesthesia in the sensory distribution of the nerve... allodynia (increased sensitivity to light touch) is another manifestation."
What Causes the Nerve to Get Compressed?
Common contributing factors (any one of these can be responsible):
- Tight belts, waistbands, or clothing pressing on the groin
- Excess body weight / obesity - increases pressure on the nerve at the inguinal ligament
- Prolonged standing or walking
- Pregnancy (historical or current)
- Diabetes - can make nerves more vulnerable
- Prior abdominal or hip surgery (appendectomy, hernia repair, bariatric surgery)
- Occupational postures - sitting for long periods or supporting weight on the thighs
- Sometimes no identifiable cause at all (idiopathic)
Is It Anything Else?
A few other conditions to consider, though less likely given your description:
- L2-L3 lumbar radiculopathy - nerve root compression in the lower back can also cause lateral thigh symptoms, but usually comes with some back pain and may affect reflexes
- Femoral neuropathy - affects the front of thigh plus causes quadriceps weakness and a reduced knee reflex; your lack of weakness makes this less likely
- Fibromyalgia or myofascial pain - diffuse, bilateral; does not match your highly localized unilateral pattern
The fact that it is strictly localized, unilateral, only on touch, no weakness, no reflex change points squarely at a peripheral sensory nerve - i.e., the LFCN.
What Should You Do?
See a doctor (neurologist, sports physician, or GP). A clinical diagnosis is usually enough - no expensive tests needed. They may:
- Perform a pelvic compression test (repositioning the pelvis to change nerve tension and see if symptoms shift)
- Check sensory mapping of both thighs
- Occasionally order nerve conduction studies to confirm, though these are technically difficult for this nerve
- Order an MRI of the lumbar spine only if radiculopathy needs to be ruled out
Conservative treatment is usually effective:
- Loosen belts, waistbands, and clothing at the waist/hip
- Weight loss if applicable
- Avoid prolonged standing
- NSAIDs for pain relief
- Local anesthetic + corticosteroid injection near the inguinal ligament - both diagnostic and therapeutic
- Neuropathic pain medications (gabapentin, amitriptyline) for persistent cases
- Surgical decompression (neurolysis) is reserved for severe, chronic, unresponsive cases and is rarely needed
Important Note
The fact that this has lasted years without spreading, without leg weakness, and without worsening is actually reassuring - it suggests a stable, localized nerve irritation rather than something progressive. However, since it has persisted this long, you should get it evaluated. An untreated compressed nerve can occasionally worsen, and there may be a simple fixable cause (like a tight belt or posture habit).
Sources: Rheumatology 2-Volume Set (2022, Elsevier); Bradley and Daroff's Neurology in Clinical Practice; Dermatology 2-Volume Set 5e; Cleveland Clinic; POGO Physio
I thought it can tumor
Finding Sources
Finding Sources
Searching the Web
thigh tumor vs meralgia paresthetica differentiating features pain only on touch years
Finding Sources
Finding Sources
Finding Sources
Searching the Web
soft tissue tumor thigh red flags symptoms that distinguish from nerve pain
That concern is worth taking seriously, so here is a clear, honest comparison:
Could It Be a Tumor? Probably Not - But Here Is Why
The Reassuring Side: Your Symptoms Don't Match a Tumor Well
A soft tissue tumor (including sarcomas - the most serious type) in the thigh has a very different profile from what you describe:
| Feature | What You Have | Soft Tissue Tumor |
|---|---|---|
| Visible/palpable lump | Not mentioned | Almost always present - the lump itself is the first sign |
| Pain type | Only on touch, no spontaneous pain | Usually painless at first; pain only develops later as it grows and presses on nerves |
| Duration - size change | Years, presumably stable | Tumors grow over time - a sarcoma stable for years would be very unusual |
| Skin changes | None mentioned | May show visible swelling, skin changes |
| Location | Skin-level sensation | Tumors are usually deep in muscle tissue |
| Weakness | None | May develop as tumor compresses muscle/nerve |
Key point from Mayo Clinic on soft tissue sarcoma: "A soft tissue sarcoma may not cause any symptoms at first. As the cancer grows, it may cause: a noticeable lump or swelling." - The lump comes first, pain is secondary and late.
Your situation is the opposite - you have pain/sensitivity on touch with no lump mentioned, which is a nerve pattern, not a tumor pattern.
Red Flags for a Soft Tissue Tumor (That You Should Watch For)
According to UK and international oncology guidelines, the features that demand urgent investigation are:
- A visible or palpable lump (this is the #1 sign)
- Lump larger than 5 cm (about 2 inches)
- Lump that is growing in size
- Lump that is deep (feels buried in muscle, not just under the skin)
- New onset pain around a lump
- Lump returning after being removed
- Weight loss, fatigue, or night sweats (systemic signs)
If you have none of these, a tumor is very unlikely.
One Thing Worth Knowing: Tumors Can Occasionally Mimic Meralgia
There are rare case reports (published in Reumatologia Clinica) of internal masses - such as a retroperitoneal tumor or abdominal/pelvic mass - pressing on the lateral femoral cutaneous nerve from the inside, causing meralgia-like symptoms. In those cases, the symptoms are usually progressive and worsening, not stable for years.
Bottom Line
The combination of:
- No lump you can feel or see
- Pain only on touching the skin (surface sensation)
- Stable for years without progression
- Confined to the nerve territory of the lateral thigh
- Normal on the other side
...is a nerve problem (meralgia paresthetica), not a tumor.
However, since this has been present for years without a diagnosis, you should see a doctor anyway - not because a tumor is likely, but because:
- A doctor can physically examine the area and confirm no mass is present
- A nerve block can both confirm and treat meralgia paresthetica
- If there is any doubt, an ultrasound of the thigh (cheap, no radiation) will immediately show whether any mass exists under the skin
That single ultrasound scan would definitively rule out a tumor and give you peace of mind.
Can it be a bony tumor as I press hard against bone than this pain increased
Finding Sources
Finding Sources
Searching the Web
bone tumor femur thigh symptoms deep pressure tenderness bony vs nerve pain differentiation
Finding Sources
Finding Sources
Finding Sources
Searching the Web
osteoid osteoma femur thigh pressure pain years benign bone tumor symptoms
Reading File
Reading File
Good - I have solid information now. Here is a thorough, honest answer:
Bony Tumor - A Fair Question, With an Important Distinction
The new detail - that pressing harder and deeper (against the bone) makes the pain worse - is worth examining carefully. Here is what it means and what it doesn't mean.
Why Deeper Pressure Hurts More: The Physics Explanation First
Before assuming bone involvement, understand this: when you press hard on the lateral mid-thigh, your fingertips progressively compress:
- Skin
- Subcutaneous fat
- The lateral femoral cutaneous nerve (which runs here)
- Fascia and muscle
- The femur bone (periosteum)
A compressed or irritated nerve will hurt MORE with harder pressure - not because the bone is diseased, but because more force = more pressure on the already-sensitive nerve. This is the same reason pressing harder on a bruise hurts more even though the bone is fine. So this finding alone does not confirm a bone problem.
Could It Be a Bone Tumor? Here Is the Honest Assessment
There are two relevant bone tumor types to consider:
1. Osteoid Osteoma (Benign - Most Relevant)
This is actually the one bone condition that best fits a years-long, localized thigh pain pattern. Key facts from Campbell's Operative Orthopaedics (2026) and Rheumatology (2022, Elsevier):
| Feature | Osteoid Osteoma |
|---|---|
| Location | Femur is the #1 site (along with tibia) |
| Pain character | Dull, aching, deep, localized to the tumor site |
| Night pain | Hallmark feature - worse at night, often wakes patient |
| Response to NSAIDs | Classic - dramatic relief with aspirin/ibuprofen |
| Duration | Can last years before diagnosis |
| Age | Most common ages 4-25, but can occur in adults |
| Malignant potential | None - never becomes cancerous |
| Size | Small (<1.5 cm), does not grow or spread |
The American Academy of Orthopaedic Surgeons confirms: "In some cases, a person will suffer the aching bothersome pain of an osteoid osteoma for years before seeing a doctor."
Ask yourself these two questions about osteoid osteoma:
- Is your thigh pain significantly worse at night - enough to wake you or disturb sleep?
- Does ibuprofen or aspirin make the pain noticeably better?
If both answers are yes - osteoid osteoma moves much higher on the list and you need an X-ray and likely CT scan urgently.
If both answers are no - osteoid osteoma is much less likely.
2. Malignant Bone Tumor (e.g., Osteosarcoma) - Much Less Likely
| Red Flag Feature | Your Situation |
|---|---|
| Constant, progressive pain (not just on touch) | You have pain ONLY on touch - not spontaneous |
| Visible swelling or lump over the bone | Not mentioned |
| Pain worsening over weeks/months | Stable for years |
| Night pain waking you | Not mentioned |
| Systemic symptoms - weight loss, fever, fatigue | Not mentioned |
| Pathological fracture | No |
A malignant bone tumor that has been present for years without progression, without spontaneous pain, without swelling - is very unlikely. Malignant bone tumors grow, cause escalating constant pain, and develop visible swelling.
Where This Leaves You: Updated Picture
| Diagnosis | Likelihood | Key Distinguishing Feature |
|---|---|---|
| Meralgia paresthetica (nerve) | Most likely | Touch-only pain, skin-level, no night pain |
| Osteoid osteoma (benign bone tumor) | Possible - needs ruling out | Night pain + dramatic NSAID relief |
| Malignant bone tumor | Unlikely | Stable for years, no swelling, no spontaneous pain |
What You Should Do Now
Since you have had this for years and are now concerned about bone involvement, the right step is:
- See a doctor and get a plain X-ray of the left femur - cheap, no radiation concerns, and an osteoid osteoma shows a characteristic appearance (small lucent nidus surrounded by thick bone). This one test rules in or out most bone pathology.
- If X-ray is inconclusive, a CT scan is the gold standard for identifying bone lesions.
- A normal X-ray + CT would essentially rule out any significant bony pathology and point back to the nerve as the cause.
The X-ray alone would give you a definitive answer and real peace of mind. That is the next logical step.
This is a shared conversation. Sign in to Orris to start your own chat.