PILON FRACTURE-STAGED MANAGEMENT CONCEPT
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pilon fracture" AND "staged management"
Reading File
Searching PubMed
"tibial pilon fracture" AND "staged protocol" AND "external fixator"
Searching Images
pilon fracture staged management external fixator ORIF tibial plafond
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have all the content needed for a comprehensive, detailed answer. Let me compile the full response.
Pilon Fracture — Staged Management Concept
Introduction & Historical Rationale
A pilon (tibial plafond) fracture involves the weight-bearing distal tibial articular surface, typically from axial loading where the talus acts as a pestle impacting the tibial ceiling. First described by Destot (1911) and further characterized by Rüedi et al. (1968), these remain among the most challenging orthopaedic trauma problems.
Early enthusiasm for immediate ORIF (1980s) was devastated by reports of massive wound complications, deep sepsis, osteomyelitis, and poor outcomes — as high as 50% poor results. This was caused by large surgical exposures on heavily traumatized, swollen soft tissue. The field cycled through external fixation alone, hybrid fixation, and then arrived at the modern staged protocol.
The seminal 1999 manuscript by Sirkin et al. formalized the two-stage approach: initial external fixator → soft tissue recovery → definitive ORIF. This yielded major complication rates of only 3% in closed and 11% in open fractures. Patterson and Cole corroborated the results, and the "Span, Scan, and Plan" philosophy became the standard of care.
Classification
Rüedi–Allgöwer (Classic):
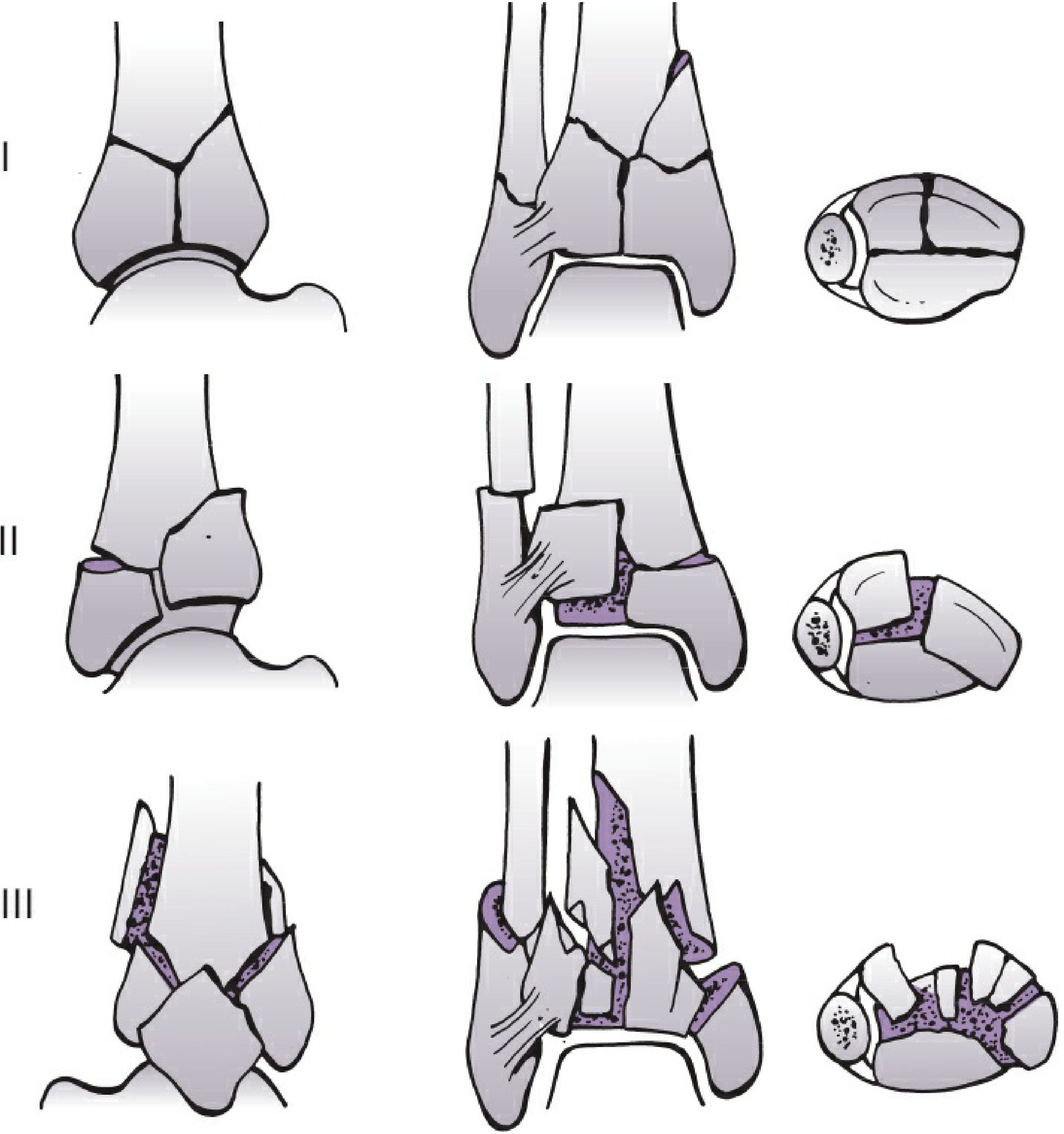
| Type | Description |
|---|---|
| I | Cleavage fracture, no significant articular displacement |
| II | Significant articular displacement without comminution |
| III | Impaction + comminution of the distal tibial articular surface |
AO/OTA Classification:
- 43A — Extra-articular
- 43B — Partial articular (one column)
- 43C — Complete articular (both columns disrupted, "true" pilon)
The C-type (especially C3) is the high-energy injury requiring staged management.
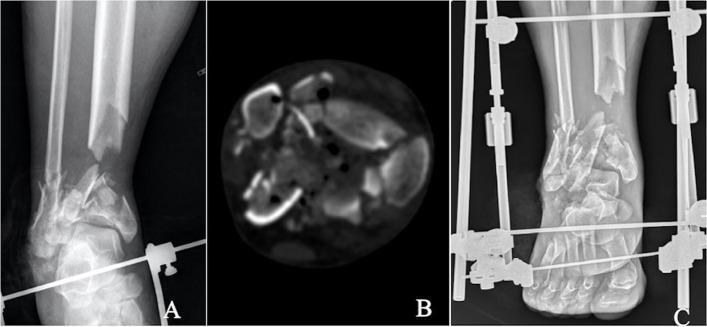
Staged Management Protocol
The Core Philosophy: "Span, Scan, and Plan"
- Span — Apply an ankle-spanning external fixator urgently
- Scan — Obtain CT scan of the distal tibia and fibula
- Plan — Plan definitive ORIF once soft tissues recover
Stage I: Ankle-Spanning External Fixator ± Fibular ORIF
Timing
Performed urgently — as soon as the patient's general condition permits (often within hours of presentation).
Goals of Stage I
- Restore limb length, alignment, and rotation
- Eliminate skin tenting and soft tissue distortion
- Relieve areas of ischemia from displaced osseous fragments
- Restore soft tissue length via ligamentotaxis
- Stability and alignment, NOT anatomic reduction (this is temporary)
Technique
- Proximal tibial shaft Schanz pin placed proximally
- Calcaneal pin placed via a medial-to-lateral direction, through both cortices, avoiding neurovascular structures
- Medial cuneiform pin to hold the foot in neutral
- Third short bar connecting cuneiform to calcaneal pin clamp with foot in neutral flexion
- Avoid overdistraction — this causes skin necrosis and painful dysesthesias
- Restoration of tibial length checked by reestablishing the normal relationship of the lateral talar process with the distal fibular tip
Fibula Fixation at Stage I
- Fibular plating at Stage I is advocated by most experts to provide a rigid lateral construct against coronal (varus/valgus) collapse
- Incision placed posterior to the fibula — critical to preserve a wide skin bridge ≥7 cm from any future anterior/medial incision
- Alternatives for poor lateral soft tissues: fibular nail, long K-wire, or long 3.5-mm screw percutaneously
Post-Stage I
- CT scan obtained immediately after frame application
- Patients reviewed at 1 week for soft tissue assessment and operative planning
- A first metatarsal pin can be added to the frame to prevent equinus if prolonged delay is anticipated
Soft Tissue Assessment — The Critical Interval
Surgery is typically delayed 10–21 days to allow:
| Sign | Significance |
|---|---|
| Wrinkle sign | Return of skin wrinkles on dorsum of foot → edema resolving, safe for incision |
| Blister re-epithelialization | Serous blisters → wait; blood-filled blisters → worse soft tissue injury |
| Fracture blister resolution | 10–14 days typically |
| Contusion resolution | May require 21 days |
New technologies (laser-assisted angiography, functional infrared thermal imaging) are emerging to objectively quantify soft tissue recovery, but remain investigational as of 2025.
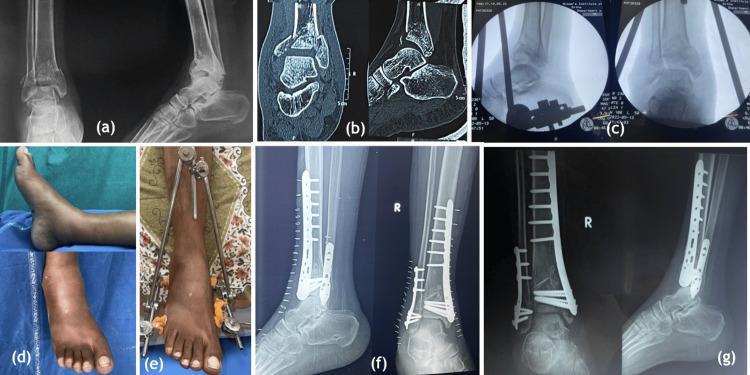
Stage II: Definitive ORIF of the Tibial Pilon
Timing
- 10–21 days after Stage I (based on soft tissue assessment, not a fixed number)
- When wrinkle sign returns and blisters have re-epithelialized
Three Overriding Surgical Goals
- Anatomic articular reduction
- Stable metaphyseal-diaphyseal fixation with acceptable alignment
- Avoidance of soft tissue complications
Preoperative Planning (CT-Based)
CT analysis drives the surgical tactic:
- Identify all fracture fragments and their size
- Determine which fracture lines are accessible through which approach
- Use the Column Theory to plan plate placement
Column Theory of the Distal Tibia
| Column | Anatomy | Importance |
|---|---|---|
| Medial | Medial tibial shaft → medial malleolus → plafond | Most common fixation site; medial plate |
| Lateral | Anterolateral tibia → Chaput tubercle → fibular notch | Fibula as lateral column; anterolateral plate |
| Posterior | Posterior tibia → posterior malleolus (held by Volkmann ligament to fibula) | Requires posterior plate if comminuted |
Most early failures result from inadequate fixation constructs or fixation placed on the wrong column.
Surgical Approaches
| Approach | Indication | Key Anatomy |
|---|---|---|
| Anterolateral | Lateral/anterior column fractures | Protects superficial peroneal nerve |
| Anteromedial | Medial column dominant fractures | Standard workhorse approach |
| Standard Anterior | Full plafond visualization | Protect deep peroneal nerve + anterior tibial artery at EHL level; EHL + NV bundle retracted laterally, AT tendon medially |
| Posterolateral / Posteromedial | Posterior malleolus fixation, posterior column | Can be added without skin compromise if original incision is midline (120° apart) |
Key rule: All incisions must maintain a skin bridge ≥7 cm between parallel incisions to prevent avascular necrosis of the intervening skin.
Implants
- Precontoured periarticular anterolateral and medial locking plates — placed with multiple epiphyseal screws, plate facilitates indirect metaphyseal reduction
- Small fragment plates (2.7, 3.5 mm) for articular reconstruction
- Tubular plates (1/3, 1/4 tubular) as supplemental medial implants
- Mini-fragment plates (2.0, 2.4 mm) for fine articular fragments
- Bone graft / allograft for metaphyseal voids after impacted fragment elevation
Articular Reconstruction Sequence
- Identify the key fragment — typically the posterior malleolus (largest articular piece, acts as the "keystone")
- Reduce and provisionally fix with K-wires
- Elevate impacted central fragments using the talus as a template
- Pack bone graft beneath elevated subchondral bone
- Lag screw fixation of articular surface
- Plate fixation of the articular block to the tibial shaft
When to Consider Alternative Strategies
| Situation | Alternative |
|---|---|
| Severe comminution + poor bone quality | Hybrid external fixation or circular/Ilizarov frame |
| Grossly contaminated open fracture | Staged: debridement → antibiotic spacer → delayed ORIF |
| Vascular injury requiring repair | Spanning ex-fix first, vascular repair, then staged ORIF |
| Patient unable to tolerate staged OR (polytrauma) | Damage control orthopaedics; minimal stabilization first |
| Nonambulatory patient / severe peripheral vascular disease | Nonoperative (casting/bracing) — outcomes poor regardless |
Nonoperative Management
Reserved for:
- Stable, truly nondisplaced fractures
- Extra-articular patterns
- Medically unwell patients (prohibitive perioperative risk)
- Nonambulatory patients
- Severe peripheral vascular disease / poorly controlled diabetes with non-healing risk
Cast immobilization cannot maintain alignment, length, or rotation reliably. Even for nonoperative cases, spanning external fixation is often preferable to casting.
Complications
| Complication | Key Points |
|---|---|
| Wound dehiscence / necrosis | Most common; staged approach reduces but does not eliminate |
| Deep infection / osteomyelitis | Requires aggressive debridement ± hardware removal |
| Posttraumatic arthritis | Occurs even with anatomic reduction due to chondrocyte apoptosis from initial axial impaction; may ultimately require ankle arthrodesis or TAR |
| Malunion | Usually varus/valgus or sagittal plane deformity from inadequate column fixation |
| Nonunion | More common in open injuries, smoking, diabetes, bone loss |
| Pin tract infection (ex-fix) | Daily pin care; resolve before Stage II |
Summary Algorithm
High-energy pilon fracture
↓
Assess soft tissue + neurovascular status
↓
STAGE I (urgent): Spanning ankle ex-fix ± fibular ORIF
↓
CT scan → preoperative planning
↓
Soft tissue recovery: Wait for wrinkle sign (10–21 days)
↓
STAGE II (definitive): ORIF — anatomic articular reconstruction
├─ Key fragment first (posterior malleolus)
├─ Elevate impaction + bone graft
├─ Lag screws → articular block
└─ Column-based plate stabilization
↓
Postop: NWB × 10–12 weeks, progressive ROM
Source: Rockwood and Green's Fractures in Adults, 10th ed. (2025), Chapter 64 — Tibial Pilon Fractures.
This is a shared conversation. Sign in to Orris to start your own chat.