Hoffas fracture
Reading File
Finding Sources
Searching PubMed
Hoffa fracture coronal femoral condyle
Searching the Web
Hoffa fracture coronal plane femoral condyle classification treatment 2024
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
I now have comprehensive information. Let me compile the full answer.
Hoffa Fracture
Definition
A Hoffa fracture is an intra-articular coronal plane shear fracture of the posterior femoral condyle - either lateral, medial, or both. The fracture line runs coronally, detaching the posterior portion of the condyle as a free intra-articular fragment. It accounts for roughly 0.65% of all femur fractures.
The injury was first described anatomically by Friedrich Busch in 1869 and later popularized by Albert Hoffa (1888), whose name is commonly attached to it. It is sometimes called a "Busch-Hoffa fracture."
Imaging: Lateral X-ray vs. CT
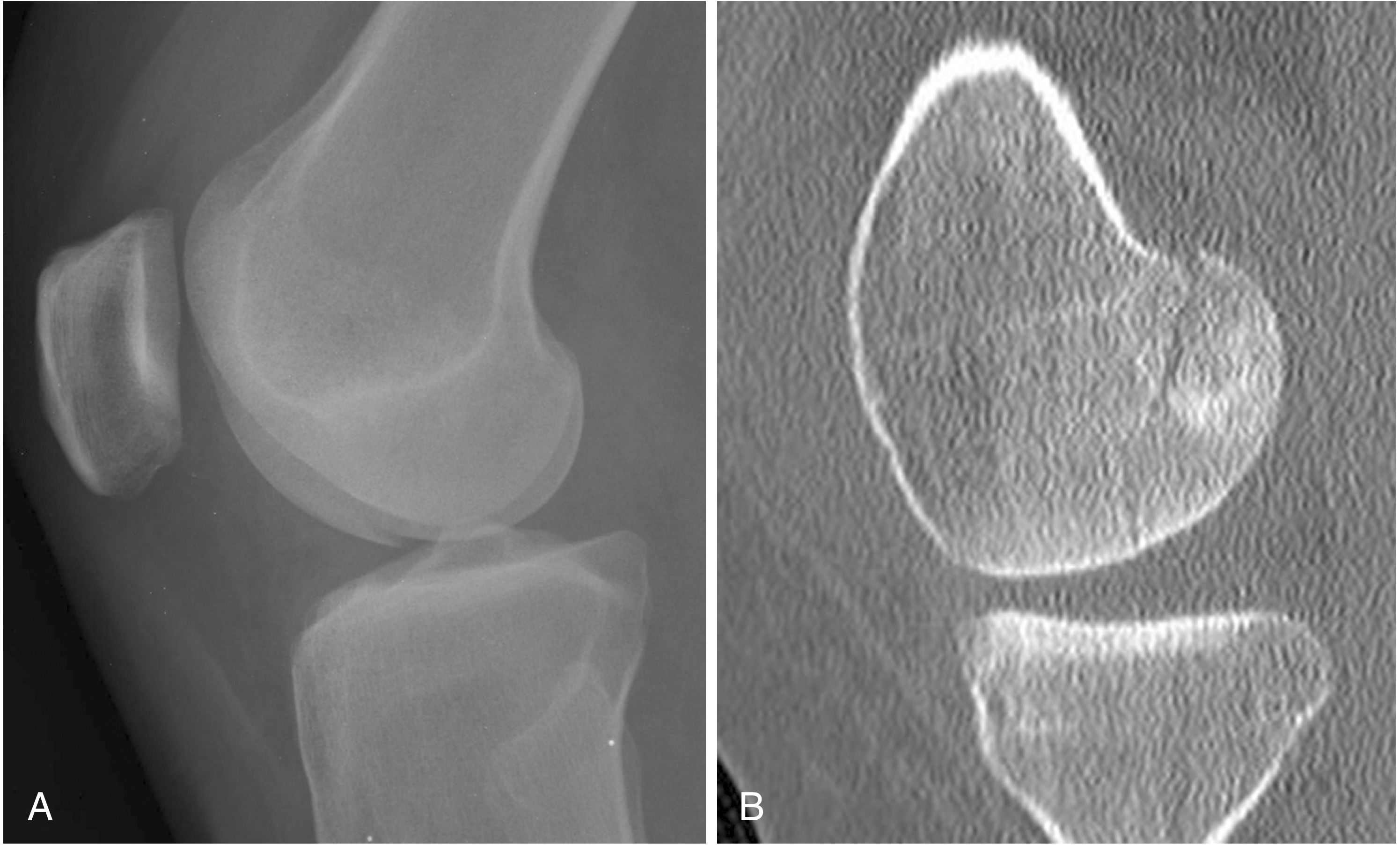
Figure: (A) Lateral radiograph - very subtle articular deformity. (B) Sagittal CT - clearly shows the coronally oriented intra-articular Hoffa fracture of the medial femoral condyle.
(Campbell's Operative Orthopaedics 15th ed., Fig. 3.52)
Mechanism
- High-energy axial loading with the knee in flexion - a translational shearing force acts on the posterior femoral condyle
- Seen in motor vehicle accidents, falls from height
- The lateral condyle is more commonly affected than the medial
- Frequently associated with other ipsilateral injuries: supracondylar fractures, intercondylar fractures, ligamentous injuries, patellar fractures
Why It Gets Missed
- Because the fracture is in the coronal plane, it is nearly invisible on AP radiographs and appears only as a subtle "double density" sign
- Studies show a 40% rate of coronal plane Hoffa fractures in intercondylar distal femur fractures, with approximately 31% missed on plain films - Rockwood & Green's 10th ed., p. 2025
- CT scan is mandatory for any distal femur fracture - sagittal and axial reconstructions reveal the fracture clearly
Plain X-ray clues:
- "Double density" sign on AP view (overlapping bony fragments)
- "Paradoxical notch view" - articular fragment visible in recurvatum on AP
Classification
Letenneur Classification (most widely used)
| Type | Description |
|---|---|
| I | Fracture line passes through the full extent of the posterior condyle (large fragment, entire posterior condyle) |
| II | Fracture only of the posterior condyle articular surface (small osteochondral fragment) |
| III | Fracture through the popliteal surface of the condyle, not fully articular |
Proposed Radiological Classification (SICOT, 2019) - based on fragment size & configuration:
| Type | Description |
|---|---|
| 1 | Fracture at or near the junction of posterior condyle and femoral shaft; fragment >2.5 cm from posterior condyle tip |
| 2 | Fracture posterior to that junction; fragment <2.5 cm |
| 3 | Comminuted coronal fractures |
| 4 | Special types: anterior lip Hoffa, bicondylar Hoffa, marginal osteochondral Hoffa, Hoffa + supracondylar fracture |
Type 4d (Hoffa + supracondylar fracture) is seen in up to 38% of cases and mandates longer, more rigid fixation constructs.
OTA/AO Classification Context
Hoffa fractures correspond to OTA/AO Type B3 (partial articular, coronal shear). They may coexist with Type C (complete articular) fractures of the distal femur.
Treatment
Non-operative
Reserved only for truly non-displaced fractures - extremely uncommon. Strict immobilization with close radiological follow-up.
Surgical (standard of care for all displaced fractures)
Fixation principle: Anteroposterior (AP) compression screws - countersunk beneath the anterior articular cartilage to avoid intra-articular protrusion.
- Implants: 2.7- or 3.5-mm cortical lag screws, or headless compression screws (e.g., Acutrak, Herbert), inserted anterior-to-posterior and countersunk below the articular surface
- A minimum of 2 screws are used to prevent rotation
- If a non-articular posterior spike is present, a small antiglide plate can be used there
- For very small fragments with no solid screw purchase: posterior-to-anterior screws may be placed
Surgical approach:
| Scenario | Approach |
|---|---|
| Isolated lateral Hoffa, no comminution | Limited lateral arthrotomy / subvastus approach |
| Isolated medial Hoffa | Medial parapatellar or posteromedial approach |
| Associated supracondylar/intercondylar fracture | Swashbuckler (modified anterior) or lateral parapatellar arthrotomy - extensile |
| Complex/comminuted | Open arthrotomy with locked buttress plate + lag screws |
"If any displacement of Hoffa fracture is present or other parts of the distal femur are to be addressed, then an extensive approach is necessary." - Rockwood & Green's 10th ed.
Key technical points:
- Restore articular congruity anatomically - even small steps lead to post-traumatic arthritis
- Flex the knee to relax the posterior capsule and aid reduction
- Countersink screws flush with or below articular cartilage
- For associated distal femur fractures: fix the Hoffa fragment first, then address the supracondylar component
Complications
| Complication | Notes |
|---|---|
| Missed diagnosis | Most common; CT is the solution |
| Osteonecrosis | The posterior condyle has a tenuous blood supply; displaced fragments may lose vascularity |
| Post-traumatic arthritis | From articular malreduction |
| Arthrofibrosis | From prolonged immobilization; early ROM is protective |
| Nonunion/malunion | Rare with rigid fixation; salvage with reconstructive osteotomy described for medial Hoffa malunion (Campbell's 15th ed.) |
| Screw protrusion | Avoided by careful countersinking |
Key Pearls
- Always get CT for intercondylar distal femur fractures - 40% have an occult Hoffa fragment
- Lateral condyle > medial condyle (ratio approximately 3:1)
- Screws go anterior to posterior, countersunk below cartilage
- Bicondylar Hoffa (both condyles involved) is rare but demands bilateral fixation
- When Hoffa + supracondylar fracture coexist, use locked buttress plate construct augmented by lag screws
- Early range of motion after fixation prevents arthrofibrosis - current evidence supports early/immediate weight-bearing does not increase fixation failure
Recent Literature
A 2023 systematic review (PMID 38050206) reviewed Busch-Hoffa fractures comprehensively. A 2025-2026 review by Gavaskar et al. in JAAOS (PMID 40550107) covers current surgical treatment strategies and is the most up-to-date summary available, with an accompanying AAOS video published January 2026.
Sources: Rockwood & Green's Fractures in Adults, 10th ed. 2025; Campbell's Operative Orthopaedics, 15th ed. 2026; SICOT-J 2019 classification review; OTA Core Curriculum V5.
This is a shared conversation. Sign in to Orris to start your own chat.