Brachial plexus block
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete, well-structured answer:
Brachial Plexus Block
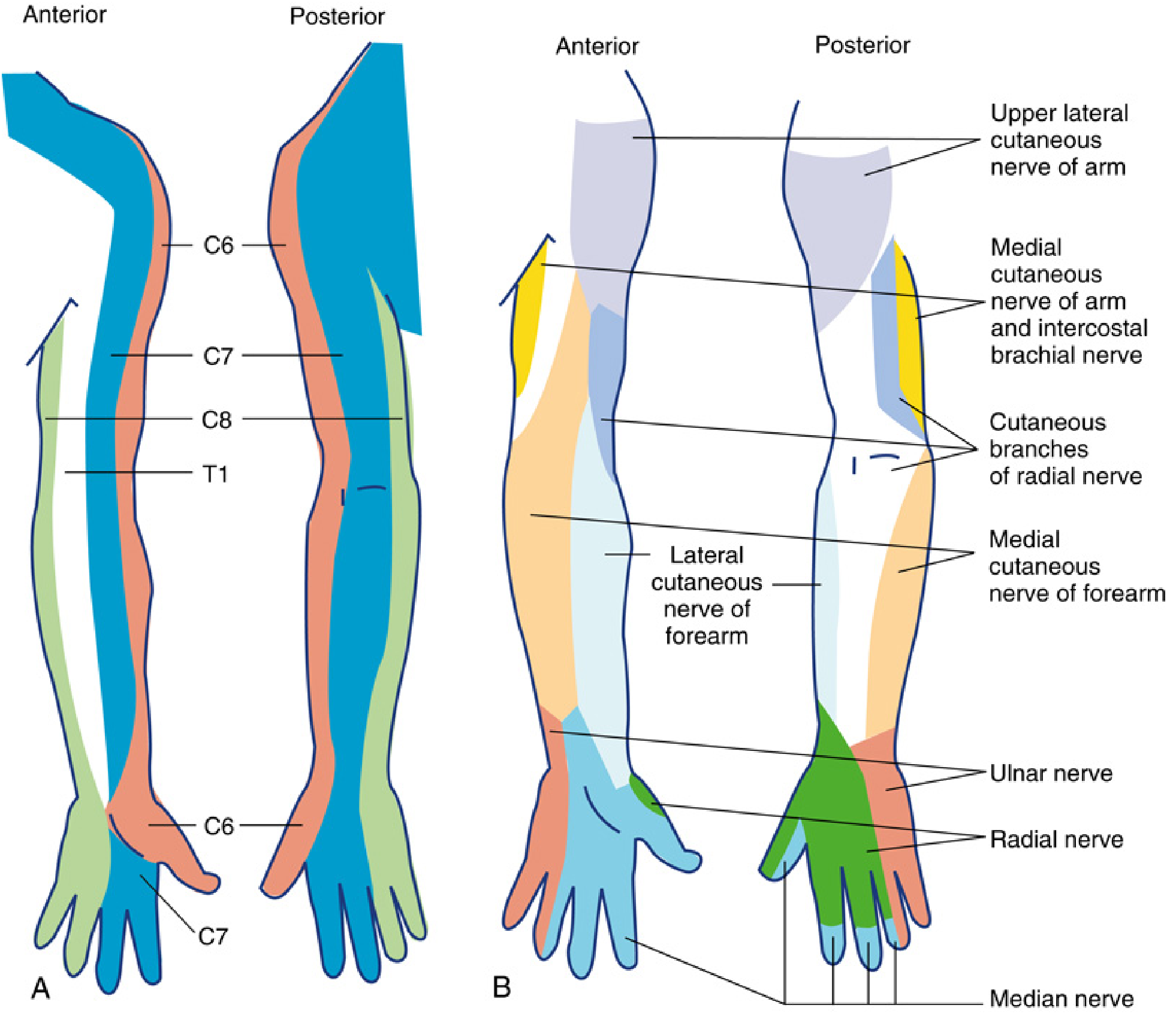
Anatomy of the Brachial Plexus
The brachial plexus arises from the ventral rami of C5-T1. These roots emerge between the anterior and middle scalene muscles and converge to form three trunks (superior, middle, inferior), each dividing into anterior and posterior divisions, which then recombine into three cords (lateral, posterior, medial) named by their relation to the axillary artery.
At the lateral border of pectoralis minor, the cords give rise to the terminal nerves:
- Lateral cord → musculocutaneous nerve + lateral head of median nerve
- Medial cord → ulnar nerve + medial head of median nerve + medial cutaneous nerves of arm and forearm
- Posterior cord → axillary nerve + radial nerve
Approaches - Overview
Blocks above the clavicle (interscalene, supraclavicular) target the ventral rami, trunks, and divisions. Blocks below the clavicle (infraclavicular, axillary) target the cords and terminal nerves. Ultrasound guidance has blurred these anatomic lines, enabling hybrid and selective nerve targeting.
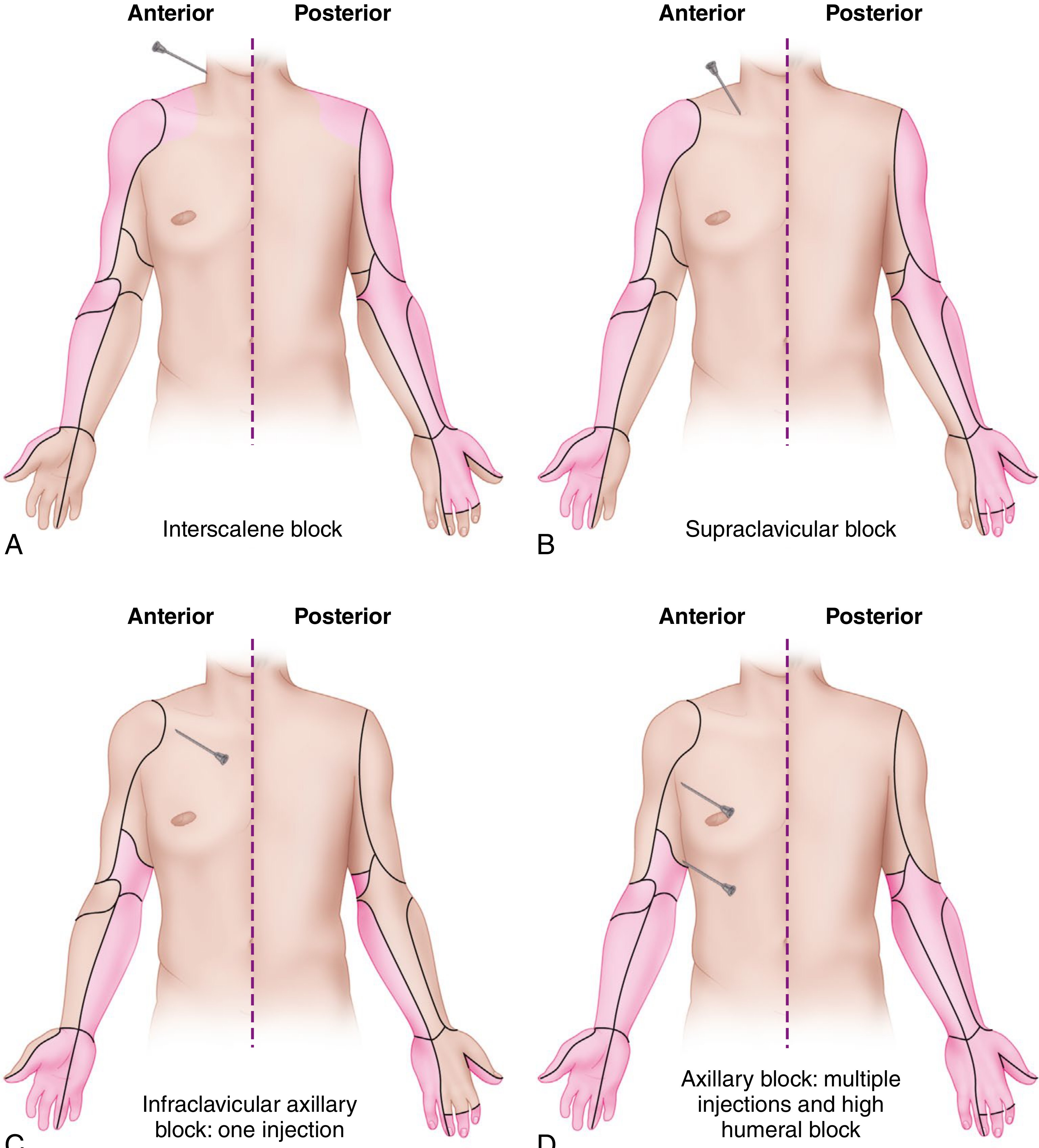
1. Interscalene Block (ISB)
Anatomy targeted: Superior and middle trunks (C5-C7 level; inferior trunk C8-T1 often incomplete)
Indications:
- Shoulder surgery (the preferred technique)
- Proximal humerus, clavicle, and acromioclavicular joint surgery
- Elbow surgery (with supplementation)
Technique (Ultrasound-Guided):
- Patient supine, head turned away from side to be blocked
- High-frequency linear probe placed at the supraclavicular fossa, then traced up the neck until trunks appear as hypoechoic structures between anterior and middle scalene muscles - the classic "stoplight" sign (three stacked circles)
- Needle inserted in-plane or out-of-plane; local anesthetic deposited within the periplexus space
Limitations: Not recommended for forearm/hand surgery (C8-T1 incomplete)
Side Effects and Complications:
| Complication | Notes |
|---|---|
| Phrenic nerve block | 100% incidence at traditional C6 level - ipsilateral hemidiaphragm paralysis is inevitable |
| Dyspnea/respiratory compromise | Symptomatic in patients with severe pulmonary disease or contralateral phrenic palsy |
| Bilateral ISB | Always contraindicated |
| Horner syndrome | Stellate ganglion block |
| Hoarseness | Recurrent laryngeal nerve block |
| Bezold-Jarisch reflex | Severe hypotension + bradycardia in awake sitting patients (beach chair position) |
| Epidural/intrathecal injection | Risk if performed under GA - should be done under light sedation |
| Pneumothorax | Low risk at C5-C6 due to distance from pleura |
Phrenic-sparing alternatives: The superior trunk block and anterior suprascapular nerve block target the suprascapular nerve (providing ~70% of shoulder joint innervation) with less phrenic nerve involvement. A low-dose (15 mL) superior trunk block shows noninferior pain scores with less hemidiaphragmatic paralysis vs. standard ISB. - Miller's Anesthesia 10e
2. Supraclavicular Block
Anatomy targeted: Distal trunks / proximal divisions (the plexus is most compact here - the "bottleneck")
Indications:
- Elbow, forearm, and hand surgery
- Considered the spinal of the upper extremity for rapid, reliable coverage
Technique (Ultrasound-Guided):
- Patient supine, head turned away, arm adducted
- High-frequency linear transducer just proximal to supraclavicular fossa
- Plexus appears as a cluster of hypoechoic circles lateral to the subclavian artery, above the first rib
- Needle advanced in-plane, lateral to medial
- Volume: 15-30 mL (higher volumes risk ischemic compression in this compact space)
- The first rib acts as a medial barrier protecting from reaching the pleural dome
Complications:
- Pneumothorax: 0.5-6% (risk persists even under ultrasound)
- Phrenic nerve block: 40-60%
- Horner syndrome
- Avoid in uncooperative patients or those who cannot tolerate any respiratory compromise
3. Infraclavicular Block
Anatomy targeted: Three cords of the brachial plexus (around the axillary artery)
Indications:
- Elbow, forearm, wrist, and hand surgery
- Preferred approach for catheter placement - stable location, extra muscle/fascial layers hold the catheter securely, arm manipulation not required
Technique (Ultrasound-Guided):
- Preferred: lateral sagittal (paracoracoid) approach - probe in parasagittal plane medial to the coracoid process
- Axillary artery visualized in short-axis, deep to pectoralis major and minor
- Needle placed posterior to the axillary artery (single injection)
- 30-40 mL posterior to the axillary artery provides complete plexus block
- Cords do NOT need to be directly visualized for success
- Costoclavicular approach (alternative): cords clustered lateral to first part of axillary artery; faster onset but higher pleural puncture risk
Complications:
- Deep block - steep needle angle makes tip visibility challenging
- Vascular puncture (accessory axillary vein lies adjacent to the lateral cord)
- No significant phrenic nerve block
- No arm positioning required (advantage over axillary)
4. Axillary Block
Anatomy targeted: Terminal nerves around axillary artery (median, ulnar, radial, musculocutaneous)
Indications:
- Forearm, wrist, and hand surgery
- Similar coverage to infraclavicular
Key Points:
- Brachial plexus block at the cord/terminal nerve level provides excellent anesthesia at or distal to the elbow; the upper arm and shoulder are NOT covered
- The intercostobrachial nerve (T2) is spared with all brachial plexus approaches - requires separate subcutaneous infiltration for medial arm tourniquet analgesia
- Nerves that branch proximal to the injection site are usually spared: axillary nerve, musculocutaneous nerve, medial brachial cutaneous nerve
- The musculocutaneous nerve (lateral forearm) can be independently blocked by infiltrating the coracobrachialis muscle
Technique:
- Arm abducted 90 degrees (may be difficult with trauma or contractures)
- Ultrasound-guided multiple injection: identify each terminal nerve around axillary artery
- Multiple injection > single injection for reliability
Contraindications:
- Infection in the axilla
- Axillary lymphadenopathy
- Axillary malignancy
Complications:
- Dysesthesias and "brachialgia" post-block (inform the patient)
- Lower complication rate vs. proximal approaches (no pneumothorax, no phrenic block)
Localization Techniques Compared
| Technique | Advantages | Disadvantages |
|---|---|---|
| Ultrasound guidance | Higher success, faster onset, fewer needle passes, less vascular puncture | Operator-dependent, limited plane of view |
| Nerve stimulator | Does not require expensive equipment | Lower success rate vs. ultrasound |
| Paresthesia | Simplest | Risk of nerve injury, less reliable |
A meta-analysis of 13 studies confirmed ultrasound-guided blocks were more successful, faster, with quicker onset and lower vascular puncture rates vs. neurostimulation. - Campbell's Operative Orthopaedics 15e
Local Anesthetic Selection
- Both short- and long-acting agents can be used
- Choice depends on agent, technique, and clinical preference
- For sustained analgesia: continuous catheter (infraclavicular preferred for catheter placement)
- Multiple-injection technique is more effective than single or double injection
- High volumes in compact spaces (supraclavicular) carry risk of ischemic neural compression
Approach Selection Summary
| Surgery Site | Preferred Block |
|---|---|
| Shoulder | Interscalene (ISB) |
| Shoulder (pulmonary compromise) | Superior trunk / anterior suprascapular |
| Proximal humerus / elbow | Interscalene or supraclavicular |
| Distal humerus, forearm, hand | Supraclavicular or infraclavicular |
| Wrist / hand (catheter needed) | Infraclavicular |
| Forearm / hand (simple, outpatient) | Axillary |
Sources:
- Miller's Anesthesia, 10e, Chapter 42 - Upper Extremity Regional Anesthesia
- Campbell's Operative Orthopaedics, 15e (2026) - Chapter 69: Brachial Plexus Blocks
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Chapter 46
- Barash's Clinical Anesthesia, 9e - Chapter 42
This is a shared conversation. Sign in to Orris to start your own chat.