Rntcp park
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough summary of RNTCP as covered in Park's Textbook of Preventive and Social Medicine:
RNTCP - Revised National Tuberculosis Control Programme
(Now renamed NTEP - National Tuberculosis Elimination Programme)
Background and Origin
India's National Tuberculosis Programme (NTP) had been in operation since 1962, but treatment success rates were unacceptably low with high death and default rates. Spread of multidrug-resistant TB further worsened the situation.
In 1993, the Government of India revitalized the NTP with assistance from international agencies, launching the Revised National TB Control Programme (RNTCP). It adopted the internationally recommended DOTS (Directly Observed Treatment Short-course) strategy as the most systematic and cost-effective approach.
RNTCP expanded rapidly and since March 2006 covers the entire country.
Objectives of RNTCP
- Achievement of at least 85% cure rate of infectious TB cases through DOTS
- Augmentation of case finding through quality sputum microscopy to detect at least 70% of estimated cases
Five Original DOTS Components
- Political will and administrative commitment
- Diagnosis by quality-assured sputum smear microscopy
- Adequate supply of quality-assured short-course chemotherapy drugs
- Directly Observed Treatment (DOT)
- Systematic monitoring and accountability
STOP TB Strategy (adopted 2006)
WHO announced the STOP TB strategy in 2006, which RNTCP adopted. Its components:
- Pursuing quality DOTS - expansion and enhancement
- Addressing TB/HIV and MDR-TB
- Contributing to health system strengthening
- Engaging all care providers
- Empowering patients and communities
- Enabling and promoting research (diagnosis, treatment, vaccine)
Renamed to NTEP
In 2014, the World Health Assembly approved the End TB Strategy (a 20-year programme aiming for zero TB deaths, disease, and suffering). In line with these End TB targets, RNTCP was renamed to National Tuberculosis Elimination Programme (NTEP).
NTEP Organizational Structure
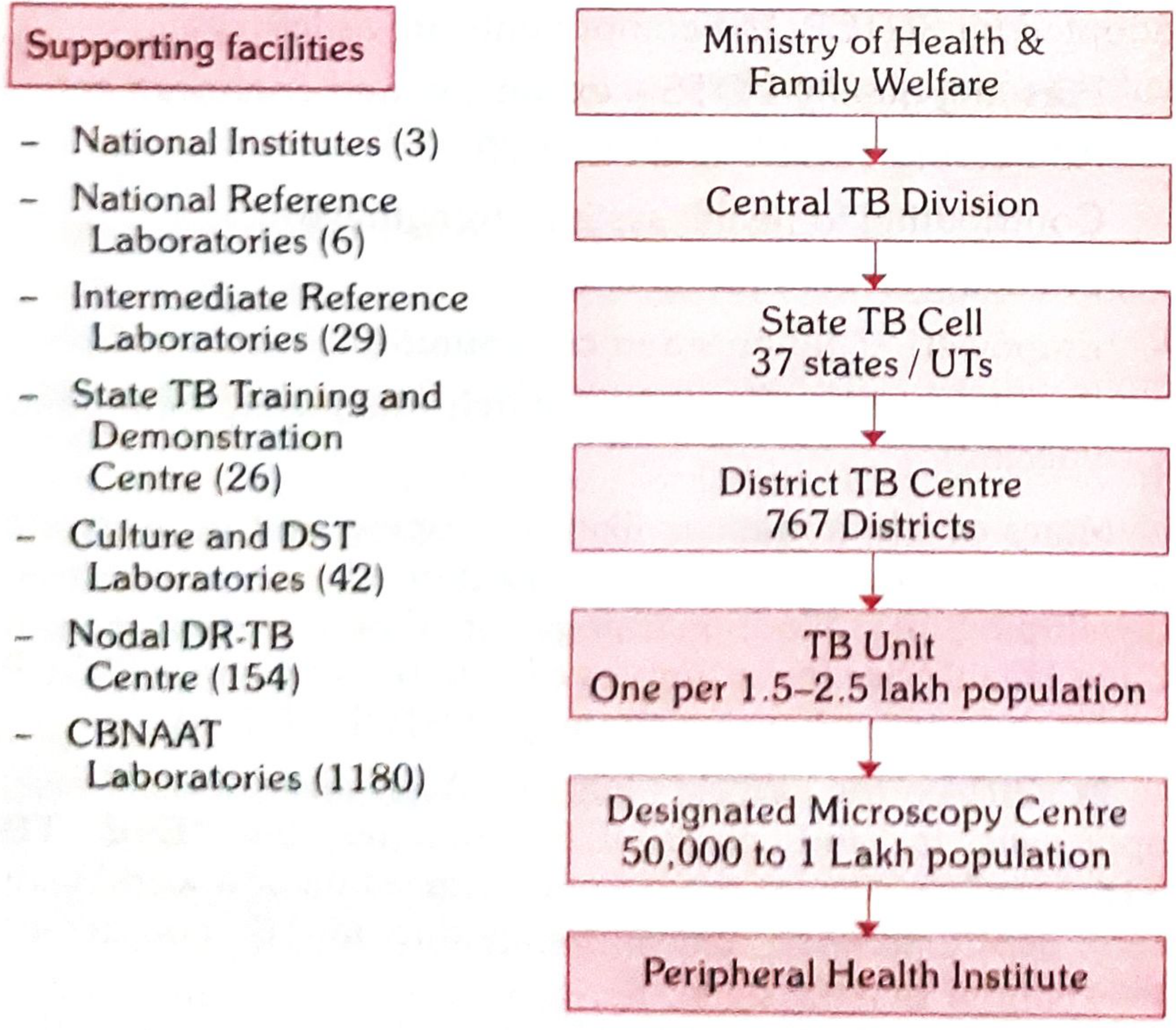
Fig. 2 - Organization structure of NTEP (Source: Park's)
The structure has 5 levels:
| Level | Key Body | Details |
|---|---|---|
| National | Central TB Division (CTD) | Under AS&DG (RNTCP & NACO); supported by 6 NRLs |
| State | State TB Cell (STC) + State TB Officer (STO) | 37 states/UTs; each has STDC with IRL |
| District | District TB Centre (DTC) + District TB Officer (DTO) | 767 districts |
| Sub-district | TB Unit (TU) | One per 1.5-2.5 lakh population |
| Peripheral | Designated Microscopy Centre (DMC) | One per 50,000-1 lakh population; also PHIs |
Supporting facilities:
- 3 National Institutes (NTI Bengaluru, NIRT Chennai, NITRD Delhi)
- 6 National Reference Laboratories (NRLs)
- 29 Intermediate Reference Laboratories
- 26 State TB Training and Demonstration Centres (STDCs)
- 42 Culture & DST Labs
- 154 Nodal DR-TB Centres
- 1,180 CBNAAT Laboratories
NTEP-Endorsed Diagnostics
- Smear microscopy for AFB (Ziehl-Neelsen or Fluorescence staining)
- Culture - Solid (LJ media) or Liquid (Middlebrook, BACTEC, MGIT)
- Rapid molecular tests - Line Probe Assay (LPA) or NAAT/GeneXpert (CBNAAT)
- Radiography (where available)
- Tuberculin skin test
New Initiatives under NTEP
1. NIKSHAY (IT Surveillance System)
- Case-based web application launched May 2012 by CTD + National Informatics Centre
- "NI-KSHAY" = eradication of TB (Hindi words)
- Functions: patient registration, diagnosis details, DOT provider tracking, HIV status, follow-up, outcome recording, DR-TB registration, referral/transfer, private sector notification, mobile app
2. Universal Drug Susceptibility Testing (DST)
- 1,180 CBNAAT machines expanded across all districts
- ~55% of all notified TB cases offered universal DST (Q3 2019)
3. Shorter Regimen and Bedaquiline (2018)
- Shorter regimen and Bedaquiline expanded for DR-TB
-
46,129 DR-TB patients on shorter regimen; >7,973 on newer drug-containing regimens
4. Campaign Mode - Active Case Finding
- Systematic screening of high-risk populations: tribal areas, slums, old age homes, prisons, orphanages, transit camps
5. Drug Packaging
- Drugs supplied in patient-wise boxes with full course in blister packs
- Intensive phase: one blister pack per day
- Continuation phase: one blister pack per week
- Color coding: Red = Category I; Blue = Category II
6. TB-HIV Coordination
- NACP and RNTCP adopted Isoniazid Prophylaxis Therapy (IPT) for prevention of TB among PLHIV
- HIV testing of TB patients jointly implemented since 2007-08
7. Integration with NPCDCS
- Integration for national strategy on TB and diabetes co-morbidities
Drug Resistance Surveillance (DRS, 2014-2016)
- MDR-TB prevalence: ~2.84% in new cases and ~11.60% in retreatment cases
- DR-TB management services started in 2007 (Gujarat and Maharashtra); scaled up nationally by March 2013
- DRTB Centres: Nodal DRTB Centres (NDRTBC) for seriously ill/new drug regimens; District DRTB Centres (DDRTBC) for MDR-TB and H mono/poly resistance
National Strategic Plan (NSP) 2017-2025
Vision: TB-free India with zero deaths, disease, and poverty due to TB
Objectives:
- Find all DS-TB and DR-TB cases (emphasis on private sector and high-risk undiagnosed)
- Initiate and sustain all patients on appropriate treatment with patient-friendly systems
- Prevent TB in susceptible populations
- Build enabling policies, empowered institutions, enhanced capacities
Key strategies:
- Private sector engagement
- Active case finding
- DR-TB case management
- Addressing social determinants including nutrition
- Robust surveillance
- Community engagement and multi-sectoral approach
Targets by 2025 (5 years ahead of SDG goal):
- 80% reduction in TB incidence (from 211/lakh to 43/lakh)
- 90% reduction in TB mortality (from 32/lakh to 3/lakh)
- 0% patients with catastrophic expenditure due to TB
Strategic pillars: DTPB - Detect - Treat - Prevent - Build
Financial Support
The programme receives support from the World Bank, DFID (via WHO), and the Global TB Drug Facility (GDF).
Public vs. Private Sector
| Public Sector | Private Sector | |
|---|---|---|
| Advantages | Free diagnosis, free treatment, standardized regimen, referral system, supervision, accountability | Wide choices (>5 lakh practitioners), better access, convenient timings, personal attention |
| Disadvantages | Staff non-response to symptoms, delays in results, travel expenditure, perceived low quality | High costs, irrational prescriptions, no adherence tracking, fear of losing patient if involved in RNTCP |
~70% of patients in India seek care from private clinics and hospitals (NSSO data).
Source: Park's Textbook of Preventive and Social Medicine, Chapter on National Health Programmes
This is a shared conversation. Sign in to Orris to start your own chat.