Moa of skeletal muscle relaxant succinylcholine
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a detailed explanation of the mechanism of action of succinylcholine, drawn from Miller's Anesthesia (10e), Katzung's Basic & Clinical Pharmacology (16e), and Barash's Clinical Anesthesia (9e):
Mechanism of Action of Succinylcholine (Suxamethonium)
Structure
Succinylcholine is structurally two acetylcholine molecules linked through their acetate methyl groups. This structural mimicry is the basis of its entire mechanism.
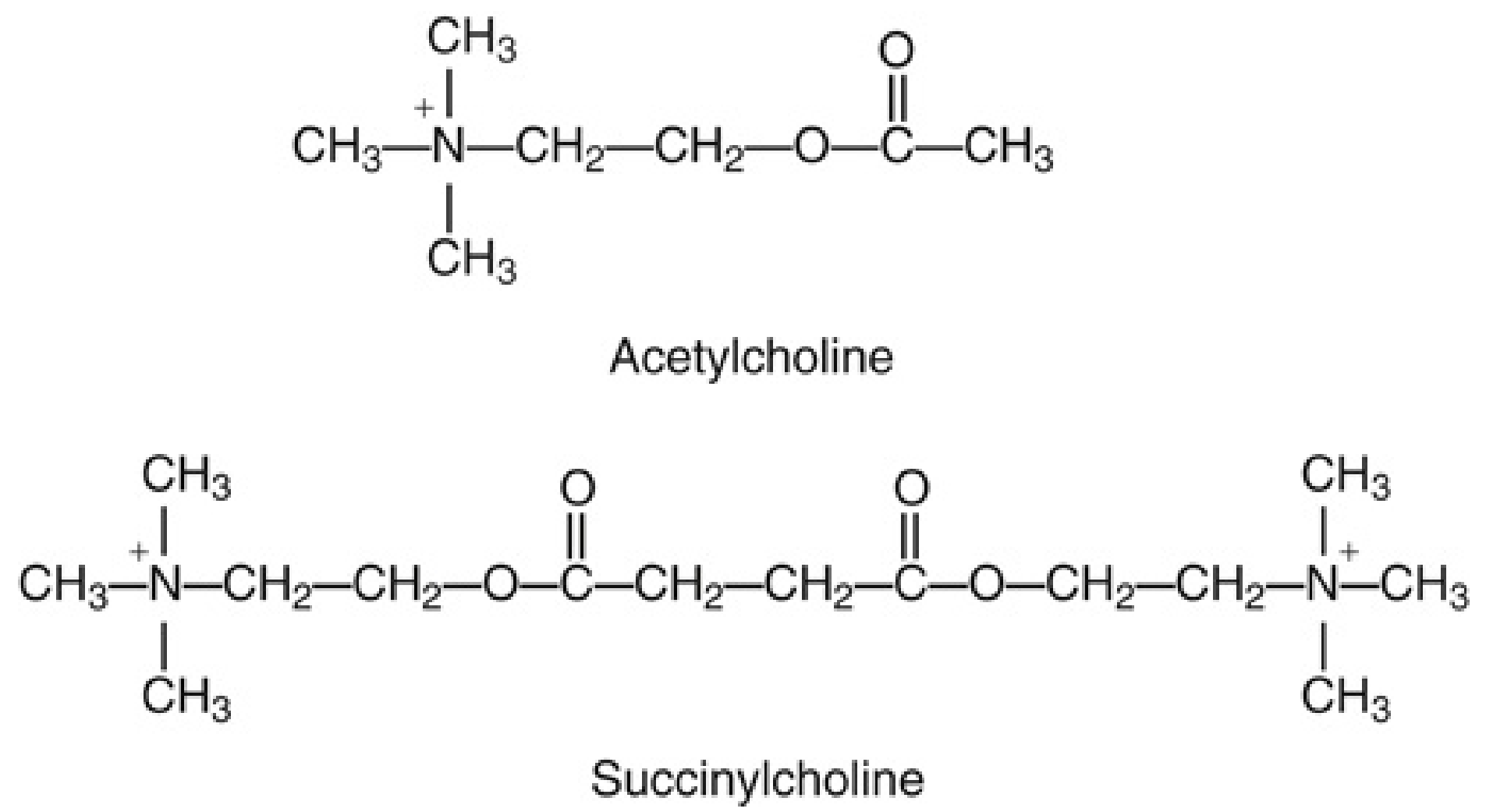
Succinylcholine = two acetylcholine molecules joined back-to-back. (Miller's Anesthesia, 10e)
Phase I Block (Depolarizing Block) - the Primary MOA
-
Binds nicotinic acetylcholine receptors (nAChR) at the neuromuscular junction (NMJ): Like acetylcholine, succinylcholine acts as an agonist at both postsynaptic (junctional) and extrajunctional nicotinic receptors. It binds the receptor and opens the ion channel, allowing Na⁺ influx and K⁺ efflux.
-
Causes sustained depolarization of the motor end plate: The initial channel opening generates an action potential that spreads to adjacent membranes, producing transient, visible muscle fasciculations (the brief twitching seen before paralysis sets in).
-
Resistance to hydrolysis at the synapse: Acetylcholine is rapidly destroyed by acetylcholinesterase (AChE) at the NMJ. Succinylcholine, however, is NOT metabolized by AChE - it is only metabolized in plasma by pseudocholinesterase (butyrylcholinesterase). Since there is little to no pseudocholinesterase at the motor end plate, succinylcholine persists and maintains continuous receptor activation.
-
Sustained depolarization → flaccid paralysis: The end plate membrane remains persistently depolarized. Adjacent voltage-gated sodium channels in the sarcolemma transition to their inactivated state and cannot be re-activated. Since excitation-contraction coupling requires end plate repolarization ("repriming") and repetitive firing to sustain muscle tension, a flaccid paralysis results.
The single-channel recording below illustrates this mechanism - at low concentrations succinylcholine causes discrete channel openings; at high concentrations it causes prolonged "flickering" as it repeatedly opens and blocks the channel:
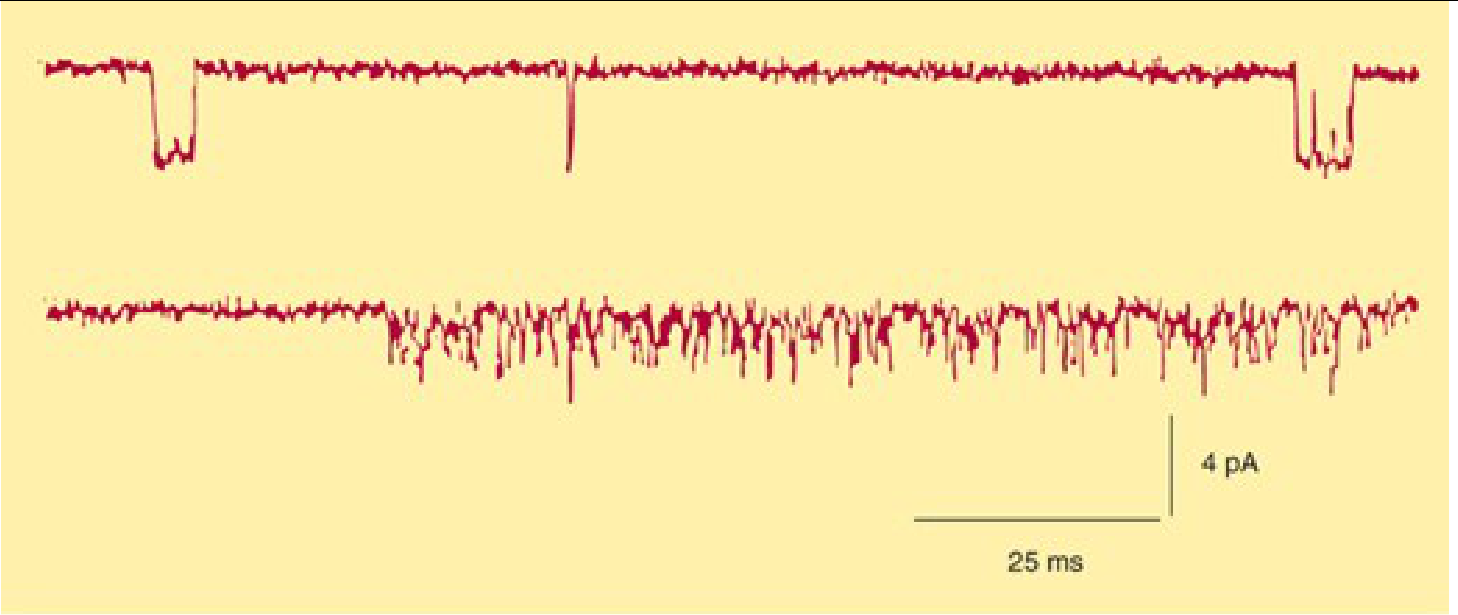
Upper trace: low dose - discrete channel openings. Lower trace: high dose - rapid flickering/blocking of channel. (Katzung, 16e, from Marshall et al., J Physiol 1990)
Phase II Block (Desensitization Block)
With prolonged or large-dose exposure (≥10× ED95, repeated doses, or continuous infusion), the mechanism shifts:
- The initial end plate depolarization decreases over time
- The membrane repolarizes, but cannot be easily depolarized again
- The receptor enters a desensitized/prolonged closed state
- The block now resembles a nondepolarizing block (fade on TOF and tetanic stimulation)
- This is called Phase II block (also historically called "dual block")
Key Distinctions from Nondepolarizing NMBDs
| Feature | Succinylcholine (Depolarizing) | Nondepolarizing (e.g., rocuronium) |
|---|---|---|
| Receptor action | Agonist - opens channel | Antagonist - blocks channel |
| Fasciculations | Yes (initial) | No |
| TOF fade | No (in Phase I) | Yes |
| Effect of neostigmine | Worsens Phase I block | Reverses block |
| Metabolism | Pseudocholinesterase (plasma) | Hepatic/renal/Hofmann |
| Onset | Fastest (~60 sec) | Slower |
Key Pharmacokinetic Points
- Only ~10% of the IV dose reaches the NMJ - the rest is hydrolyzed in plasma by pseudocholinesterase
- Metabolites: succinylmonocholine (weak NMBD) and choline
- Dose of 1 mg/kg produces complete block in ~60 seconds, with recovery to 90% strength in 9-13 minutes in patients with normal pseudocholinesterase
- Patients with atypical or reduced pseudocholinesterase (e.g., dibucaine-resistant variant) have prolonged block ("succinylcholine apnea")
Sources:
- Miller's Anesthesia, 10e - Pharmacology of Succinylcholine, p. 3228-3229
- Katzung's Basic & Clinical Pharmacology, 16e - Phase I Block, p. 754
- Barash's Clinical Anesthesia, 9e - Depolarizing NMB Drug: Succinylcholine, p. 1607-1609
This is a shared conversation. Sign in to Orris to start your own chat.