Short vermis height
Reading File
Finding Sources
Finding Sources
Searching the Web
short vermis height MRI cerebellar finding significance
Finding Sources
Finding Sources
Searching PubMed
vermis height cerebellar hypoplasia MRI measurement
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have enough information to give a thorough answer. Let me compile this.
Short Vermis Height
Short vermis height refers to a reduced craniocaudal (superior-to-inferior) dimension of the cerebellar vermis, measured on mid-sagittal MRI or ultrasound. It is a key biometric marker of vermian hypoplasia - underdevelopment of the central portion of the cerebellum.
What Is Vermis Height?
On a mid-sagittal view, the vermis is assessed for:
- Size: height (craniocaudal), depth (anteroposterior), and area
- Shape: normal lobular foliation vs. dysmorphic appearance
- Rotation: degree of tilt relative to the brainstem
- Fastigial point: the apex of the fourth ventricle
A "short vermis height" means the craniocaudal dimension falls below the expected range for gestational age (on fetal imaging) or age (on postnatal imaging). This is distinct from a normally sized but rotated vermis (as in a Blake pouch cyst).
Differential Diagnosis by Cause
Short vermis height fits within several diagnostic categories:
1. Dandy-Walker Malformation (DWM) Spectrum
The most recognized cause of hypoplastic/absent vermis. DWM features:
- Absent or severely hypoplastic vermis (often with upward rotation of the remnant)
- Cystic dilatation of the fourth ventricle filling the posterior fossa
- Enlarged posterior fossa with elevation of the torcular Herophili above the lambdoid suture
- Elevated tentorium
- Ventriculomegaly in 70-80% of cases
DWM is rare (1:30,000 births), presents in 4-12% of all infantile hydrocephaly cases, and results from developmental arrest at 4-6 weeks gestation. Associated CNS anomalies (corpus callosum agenesis, holoprosencephaly, heterotopias) occur in 50-70%. Chromosomal anomalies (trisomy 9, 13, 18, 21) are also associated.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 395-396
2. Vermian Dysgenesis
Incomplete vermis with normal torcular position (unlike DWM). The incomplete vermis may be rotated and does not cover the fourth ventricle. Loss of the normal fastigial point is the key imaging feature. Outcome varies: isolated inferior vermian dysgenesis carries a relatively good prognosis, but more severe forms cause profound neurologic impairment.
3. Joubert Syndrome and Related Disorders (JSRD)
Autosomal recessive ciliopathy causing:
- Hypoplastic vermis with midline vermian cleft
- Molar tooth sign on axial imaging: midbrain hypoplasia + deep interpeduncular fossa + failure of superior cerebellar peduncle decussation
- "Batwing" appearance of the fourth ventricle on axial cuts
- Neonatal hypotonia, tachypnoea/episodic hyperpnea, abnormal eye movements, developmental delay
- Over 30 clinical phenotypes; associated features include renal cysts, liver fibrosis, retinal dystrophy, and polydactyly
4. Pontocerebellar Hypoplasias (PCH)
A group of 11 genetic disorders (PCH1-11) with varying degrees of cerebellar and pontine hypoplasia:
- PCH2 (TSEN54 mutation): "dragonfly" cerebellum - marked cerebellar hemisphere atrophy with relative vermian sparing (so the vermis may be less affected)
- Other mutations: "butterfly" appearance with equal hemispheric and vermian involvement
- The pons is disproportionately small; cerebellar hemisphere cysts may be seen
5. Genetic/Neurometabolic Causes
Many autosomal recessive neurodegenerative conditions cause cerebellar hypoplasia with vermian involvement, including:
- Friedreich ataxia, ataxia-telangiectasia, oculomotor apraxia types 1 & 2
- Infantile neuroaxonal dystrophy (INAD / PLA2G6 mutation)
- Congenital disorders of glycosylation
- Nephronophthisis-related ciliopathies (NPHP genes - cerebellar vermis hypoplasia + retinitis pigmentosa)
6. Rhombencephalosynapsis
Rare malformation with fusion of cerebellar hemispheres across the midline and hypoplasia or aplasia of the vermis. Often associated with aqueduct stenosis and hydrocephalus.
Key Imaging Landmarks for Diagnosis
The table below summarizes how to differentiate common causes of short/absent vermis on mid-sagittal MRI:
| Feature | DWM | Vermian Dysgenesis | Blake Pouch Cyst | Joubert |
|---|---|---|---|---|
| Torcular elevation | Yes | No | No | No |
| Fastigial point | Absent/abnormal | Abnormal | Normal | Abnormal |
| Vermis | Absent/hypoplastic, rotated | Incomplete, may rotate | Normal structure, rotated up | Hypoplastic, cleft |
| Posterior fossa | Enlarged | Normal | Normal | Normal/small |
| Molar tooth sign | No | No | No | Yes |
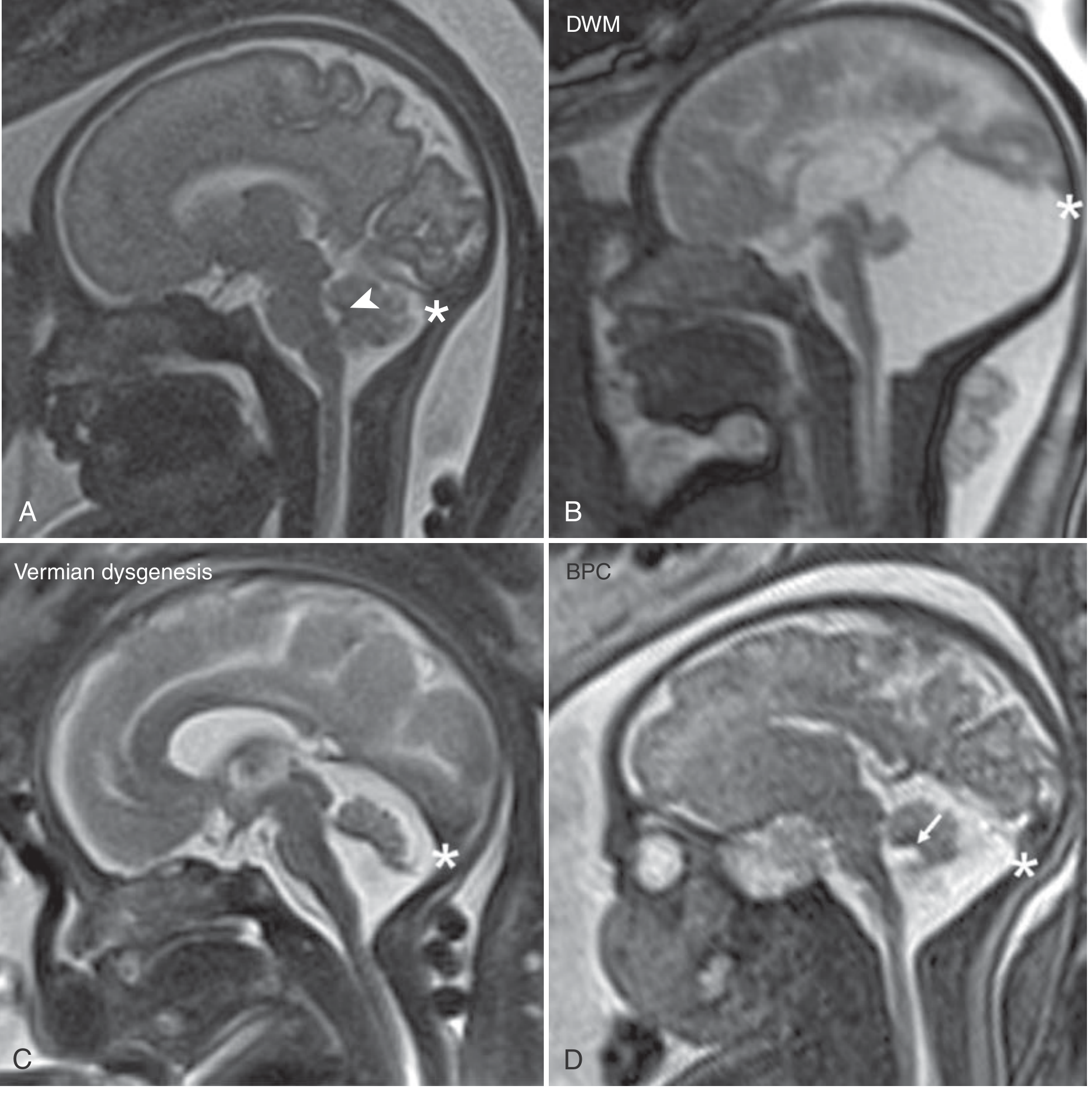
Mid-sagittal MRI: (A) Normal - note fastigial point (arrow) and torcular (asterisk). (B) Dandy-Walker malformation - torcular elevated. (C) Vermian dysgenesis - normal torcular, lost fastigial point. (D) Blake pouch cyst - fastigial point and torcular normal, vermis rotated away from brainstem. - Creasy & Resnik's Maternal-Fetal Medicine
Clinical Assessment
When short vermis height is found:
- Assess torcular position (elevated = DWM; normal = dysgenesis, Blake pouch, Joubert)
- Assess fastigial point (present = Blake pouch cyst; absent/abnormal = DWM or dysgenesis)
- Look for molar tooth sign on axial imaging (Joubert)
- Evaluate brainstem (pons size - PCH vs. isolated vermian hypoplasia)
- Assess supratentorial structures (corpus callosum, cortical foliation, ventricles)
- Genetic workup: karyotype, microarray, targeted gene panels (ciliopathy genes for JSRD)
- Fetal MRI is valuable when ultrasound is ambiguous, especially to detect associated anomalies and differentiate true hypoplasia from rotation artifact
Prognosis depends heavily on the underlying diagnosis and the severity and extent of associated anomalies. Isolated inferior vermian dysgenesis may have a good outcome, while DWM with associated CNS anomalies or chromosomal abnormalities carries a significantly worse prognosis.
- Grainger & Allison's Diagnostic Radiology, p. 1972-1974
- Creasy & Resnik's Maternal-Fetal Medicine, p. 370-371, 395-396
https://link.camscanner.com/27W89JJlD4
Reading Web Page
analyse_media
The link redirects to a CamScanner loading page rather than a directly accessible document or image - the content is loaded dynamically by a JavaScript app, so I can't extract the actual scanned document from it.
To help you, could you:
- Download the document from CamScanner and upload it directly here (as a PDF or image)
- Share the direct image URL if CamScanner gives you one (usually ends in
.jpgor.png) - Take a screenshot of the scanned document and attach it to your message
Once you share the actual file or image, I can read and analyze it right away.
This is a shared conversation. Sign in to Orris to start your own chat.