Naphthalene balls consumption path genesis and treatment in details
Reading File
Finding Sources
Searching PubMed
naphthalene toxicity poisoning treatment
Searching the Web
naphthalene balls toxicity pathophysiology hemolysis treatment clinical management
Reading File
Reading Article
PMID: 38231722
Reading File
Reading File
Finding Sources
I now have comprehensive information. Let me compile the full detailed answer.
Naphthalene (Mothball) Poisoning - Detailed Clinical Overview
1. What Is Naphthalene?
Naphthalene (C₁₀H₈) is a bicyclic aromatic hydrocarbon derived from the middle fraction of coal-tar distillation. It forms large, lustrous, crystalline white balls with a characteristic pungent odour and is used as:
- A pesticide/moth repellent (mothballs)
- A toilet/lavatory deodorant
- In the dye industry (indigo, azo dyes)
- In industrial solvents and fumigants
Key pharmacological identity: Naphthalene is a potent oxidant that stresses the erythrocyte redox system. It is distinct from the other common mothball compound, paradichlorobenzene (non-toxic). Differentiation tip: naphthalene balls melt in a water bath >80°C; paradichlorobenzene melts at 53°C.
2. Routes of Consumption / Exposure Pathways
Naphthalene is readily absorbed via ALL major routes:
A. Ingestion (Most common in children)
- Children mistake mothballs for candy or sweets
- Suicide attempts in adults (rare but reported)
- As little as one mothball can cause toxicity in a child
- Fatal dose: ~2 grams orally; fatal period: hours to 2-3 days
- Baby oils act as a solvent, significantly promoting absorption if naphthalene-contaminated clothing is worn by infants
B. Inhalation (Most common in adults)
- Volatilises readily at room temperature - creates persistent vapour
- Heavy dusting of bedclothes with naphthalene powder
- Occupational exposure in dye factories
- Prolonged presence in poorly ventilated rooms
C. Dermal Absorption
- Contact with contaminated bedding or clothing
- Naphthalene is NOT water-soluble (persists in garments after washing) but IS lipid-soluble
- Baby oils and skin creams massively accelerate dermal absorption in neonates
- Neonates are especially vulnerable because their metabolic capacity is immature
D. Transplacental / Neonatal Routes
- Maternal ingestion or inhalation can cause haemolytic anaemia in the foetus/newborn
- Cases of neonatal jaundice within 7 hours of birth have been documented after maternal exposure during the third trimester
3. Mechanisms of Toxicity (Pathogenesis)
Step 1 - Metabolic Activation
Naphthalene itself is not directly toxic. The liver metabolises it via cytochrome P450 (CYP1A1, CYP1A2, CYP2E1) to highly reactive intermediates:
- Naphthalene-1,2-epoxide (primary reactive metabolite)
- Naphthol (1-naphthol, 2-naphthol)
- Naphthalene dihydrodiol
- 1,2-Naphthoquinone (most oxidatively damaging)
These electrophilic metabolites react with cellular macromolecules and deplete glutathione.
Step 2 - Oxidative Stress on Red Blood Cells
- Reactive metabolites generate reactive oxygen species (ROS)
- ROS oxidise haemoglobin Fe²⁺ → Fe³⁺ = methaemoglobin (MetHb)
- MetHb cannot carry oxygen → functional anaemia + tissue hypoxia
- Continued oxidation causes precipitation of denatured Hb as Heinz bodies on the inner RBC membrane
- Heinz body-laden RBCs are destroyed in the spleen and microvasculature → intravascular haemolysis
Step 3 - The G6PD Connection (Critical)
The glutathione pathway is the RBC's primary defence against oxidative damage:
- G6PD (glucose-6-phosphate dehydrogenase) regenerates NADPH
- NADPH keeps glutathione in its reduced (protective) form
- In G6PD-deficient individuals, this defence is absent
- Result: naphthalene-induced haemolysis is dramatically amplified in G6PD deficiency
- G6PD gene is X-linked: males are more severely affected
Step 4 - Downstream Organ Damage
| Mechanism | Organ Affected | Result |
|---|---|---|
| Free Hb released from haemolysis precipitates as acid haematin crystals | Renal tubules | Acute tubular necrosis, AKI, pigment nephropathy |
| Direct toxic metabolite effects | Liver | Centrilobular necrosis, jaundice |
| MetHb + hypoxia | Brain | Confusion, seizures, coma |
| Oxidant injury | Lens | Naphthalene cataract (chronic) |
| Irritant vapours | Conjunctiva/lung | Conjunctivitis, pulmonary oedema |
4. Clinical Features
A. After Ingestion
Early (GI irritation phase):
- Nausea, vomiting, abdominal pain
- Burning sensation in throat and stomach
- Characteristic naphthalene odour on breath
Intermediate (haemolysis phase - hours to days):
- Pallor, fatigue, tachycardia
- Jaundice (haemolytic)
- Dark brown/black urine (haemoglobinuria)
- Dysuria, burning urethral pain, strangury
- Proteinuria/albuminuria
Severe/Late (multi-organ failure):
- Methaemoglobinaemia → central cyanosis unresponsive to supplemental O₂
- Acute kidney injury (oliguria/anuria)
- Hepatic necrosis
- Convulsions, altered consciousness, coma
- Cardiovascular collapse and death
B. After Inhalation
- Headache, malaise, nausea, vomiting
- Conjunctivitis, lacrimation
- Mental confusion
- Visual disturbances
- In severe/chronic cases: haemolytic anaemia, jaundice, haematuria
C. After Dermal Contact
- Dermatitis, skin irritation
- Conjunctivitis
- With large exposures: systemic haemolysis (especially in neonates)
D. Chronic Exposure
- Haemolytic anaemia
- Hepatic dysfunction
- Naphthalene cataract (bilateral posterior subcapsular lens opacity)
- Symptoms resolve 1-6 months after stopping exposure
5. High-Risk Populations
- Children - most common accidental victims; lower body weight means lower toxic threshold
- G6PD-deficient individuals - dramatically exaggerated haemolysis
- Neonates - immature metabolism, prone to neonatal jaundice and haemolysis
- Sickle cell disease/trait - additional oxidant vulnerability
- Pregnant women - risk to foetus via transplacental exposure
6. Diagnosis
Clinical
- History of naphthalene exposure + characteristic odour
- Unexplained haemolytic anaemia + dark urine + cyanosis not correcting with O₂
Laboratory Investigations
| Test | Expected Finding |
|---|---|
| CBC | Haemolytic anaemia, leukocytosis |
| Peripheral blood smear | Heinz bodies, fragmented RBCs (schistocytes) |
| Reticulocyte count | Elevated (compensatory) |
| LFTs | Elevated bilirubin (indirect), elevated transaminases |
| Urine | Haemoglobinuria, proteinuria, granular casts |
| Serum LDH | Markedly elevated |
| Haptoglobin | Decreased |
| Co-oximetry | MetHb fraction elevated (pulse oximetry unreliable - falsely normal) |
| G6PD screen | To identify high-risk patients |
| Renal function | Elevated creatinine, BUN in AKI |
7. Treatment
Immediate Decontamination
- Remove from exposure - fresh air immediately for inhalation
- Skin: flush with lukewarm running water for at least 20 minutes; remove contaminated clothing
- Eyes: irrigate copiously with water
- Ingestion - GI decontamination (if presenting within 1-2 hours):
- Activated charcoal (if airway is protected, no contraindication)
- Gastric lavage with warm water or normal saline
- Whole bowel irrigation may be considered for large ingestions
Supportive Care
- Keep patient warm (hypothermia worsens haemolysis)
- IV fluid hydration to maintain urine output and prevent tubular precipitation
- Monitor urine output, renal function, electrolytes
Alkaline Diuresis (Key Intervention)
- Administer sodium bicarbonate IV/orally to alkalinise urine (target urine pH >6.5)
- Alkaline urine prevents precipitation of acid haematin crystals in renal tubules
- Reduces risk of AKI from pigment nephropathy
Treating Methaemoglobinaemia
- Methylene blue 1-2 mg/kg IV (1% solution, slow push) - FIRST-LINE
- Reduces MetHb via NADPH-dependent pathway
- CONTRAINDICATED in G6PD deficiency - will worsen haemolysis (requires NADPH which is unavailable)
- Ascorbic acid (Vitamin C) 1-2 g IV - non-enzymatic MetHb reduction; used in G6PD deficiency when methylene blue is contraindicated
- N-acetylcysteine (NAC) - replenishes glutathione stores; used adjunctively (evidence limited but used in severe cases)
- Oxygen therapy - high-flow O₂ helps displace MetHb reduction; hyperbaric O₂ in severe cases
Treating Haemolytic Anaemia
- Packed red blood cell (PRBC) transfusion - for haemoglobin <7 g/dL or haemodynamic compromise
- In G6PD-deficient patients with MetHb: transfusion is the primary treatment (avoid methylene blue)
- Hydrocortisone - may help limit haemolysis (used adjunctively)
Managing AKI
- Forced alkaline diuresis
- Haemodialysis/CVVH for established AKI, anuria, or severe electrolyte abnormalities
- Naphthalene itself is dialysable (small molecule)
- Continuous venovenous haemofiltration (CVVH) has been used in severe cases
Managing Convulsions
- Benzodiazepines (diazepam, lorazepam) for seizure control
- Correct metabolic derangements (acidosis, electrolytes)
Summary Treatment Table
| Problem | Intervention |
|---|---|
| GI decontamination | Activated charcoal, gastric lavage |
| Alkalinise urine | IV sodium bicarbonate |
| MetHb (G6PD normal) | Methylene blue IV 1-2 mg/kg |
| MetHb (G6PD deficient) | Ascorbic acid IV + PRBC transfusion |
| Haemolytic anaemia | PRBC transfusion, hydrocortisone |
| AKI/pigment nephropathy | Forced diuresis, dialysis |
| Seizures | Benzodiazepines |
| Chronic cataract | Remove from exposure; ophthalmology referral |
8. Post-Mortem Findings
- Skin: yellow (jaundice)
- Gastric mucosa: yellow, congested, inflamed
- Liver: enlarged, congested, fatty degeneration / centrilobular necrosis
- Kidneys: severe damage, cortical pallor with tubular necrosis
- Other organs: generally congested
- Respiratory tract: signs of irritation if inhalation was the route
9. Medicolegal Aspects
- Accidental poisoning is the most common scenario - especially in children mistaking mothballs for candy
- Suicide by naphthalene ingestion has been reported but is uncommon
- Homicidal use is very rare
- Naphthalene persists in garments after washing (not water-soluble), making ongoing dermal exposure possible even after the primary source is removed
- Baby oil / skin oils act as vehicles dramatically increasing dermal absorption in infants
Sources: Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology, p. 678 | PC Dikshit Textbook of Forensic Medicine and Toxicology | Goldman-Cecil Medicine | Roberts and Hedges' Clinical Procedures in Emergency Medicine | Mathur & Garg, Acute Kidney Injury Following Naphthalene Poisoning, Saudi J Kidney Dis Transpl 2023 | UK PHE Naphthalene Toxicological Overview
When it is called methaemoglobinemia
Finding Sources
Searching the Web
methaemoglobinaemia definition percentage threshold clinical levels symptoms
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete, detailed answer:
Methaemoglobinaemia - When Is It Called That?
Definition
Methaemoglobinaemia is the clinical condition diagnosed when the proportion of methaemoglobin (MetHb) in the blood exceeds 1-2% of total haemoglobin.
Under normal physiology, <1% of circulating haemoglobin exists as methaemoglobin at any moment. This baseline arises because haemoglobin iron (Fe²⁺) is continuously being oxidised by ambient oxygen and other molecules, and is just as continuously being reduced back by enzymatic systems. The condition is declared when this balance tips, and MetHb accumulates above the normal threshold.
Different sources set slightly different cut-offs:
- >1-2% = condition exists (Tintinalli's Emergency Medicine)
- >5% = formal diagnosis of methaemoglobinaemia (European Journal of Cardiovascular Medicine; healthcare-bulletin.co.uk)
- >10% = clinically symptomatic methaemoglobinaemia (Goldman-Cecil Medicine)
In practice, most clinicians call it methaemoglobinaemia when MetHb exceeds 1-2% of total haemoglobin, and become clinically concerned when it crosses 10%.
The Core Biochemical Basis
Normal haemoglobin has iron in the ferrous state (Fe²⁺), which binds and releases oxygen freely.
When iron is oxidised to the ferric state (Fe³⁺), the resulting molecule is called methaemoglobin - it:
- Cannot bind oxygen for transport
- Shifts the oxygen-haemoglobin dissociation curve to the left (remaining Hb holds onto O₂ more tightly, releasing less to tissues)
- Results in functional anaemia + tissue hypoxia out of proportion to the haemoglobin level
Normal Protective Mechanisms (Why <1-2% is Normal)
The diagram below from Tintinalli's shows the two reduction pathways that continuously keep MetHb levels low:
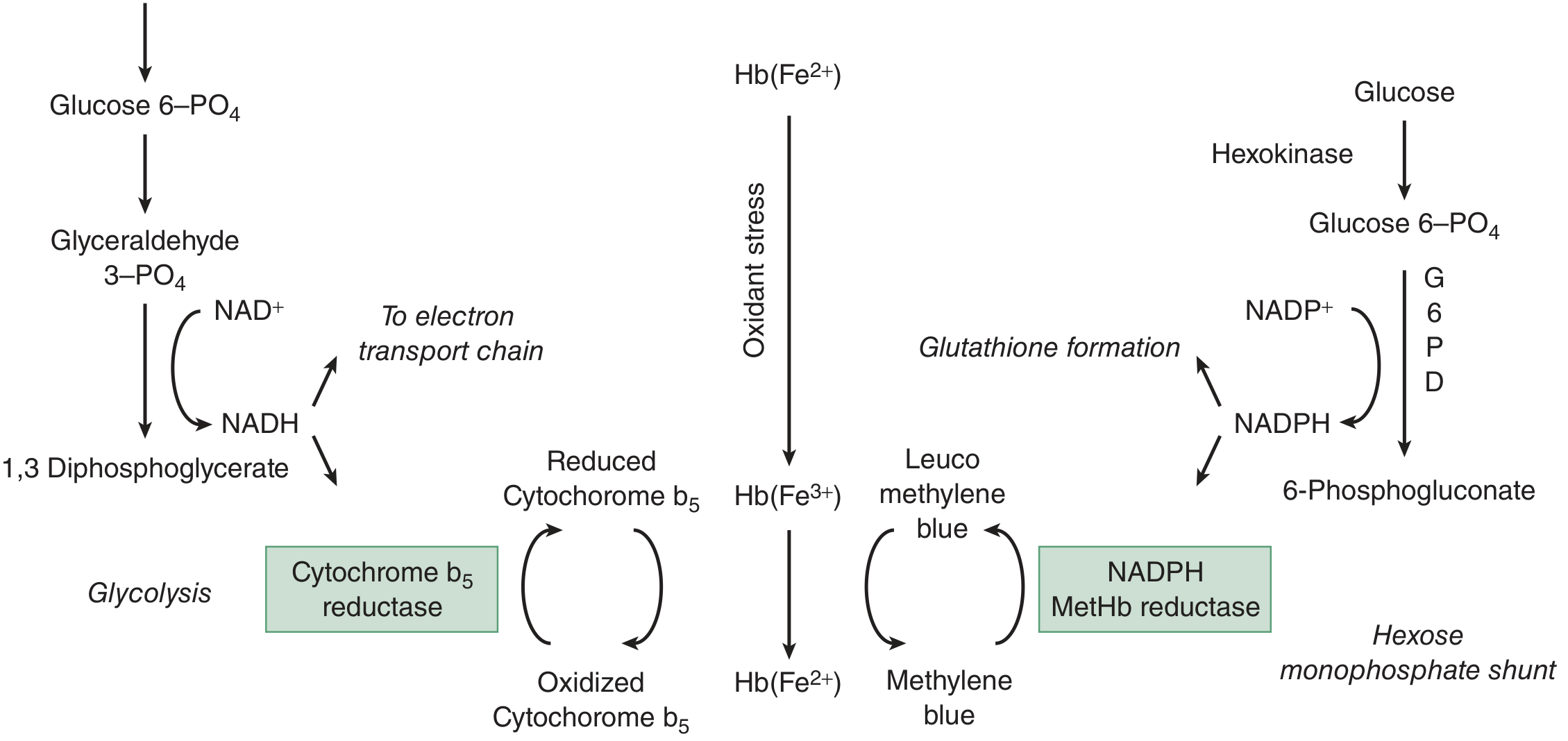
Pathway 1 - Cytochrome b5 reductase (NADH-dependent) - Primary, ~95%:
- Glycolysis produces NADH
- NADH donates electrons to cytochrome b5
- Reduced cytochrome b5 converts MetHb (Fe³⁺) back to Hb (Fe²⁺)
- This handles ~95% of MetHb reduction under normal conditions
Pathway 2 - NADPH-MetHb reductase (Hexose monophosphate shunt) - Minor, <5%:
- G6PD in the HMP shunt produces NADPH
- NADPH-MetHb reductase uses NADPH to reduce MetHb
- Normally minor - but this is the pathway methylene blue activates (methylene blue is reduced to leucomethylene blue by NADPH, which then reduces MetHb)
Minor non-enzymatic pathways: Vitamin C (ascorbic acid) and glutathione also contribute negligibly.
When Methaemoglobinaemia Occurs - Causes
Methaemoglobinaemia is triggered when oxidant stress overwhelms the cytochrome b5 reductase pathway:
Acquired (most common)
| Category | Examples |
|---|---|
| Drugs | Dapsone, primaquine, chloroquine, sulfonamides, nitrofurantoin, metoclopramide, benzocaine, lidocaine, prilocaine |
| Chemicals/toxins | Naphthalene (mothballs), aniline dyes, nitrites, nitrates, chlorates, phenols, paraquat |
| Environmental | Well water with high nitrates (infant methaemoglobinaemia), smoke inhalation |
| Medical use | GTN (nitroglycerin), nitric oxide (therapeutic), silver nitrate |
Congenital (rare)
- Cytochrome b5 reductase deficiency - autosomal recessive; the reduction pathway fails even without oxidant exposure; patients chronically cyanosed but often adapt well (tolerate MetHb 30-40%)
- Haemoglobin M (HbM) variants - mutations in α or β globin stabilise the iron in Fe³⁺ state; methylene blue is ineffective (the protein structure, not the enzyme, is the problem)
- Cytochrome b5 deficiency - rare
Clinical Severity - The Threshold Table
This is the key classification that defines when it becomes a clinical emergency:
| MetHb (% of total Hb) | Clinical State | Symptoms |
|---|---|---|
| <1-2% | Normal | None |
| 1-10% | Mild elevation | Usually asymptomatic; possible slight cyanosis at higher end |
| 10-20% | Mild MetHgb | Cyanosis (blue-grey skin), chocolate-brown blood visible at 15%; mild headache |
| 20-30% | Moderate | Anxiety, headache, light-headedness, tachycardia |
| 30-50% | Significant | Fatigue, confusion, dizziness, tachycardia, tachypnoea, dyspnoea |
| 50-70% | Severe | Coma, seizures, arrhythmias, respiratory depression, metabolic acidosis |
| >70% | Fatal | Death |
Important caveat: Symptom severity does not always map neatly to MetHb %. A patient with pre-existing anaemia, cardiovascular disease, or pulmonary disease may be severely symptomatic at MetHb 10-15%, because their baseline functional haemoglobin is already compromised.
Example from Tintinalli's: MetHb 1.5 g/dL in a healthy patient (Hb 15 g/dL) = 10% MetHb, functional Hb 13.5 g/dL - may be asymptomatic. The same 1.5 g/dL in an anaemic patient (Hb 8 g/dL) = 18.75% MetHb, functional Hb only 6.5 g/dL - severely symptomatic.
Key Diagnostic Clues
| Finding | Significance |
|---|---|
| Cyanosis that does NOT improve with supplemental O₂ | Classic hallmark - MetHb cannot carry O₂ |
| "Chocolate brown" arterial blood | Visible from ~15% MetHb; does not turn red on O₂ exposure |
| Pulse oximetry reads ~85% regardless of true saturation | SpO₂ falsely stabilises near 85% because MetHb absorbs 660nm and 940nm light equally |
| PaO₂ normal on ABG | Dissolved O₂ is fine; it is Hb-bound O₂ that is impaired |
| Co-oximetry - the definitive test | Directly measures MetHb fraction; ABG co-oximeter required, not standard pulse ox |
Treatment Threshold
Active treatment is indicated when:
- MetHb >30% regardless of symptoms, OR
- MetHb <30% with significant symptoms
Treatment: Methylene blue 1-2 mg/kg IV (activates NADPH-MetHb reductase pathway). Contraindicated in G6PD deficiency - use ascorbic acid + transfusion instead.
Sources: Tintinalli's Emergency Medicine, p. 1371 | Goldman-Cecil Medicine, p. 2188-2190 | RCEM Learning - Methaemoglobinaemia | StatPearls - Methemoglobinemia | Drug-induced methaemoglobinaemia - PubMed
This is a shared conversation. Sign in to Orris to start your own chat.