Histology of growth plate. Factors causing growth disturbance. Principles of guided growth modulation.?Answer this question for ms orthopaedic university exam 10 marks in handwritten notes image format
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Generating Image
Loading Image
Generating Image
Here are your MS Orthopaedics exam notes. Below is the complete typed version of all content for reference and study:
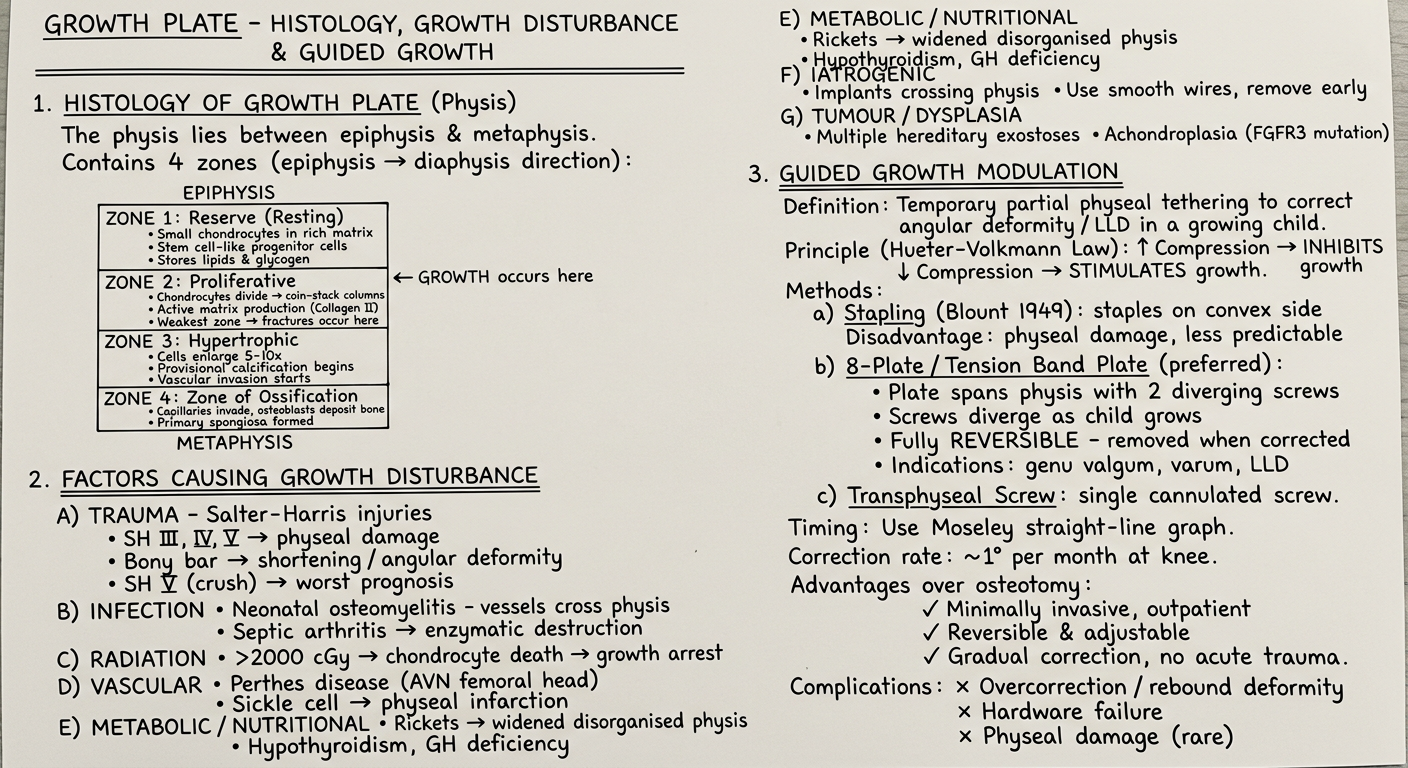
GROWTH PLATE (PHYSIS) - HISTOLOGY, GROWTH DISTURBANCE & GUIDED GROWTH MODULATION
1. HISTOLOGY OF GROWTH PLATE
The physis is a cartilaginous disc between epiphysis and metaphysis responsible for longitudinal bone growth. It has 4 zones arranged from epiphysis toward metaphysis:
| Zone | Key Features |
|---|---|
| Zone 1 - Reserve (Resting) | Small scattered chondrocytes; stem cell-like progenitor cells; stores lipids/glycogen; anchors physis to epiphysis |
| Zone 2 - Proliferative | Chondrocytes divide into "coin-stack" columns; most active growth zone; produces collagen type II; weakest zone - fractures occur here |
| Zone 3 - Hypertrophic | Cells enlarge 5-10x; three sub-zones: maturation, degeneration, provisional calcification; vascular invasion begins |
| Zone 4 - Ossification (Primary Spongiosa) | Capillary invasion; osteoblasts deposit bone on calcified cartilage scaffold; remodelled to secondary spongiosa |
Key point: Thickness of physis remains constant during growth - new cartilage produced = cartilage resorbed.
Here is a real histology image of the growth plate (picrosirius red stain, 17-week human fetal physis):
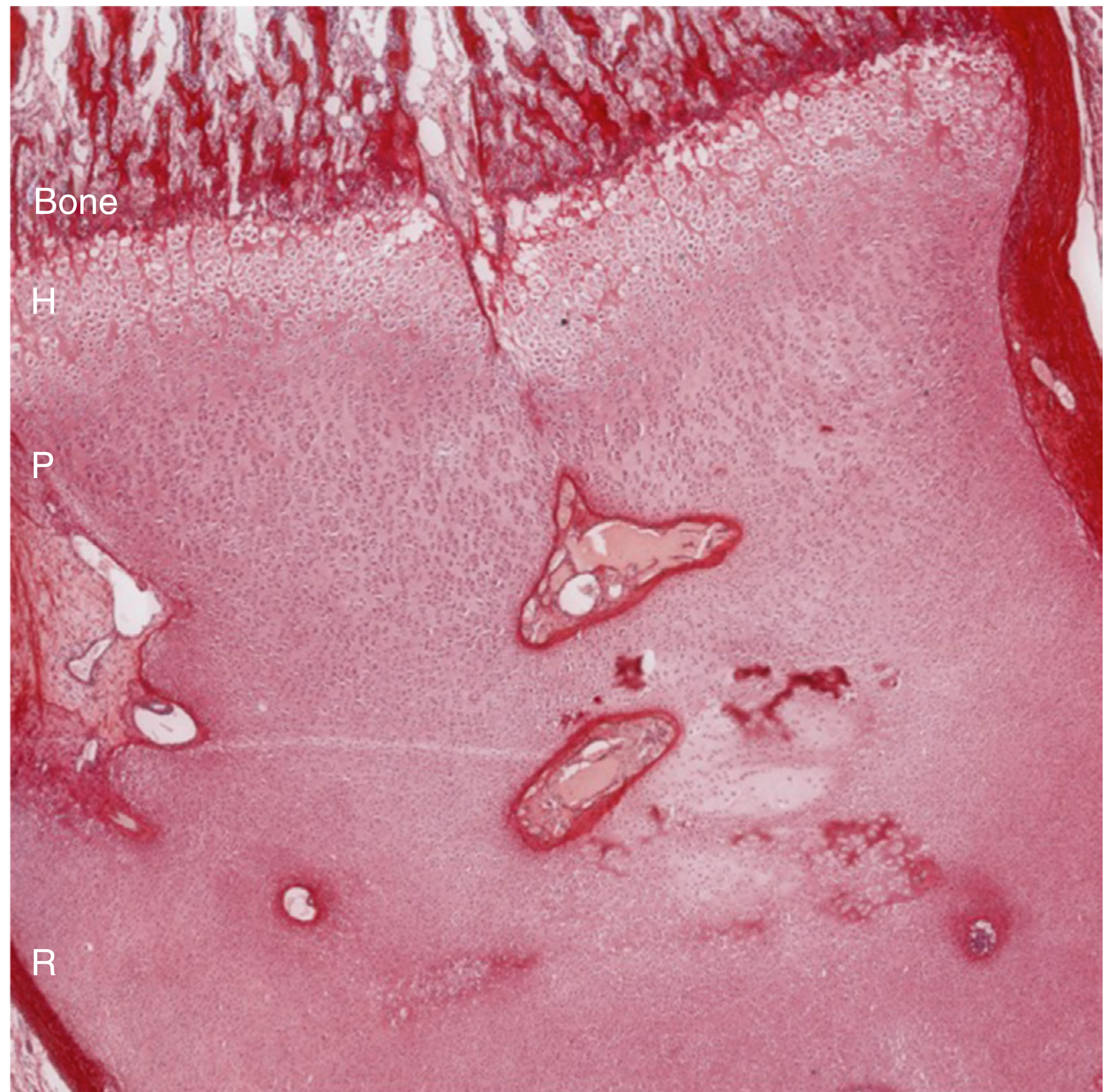
(Zones H = Hypertrophic, P = Proliferative, R = Resting - Firestein & Kelley's Rheumatology)
2. FACTORS CAUSING GROWTH DISTURBANCE
A) Traumatic
- Salter-Harris (SH) types III, IV, V carry highest risk
- SH V (crush/compression) - worst, often missed acutely
- Bony physeal bar: peripheral bar → angular deformity; central bar → shortening
- Most physeal fractures run through the proliferative zone
B) Infection
- Neonatal haematogenous osteomyelitis: metaphyseal vessels cross physis in children <18 months
- Septic arthritis: proteolytic enzymes directly destroy cartilage
- Especially dangerous: hip (proximal femur physis)
C) Radiation
- Doses >2000 cGy cause chondrocyte death
- Growth arrest or angular deformity depending on field
D) Vascular/Ischaemic
- Perthes disease (AVN femoral head)
- Sickle cell disease: physeal infarction
- Disruption of perichondrial ring of LaCroix
E) Metabolic/Nutritional
- Rickets: widened, cupped, frayed physis; disorganised zones
- Scurvy: zone of provisional calcification primarily affected
- Hypothyroidism, growth hormone deficiency
F) Iatrogenic
- Hardware crossing physis (threaded pins most damaging)
- Principle: use smooth wires, smallest diameter, remove as soon as stable
G) Tumours/Dysplasia
- Multiple hereditary exostoses: osteochondromas tether physis
- Achondroplasia: FGFR3 mutation - reduced proliferative zone activity
3. PRINCIPLES OF GUIDED GROWTH MODULATION
Definition: Temporary, reversible, partial physeal tethering to correct angular deformity or limb length discrepancy in a skeletally immature patient.
Underlying Principle - Hueter-Volkmann Law:
- Increased compressive load → inhibits physeal growth
- Decreased compressive load → stimulates physeal growth
- Tethering the convex side slows growth there, allowing the concave side to "catch up"
Methods:
-
Stapling (Blount, 1949)
- Metallic staples across physis on convex side
- Disadvantages: can damage physis, staples may "walk out," less predictable
-
Tension Band Plate / 8-Plate (Metaizeau; popularised by Stevens)
- Plate spans physis with 2 screws (one epiphyseal, one metaphyseal)
- As limb grows, screws diverge in a tension-band effect
- Fully reversible - plate removed once deformity corrected
- Indications: genu valgum, genu varum, tibia vara, limb length discrepancy, knee flexion contracture
- Timing: condyle must be large enough for smallest screw (>16 mm)
-
Transphyseal Screw
- Single cannulated screw crossing physis
- Minimally invasive, simple technique
Timing of intervention:
- Predict using Moseley straight-line graph or Green-Anderson tables
- Correction rate approximately 1° per month at the knee
- Must have adequate growth remaining
Advantages over corrective osteotomy:
- Minimally invasive, often outpatient
- Reversible and adjustable
- Gradual correction (no acute deformity)
- Can be repeated if overcorrection occurs
Complications:
- Overcorrection/rebound deformity after plate removal
- Hardware failure or migration
- Physeal damage (rare with smooth implants)
- Loss of correction
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Histology: A Text and Atlas (Eroschenko/Ross 9e); Firestein & Kelley's Textbook of Rheumatology
This is a shared conversation. Sign in to Orris to start your own chat.