Percutaneous tracheostomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"percutaneous tracheostomy"[MeSH Terms] AND "intensive care"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content to provide a thorough answer. Let me compile it.
Percutaneous Tracheostomy (Percutaneous Dilatational Tracheostomy - PDT)
Overview
Percutaneous tracheostomy was first described over 50 years ago (Sheldon, 1957) but grew significantly in popularity after Ciaglia introduced the dilatational technique in 1985. It is now the most common method of providing an alternative airway in ICU patients. The commercial kits most widely used are based on the Ciaglia single-dilator technique.
Indications
- Prolonged mechanical ventilation (anticipated >7-14 days)
- Failed or difficult weaning from ventilator
- Airway protection (impaired swallowing, neurological dysfunction)
- Upper airway obstruction
- Pulmonary toilet - facilitating secretion clearance
- Reducing work of breathing (shorter tube, lower airway resistance)
Contraindications
Absolute
- Cellulitis or deep infection at the insertion site
- Operator inexperience
Relative (PDT-specific)
- Inability to palpate relevant tracheal anatomy (short/obese neck)
- Overlying vessels (high-riding innominate artery, aberrant vasculature)
- Severe uncorrectable coagulopathy (ideally PT/PTT <1.5x control, platelets >50,000/mm³)
- Emergent airway situations
- PEEP >12 cm H2O (risk of derecruitment during procedure)
- Worsening acute critical illness (septic shock, severe ARDS)
- Children (rarely performed percutaneously)
Patients with coagulopathy from uremia can be treated with DDAVP before the procedure. Patients with difficult anatomy or significant coagulopathy should be referred for surgical tracheostomy.
Pre-procedure Assessment
- Review existing CT neck/chest: evaluate vascular anatomy (high-riding innominate artery, aberrant vessels)
- Ultrasound assessment of the neck - strongly recommended to identify vessels in the cannulation pathway
- Labs: platelet count, PT, PTT, BUN (to screen for uremia-related platelet dysfunction)
- Physical exam: palpate thyroid cartilage, cricoid cartilage, tracheal rings 1-3
- Ideal anatomy: easily palpable landmarks, no overlying vessels
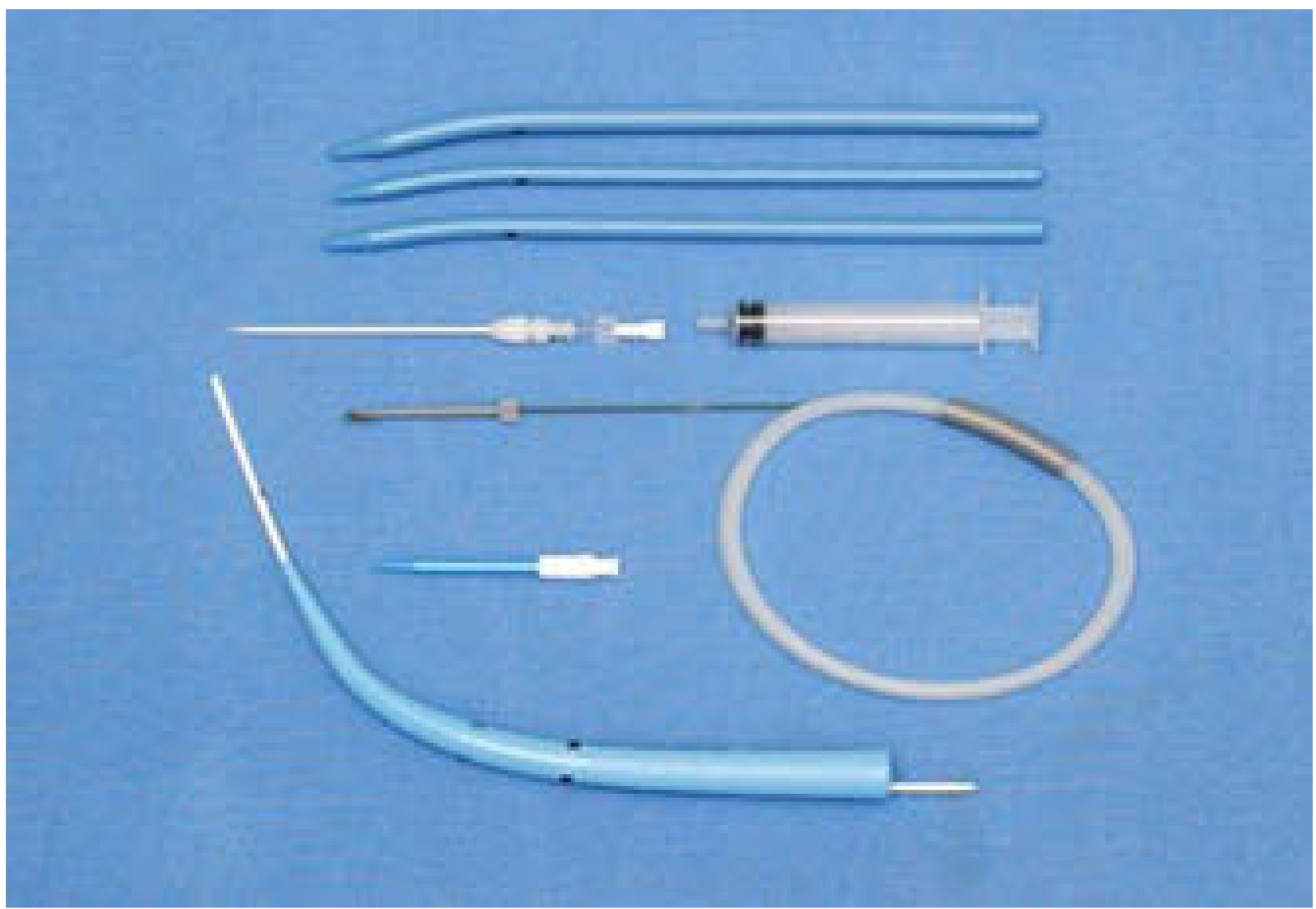
Equipment (Ciaglia Technique Kit)
- 14-gauge introducer needle + cannula
- Syringe (saline-filled for air confirmation)
- J-tipped guidewire
- Short 14-French initial dilating catheter
- Single tapered dilator (Ciaglia Blue Rhino)
- Tracheostomy tube loaded on obturator
- Flexible bronchoscope (strongly recommended)
Technique (Ciaglia Single-Dilator - Step by Step)
Setup
- Patient supine with shoulder roll to extend neck and improve landmark access
- Head of bed slightly elevated (reverse Trendelenburg) to reduce cervical venous pressure
- Increase FiO₂ to 1.0; adjust ventilator mode to ensure adequate minute ventilation
- Sedate, analgesic, and short-acting paralysis - minimize coughing and patient movement
- Optimal staffing: anesthesiologist at head of bed to manage ETT + bronchoscopy + medications; trained nurse for monitoring and assistance
Incision and Access
- Identify landmarks: thyroid cartilage → cricoid → tracheal rings 1-3
- Infiltrate skin and subcutaneous tissue with 1% lidocaine + epinephrine (up to 10cc) - primarily for vasoconstriction
- Make a 1-1.5 cm horizontal (or vertical) incision through skin and subcutaneous fascia
- Bluntly dissect soft tissue until tracheal rings are palpable
Bronchoscopic Guidance
- Position bronchoscope at the distal end of the ETT
- Withdraw scope proximally and use transillumination through the neck incision to estimate how far to retract the ETT
- Deflate ETT cuff and retract ETT until the bronchoscopist can visualize the intended entry site
Needle and Wire Insertion
- Insert 14-gauge needle into the trachea under direct bronchoscopic visualization, aiming for midline, avoiding the posterior membrane
- Target: between the 1st-2nd or 2nd-3rd tracheal rings (above the 3rd ring reduces stenosis risk; below 3rd ring increases tracheo-innominate fistula risk)
- Confirm position: aspiration of air + direct bronchoscopic visualization
- Remove syringe; advance J-tipped guidewire toward the carina
Dilation and Tube Placement
- Dilate tract with the short 14-French dilating catheter first
- Pass single tapered dilator over the guidewire (Seldinger technique)
- Load tracheostomy tube over its obturator and advance over the guidewire into the trachea
- Inflate tracheostomy tube cuff once confirmed in tracheal lumen
- Verify position via bronchoscopy through the ETT
- Then remove ETT; secure tracheostomy tube
Timing of Tracheostomy
This remains controversial and individualized. Key data points:
| Timing | Definition | Evidence |
|---|---|---|
| Early | Within 4-7 days (some trials: 48-96h) | No mortality benefit shown in RCTs |
| Late | >10-21 days | >50% of patients randomized to late tracheostomy never needed the procedure |
A multicenter RCT of 1,032 patients (57 sites) comparing early (≤4 days) vs. late (>10 days) tracheostomy found no difference in 30-day or 2-year mortality, duration of mechanical ventilation, antibiotic use, or sedative use. Multiple meta-analyses confirm no mortality benefit from early tracheostomy, though early tracheostomy may reduce ventilator-associated pneumonia (VAP). Timing remains a case-by-case clinical decision.
Complications
Perioperative (Intraoperative / Early)
| Complication | Notes |
|---|---|
| Hemorrhage | Most common; ligation/cautery not available in PDT unlike surgical |
| Hypoxia / desaturation | From ETT manipulation; increase FiO₂ pre-procedure |
| Posterior tracheal wall injury | Higher rate in PDT vs. surgical (50 vs. 6 per 10,000) |
| Pneumothorax / pneumomediastinum | Higher rate in PDT vs. surgical tracheostomy |
| False passage | Guidewire/dilator exits trachea |
| Accidental decannulation | Tube displacement before tract matures |
| Cardiorespiratory arrest | Rare; higher in PDT than surgical in some meta-analyses |
Late Complications
| Complication | Notes |
|---|---|
| Tracheo-innominate artery fistula (TIF) | <1% incidence; mortality ~85%; peak at 7-14 days post-op |
| Tracheal stenosis | Risk increases if cricothyroid membrane involved; tube below 3rd ring |
| Tracheomalacia | Chronic pressure necrosis |
| Tracheoesophageal fistula | Rare |
| Stomal infection | Higher in surgical than PDT per some meta-analyses |
| Granulation tissue | Common at stoma site |
Managing Tracheo-Innominate Fistula (TIF) - Emergency Protocol
- Do NOT deflate the tracheostomy cuff
- If stable: CT neck with contrast to assess fistula
- Take to OR for immediate repair
- If actively hemorrhaging: replace tracheostomy with ETT through vocal cords (cuff distal to bleeding); apply digital anterior pressure through the stoma; OR immediately
PDT vs. Surgical Tracheostomy - Comparison
| Feature | PDT | Surgical Tracheostomy |
|---|---|---|
| Setting | Bedside ICU | OR (or bedside with full equipment) |
| Speed | Faster; no OR scheduling | Slower (OR time required) |
| Cost | Lower | Higher |
| Hemorrhage & infection | Lower in most meta-analyses | Higher in most meta-analyses |
| Perioperative serious complications | Slightly higher (pneumothorax, posterior wall injury) | Slightly lower |
| Late complications (stenosis, TEF) | Similar | Similar |
| Coagulopathy management | Limited (no cautery) | Better (cautery available) |
| Difficult anatomy | Refer to surgical | Preferred |
A meta-analysis of 17 RCTs (n=1,212) showed PDT was associated with fewer infections and less bleeding vs. surgical tracheostomy. However, an earlier meta-analysis of 65 trials showed serious perioperative complications (cardiorespiratory arrest, pneumothorax, posterior wall injury) were more common with PDT (149 vs. 86 per 10,000). Late complication rates were similar between the two approaches.
Post-Procedure Care
- Monitor cuff pressure: keep <25 mmHg to prevent ischemic mucosal injury and avoid tracheal stenosis
- Initial tube: cuffed (to protect from secretions and bleeding)
- After 3-4 days: can change to uncuffed tube if no longer on ventilator
- Secure tube with ties (neck slightly flexed when tying - avoids slack when neck moves)
- Or suture flanges directly to skin
- Once ventilation no longer required: consider downsizing and decannulation, change to uncuffed tube
Sources:
- Current Surgical Therapy, 14e, Tracheostomy chapter
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Ch. 72
- Bailey and Love's Short Practice of Surgery, 28e, Ch. 52
- Cummings Otolaryngology Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.