Pericarditis (dry pericarditis and pericardial effusion).
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pericarditis"[MeSH Terms] AND "pericardial effusion"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
pericarditis ECG saddle-shaped ST elevation
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Let me compile the complete, well-organized response.
Pericarditis: Dry Pericarditis and Pericardial Effusion
1. Anatomy of the Pericardium
The pericardium consists of two serous layers — the visceral pericardium (continuous with the epicardial surface) and the parietal pericardium (a dense fibrous structure), enclosing a potential space that normally contains 5–35 mL of ultrafiltrate. Functions include: fixing the heart's position, lubricating its surface, preventing overdistension, limiting spread of infection, and mediating ventricular interdependence during diastolic filling. Notably, congenital absence of the pericardium causes few if any functional problems. — Textbook of Clinical Echocardiography; ROSEN's Emergency Medicine
2. Etiology
Pericarditis is inflammation of the pericardium caused by granulocytic and lymphocytic infiltration. It accounts for ~5% of non-ischemic chest pain presentations to the ED. — ROSEN's Emergency Medicine
| Category | Examples |
|---|---|
| Infectious | Viral (most common in developed countries), bacterial, fungal, parasitic, TB (common in developing countries) |
| Post-injury | Blunt/penetrating trauma, post-cardiac surgery, radiation, post-MI (Dressler syndrome), medications |
| Systemic diseases | SLE, rheumatoid arthritis, systemic sclerosis, sarcoidosis, amyloidosis, rheumatic fever |
| Metabolic | Uremia (most common systemic cause), hypothyroidism |
| Neoplastic | Metastatic (lung, breast, lymphoma, melanoma) or primary cardiac tumors |
| Idiopathic | 80–90% of cases in Western countries are labeled idiopathic (presumed viral) |
— ROSEN's Emergency Medicine, Box 68.3; Robbins & Kumar Basic Pathology
3. Dry (Fibrinous) Pericarditis
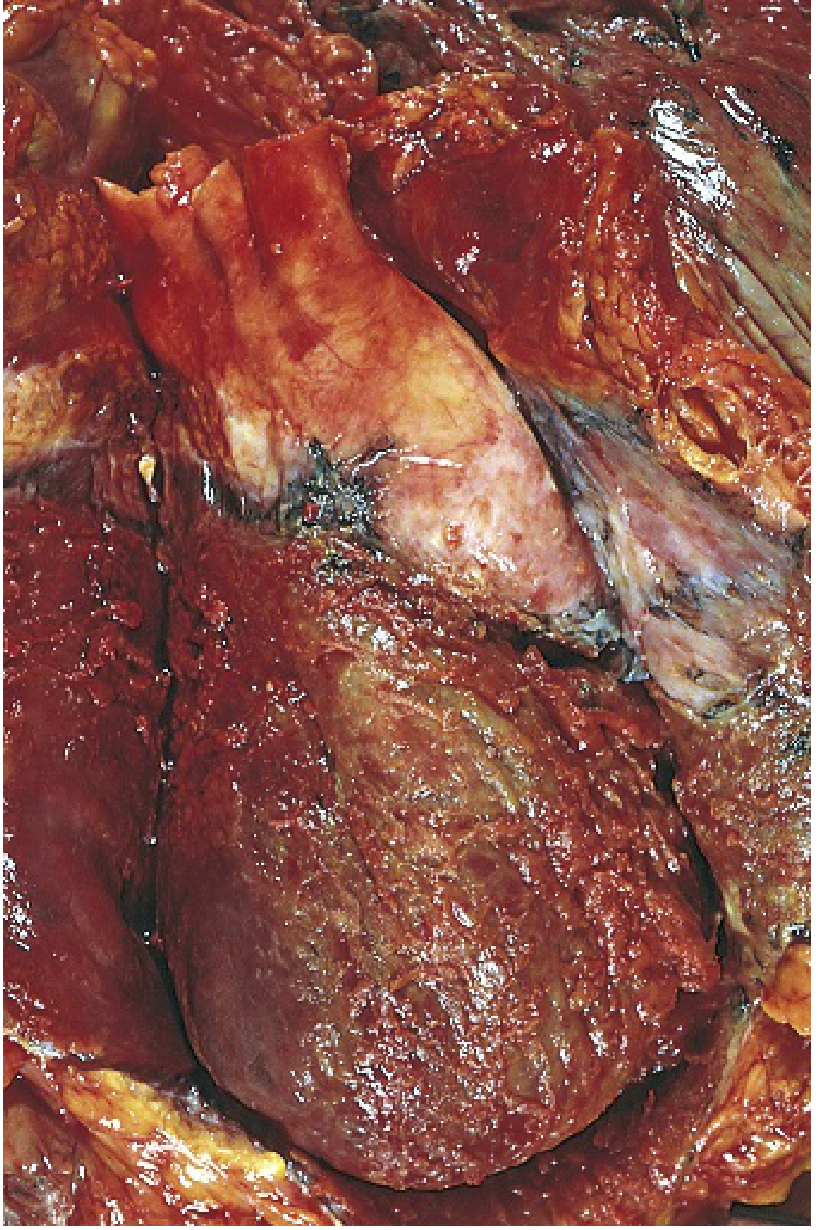
Pathology
In viral/idiopathic pericarditis or uremia, the exudate is fibrinous, imparting a shaggy, bread-and-butter appearance to the pericardial surface. Bacterial pericarditis produces fibrinopurulent (suppurative) exudate with areas of pus. Tuberculous pericarditis shows caseous necrosis. Malignant pericarditis is associated with a shaggy fibrinous exudate, often with a hemorrhagic effusion. — Robbins & Kumar Basic Pathology
Clinical Features
- Chest pain: Sharp, pleuritic, retrosternal; can radiate to the trapezius ridge, neck, shoulder, or arms. Relieved by sitting forward, worsened by lying flat, deep inspiration, or swallowing. — ROSEN's EM
- Pericardial friction rub: The hallmark sign. A "scratchy," leathery sound classically with three components (atrial systole, ventricular systole, ventricular diastole — the "to-and-fro" rub). Best heard at the lower left sternal border with the diaphragm, patient leaning forward in full expiration. Tends to be intermittent and migratory. — ROSEN's EM
- Fever and myalgias are common.
- Dyspnea, cough, hiccups, dysphagia may also be present.
Diagnostic Criteria
Diagnosis requires at least 2 of 4 criteria: — Textbook of Family Medicine
- Characteristic chest pain
- Pericardial friction rub
- Characteristic ECG changes
- New or worsening pericardial effusion
ECG Changes — The Four Stages
The ECG is the most reliable diagnostic tool and evolves in four stages over time:
| Stage | Timing | ECG Findings |
|---|---|---|
| Stage 1 | Hours to days | Diffuse concave-upward (saddle-shaped) ST elevation in multiple leads; PR segment depression (most prominent in II and V4–V6); reciprocal ST depression and PR elevation in aVR; Spodick's sign (downward slope of TP segment) |
| Stage 2 | Days | ST and PR normalize; T waves begin to flatten |
| Stage 3 | Weeks | Deep, symmetric T-wave inversions (without Q waves); normal ST segments |
| Stage 4 | Weeks–months | Full normalization (T-wave inversions may persist) |
Key ECG differences from STEMI: ST elevation is diffuse (not localized to one coronary territory), concave upward (not convex), T-wave inversions are not simultaneous with ST elevation, no Q waves develop, and PR depression is a unique feature. — ROSEN's EM

Laboratory Findings
- ESR and CRP elevated (CRP useful for monitoring disease activity and guiding duration of therapy)
- Leukocytosis
- Troponin may be elevated if concurrent myopericarditis (myocardial involvement)
- Other labs directed at non-idiopathic causes (ANA, RF, BUN/creatinine, cultures, TSH)
- Serology (antiviral titers) has low yield and does not alter management
4. Pericardial Effusion
Definition and Causes
An abnormal accumulation of fluid in the pericardial space, either transudative or exudative. Common causes include: — Grainger & Allison's Diagnostic Radiology; ROSEN's EM
| Mechanism | Causes |
|---|---|
| Transudative | Heart failure, uraemia, post-cardiac surgery, radiation, myxoedema, post-pericardiectomy syndrome, collagen-vascular diseases |
| Exudative | Viral/idiopathic pericarditis, bacterial/TB infection, malignancy |
| Haemopericardium | Trauma, aortic dissection, aortic rupture, neoplasm |
Clinical Features
- Often asymptomatic, especially if accumulation is slow
- Symptoms (cough, fever, chest pain, dyspnea) may reflect the underlying pericarditis
- Large or rapidly accumulating effusions → risk of cardiac tamponade
Imaging
Chest X-Ray:
- Requires ≥200–250 mL of fluid to produce cardiomegaly on CXR
- Water-bottle (flask) sign: globular enlargement of the cardiac silhouette with a broad base
- Effacement of normal cardiac borders; bilateral hilar overlay
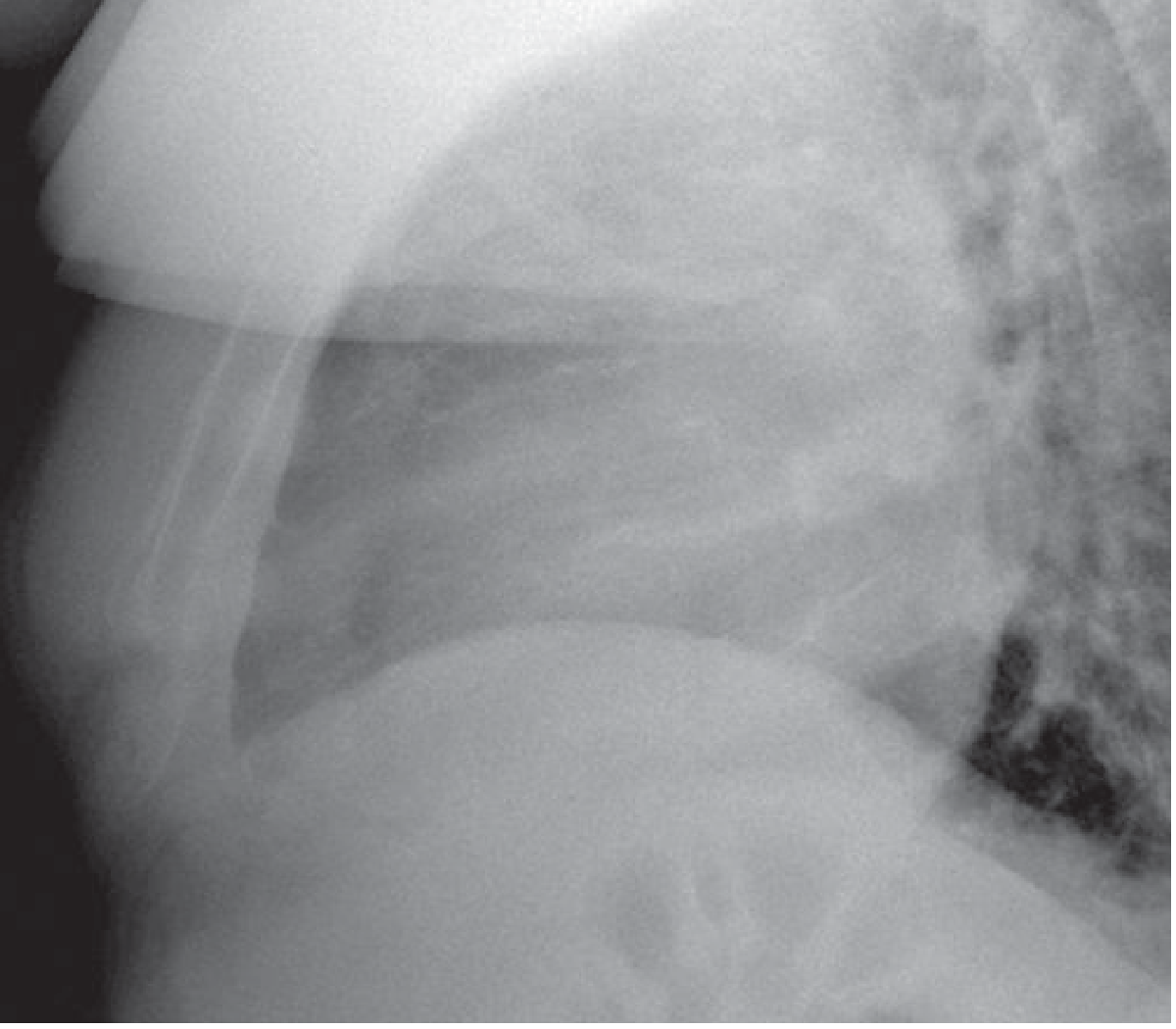
- Epicardial fat pad sign on lateral view: a pericardial stripe >2 mm between epicardial and mediastinal fat bands
- "Sandwich sign": on lateral CXR, a wide band of higher density in the retrosternal space flanked by two bands of lower density (fat)
- Interval enlargement of cardiac silhouette on serial films should raise strong suspicion — Grainger & Allison; Goldman-Cecil Medicine
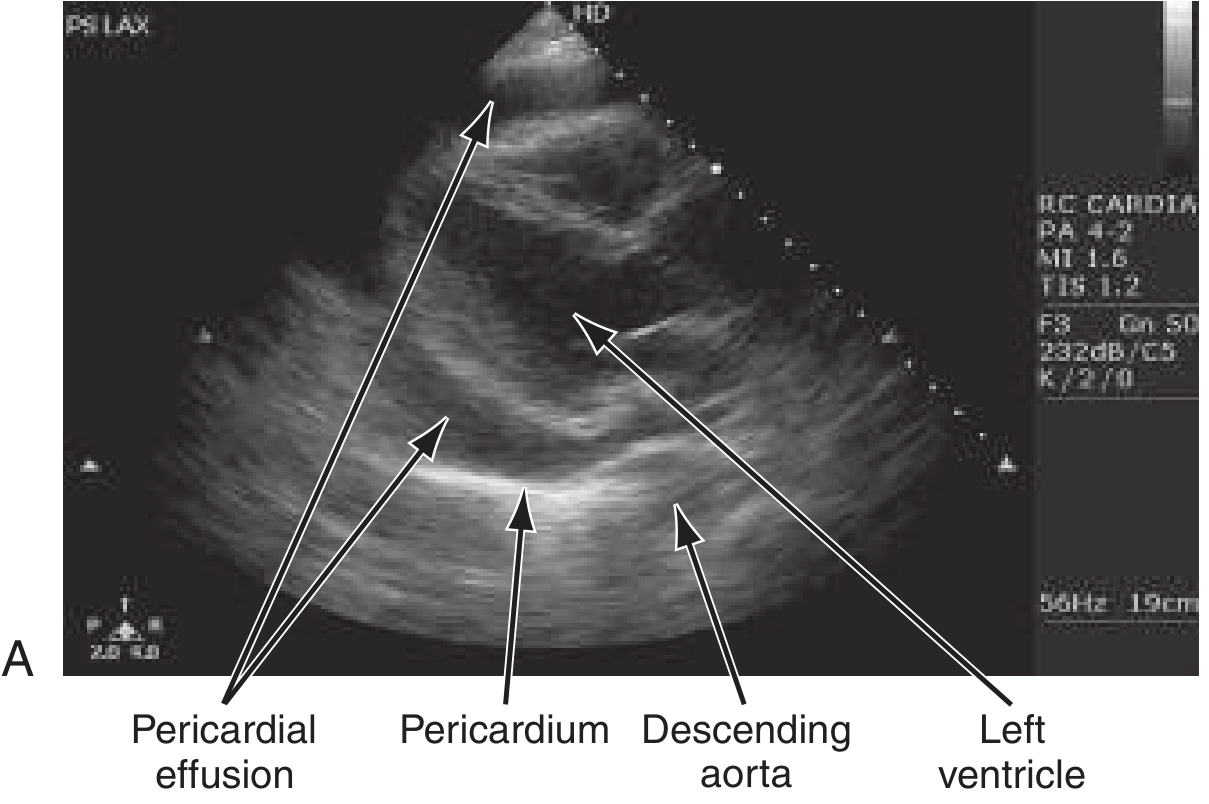
Echocardiography (Echo/POCUS):
- Highly sensitive and specific; first-line imaging
- Echo-free (anechoic) space between the pericardium and the epicardium
- Up to 60% of pericarditis patients have a detectable effusion on echo
- Distinguishes pericardial fluid from pleural fluid and from cardiac chamber dilation
- A normal echo does not exclude pericarditis
CT/MRI:
- Useful when echo is technically limited (obese/emphysematous patients)
- MRI with gadolinium: pericardial delayed hyperenhancement indicates active inflammation
- CT delineates the extent of effusion and underlying causes
Sizing and Hemodynamic Impact
| Size | Volume (approx.) | Risk |
|---|---|---|
| Small | <100 mL | Typically asymptomatic; seen on echo |
| Moderate | 100–500 mL | May be symptomatic depending on rate |
| Large | >500 mL | High tamponade risk, especially if rapidly accumulating |
The rate of accumulation matters more than volume: a slowly developing effusion of 2 L may be tolerated, while a rapidly developing 200 mL can cause tamponade due to the pericardium's limited compliance.
5. Cardiac Tamponade
When pericardial fluid accumulates faster than the pericardium can stretch, intrapericardial pressure rises and compresses the cardiac chambers, reducing diastolic filling and cardiac output.
Pathophysiology
- Equalization of pressures: right atrial pressure = left atrial pressure = PCWP = pericardial pressure
- Blunted or absent y descent on right atrial tracing (impaired early diastolic filling)
- Ventricular interdependence exaggerated: RV filling during inspiration reduces LV filling
Clinical Features — Beck's Triad (classic)
- Hypotension (falling cardiac output)
- Raised JVP (right-sided venous distension)
- Muffled heart sounds
Additional findings:
- Tachycardia (first compensatory mechanism)
- Pulsus paradoxus (>10 mmHg drop in systolic BP on inspiration) — key sign
- Kussmaul's sign is absent in tamponade (present in constriction)
- ECG: electrical alternans (alternating QRS amplitude — heart swinging in fluid) + sinus tachycardia + low voltage
Echo in Tamponade (key findings):
- Right atrial systolic collapse (most sensitive)
- Right ventricular diastolic collapse (more specific for hemodynamic compromise)
- Reciprocal respiratory variation in ventricular volumes (RV expands on inspiration while LV contracts)
- IVC dilation with absent respiratory collapse
- Respiratory variation in mitral/tricuspid Doppler flows >25–40% — Textbook of Clinical Echocardiography
Treatment
- Urgent pericardiocentesis (echo-guided preferred) — both diagnostic and therapeutic
- Avoid vasodilators and diuretics (they reduce preload); give IV fluids as a bridge
- Inotropes may be required
- Surgical drainage (pericardial window) for recurrent or loculated effusions
6. Management of Acute Pericarditis
First-Line (Non-specific / Idiopathic)
| Drug | Dose | Duration |
|---|---|---|
| Aspirin | 650 mg TID (preferred first-line) | ~3 weeks |
| Ibuprofen | 600 mg QID | 10–14 days |
| Indomethacin | 25 mg TID | 10–14 days |
| Naproxen | 250 mg BID | 7 days (if other NSAID fails) |
- Add a proton pump inhibitor (gastroprotection)
- Colchicine (0.5–1 mg/day for 4–6 weeks): recommended as adjunct; reduces recurrence rate; avoid in severe hepatic/renal impairment
Second-Line
- Corticosteroids: avoided unless all other treatments have failed — associated with higher relapse rates. Acceptable as first-line only in autoimmune disease (SLE) or uremic pericarditis where NSAIDs are contraindicated. — Textbook of Family Medicine
Surgical
- Pericardiectomy: reserved for recurrent pericarditis unresponsive to aggressive medical therapy. May not always eliminate symptoms. — Textbook of Family Medicine
Activity Restriction
- Athletes and physically active patients: restrict strenuous activity until symptom resolution and normalization of CRP/ECG/echo
Indications for Hospitalization
- First episode (for observation)
- Large effusion or tamponade
- High-risk features: fever >38°C, subacute onset, immunosuppression, anticoagulation use, elevated troponin (suggesting myopericarditis), failure of NSAIDs
7. Outcomes and Complications
| Outcome | Notes |
|---|---|
| Resolution without sequelae | Most common in viral/idiopathic pericarditis |
| Recurrent pericarditis | ~15–30% of cases; colchicine significantly reduces recurrence |
| Cardiac tamponade | More common with bacterial, malignant, or trauma-related effusions |
| Constrictive pericarditis | Fibrotic end-stage; dense pericardial scarring prevents diastolic filling; mimics restrictive cardiomyopathy |
| Effusive-constrictive pericarditis | Mixed picture; late complication especially after chest irradiation |
Constrictive pericarditis produces a combination of right-sided venous distension and low cardiac output. The pericardial space is obliterated by dense fibrosis such that the heart cannot expand during diastole. — Robbins & Kumar Basic Pathology
Predictors of poor outcome (multivariable analysis): female sex, large effusion or tamponade, failure of aspirin/NSAIDs. — Textbook of Family Medicine
8. Special Contexts
- Autoimmune diseases: Pericarditis affects 40–80% of SLE patients (necropsy studies) and 40% of RA patients; usually associated with disease flare. Cardiac tamponade is rare in SLE (1–2%). In SSc, small effusions are common but rarely hemodynamically significant. — Braunwald's Heart Disease
- Dressler syndrome: Post-MI autoimmune pericarditis (develops weeks after MI) due to antibodies against injured myocardium; presents with fever, chest pain, and pleuritis
- Purulent pericarditis: Life-threatening; Streptococcus and Staphylococcus most common; requires pericardiocentesis for diagnosis and drainage; treatment is pericardiectomy or indwelling catheter + fibrinolytics + IV antibiotics — ROSEN's EM
- Malignant effusion: ~40% of cancer patients with pericardial effusion actually have radiation-induced or idiopathic pericarditis, not malignant involvement — Braunwald's Heart Disease
Sources: Robbins & Kumar Basic Pathology; Braunwald's Heart Disease (11e); ROSEN's Emergency Medicine; Textbook of Family Medicine (9e); Textbook of Clinical Echocardiography; Grainger & Allison's Diagnostic Radiology; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.