Uncle herniation and tentorium cerebelli
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Excellent - I have rich content and two clear diagrams. Let me now compile the comprehensive answer.
Uncal Herniation and the Tentorium Cerebelli
The Tentorium Cerebelli - Anatomy
The tentorium cerebelli is a rigid dural fold that separates the supratentorial compartment (cerebral hemispheres) from the infratentorial compartment (brainstem + cerebellum/posterior fossa). It is less flexible than the falx cerebri because its fibrous dural lamina is stretched across the surface of the middle fossa and tethered for about three-quarters of its extent:
- Anteriorly: attaches to the petrous ridges and posterior clinoid processes
- Laterally: attaches to the occipital bone along the lateral sinus
- Centrally: has a large semioval opening called the tentorial notch (incisura), measuring ~25-40 mm mediolaterally and 50-70 mm rostrocaudally
The tentorial notch is the critical passage through which herniation occurs. The midbrain, CN III, posterior cerebral arteries, and the ascending arousal system (reticular formation) all pass through or adjacent to this notch.
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Herniation Syndromes Overview
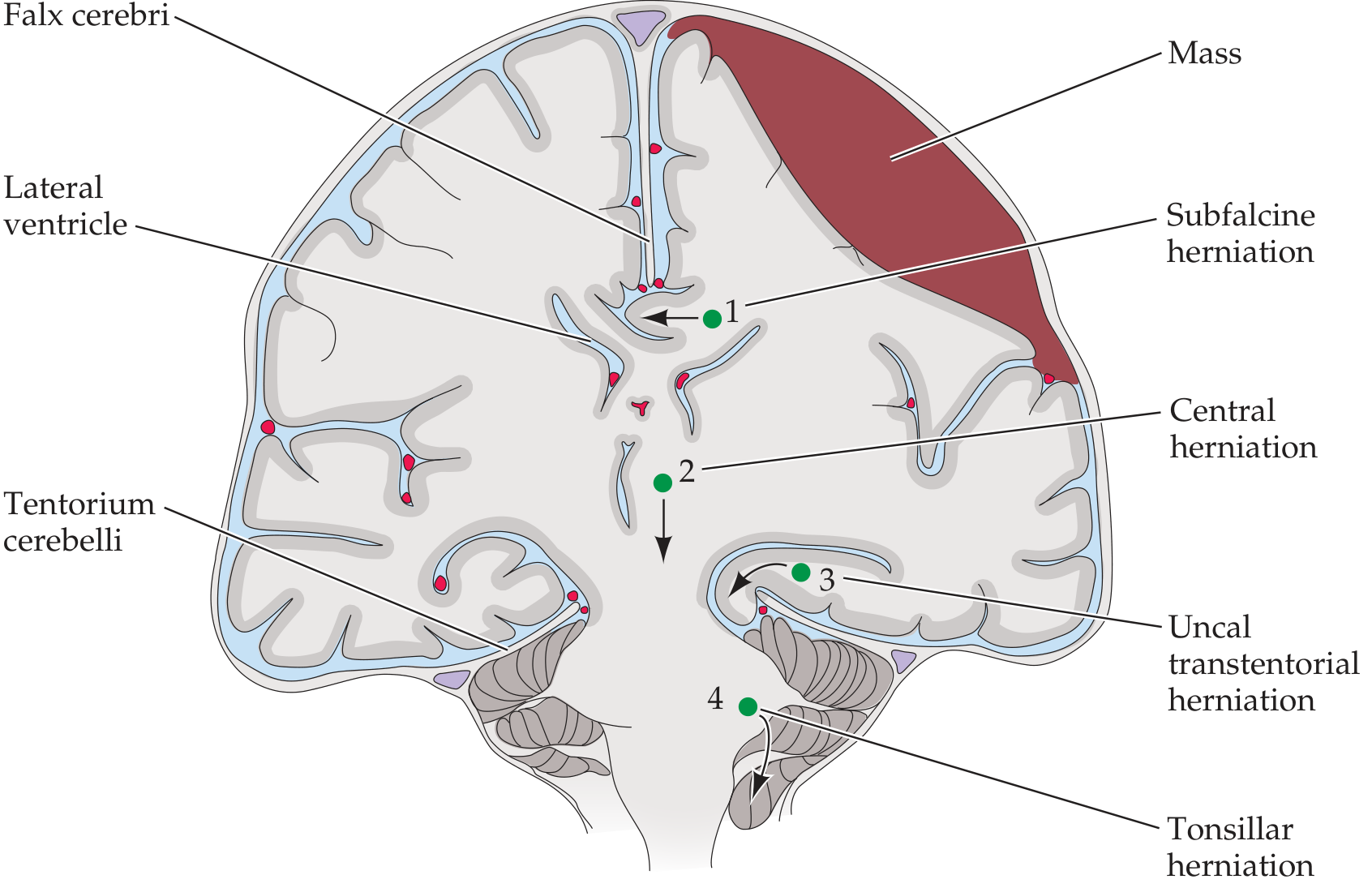
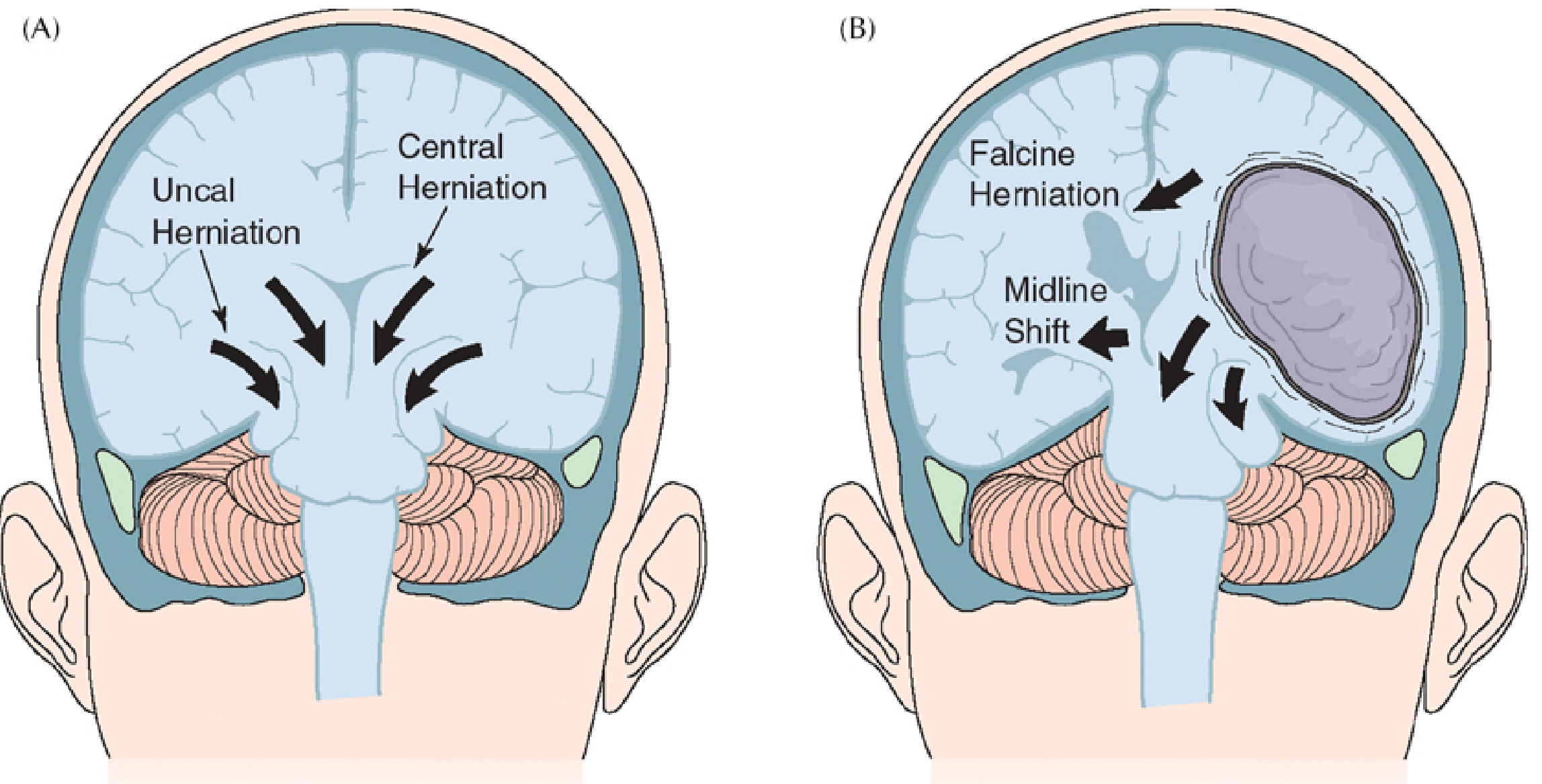
Uncal Herniation - Mechanism
Uncal herniation (also called transtentorial or uncal transtentorial herniation) is the most common type of brain herniation. It occurs when a laterally expanding supratentorial mass lesion (e.g., epidural/subdural hematoma, intracerebral hemorrhage, large infarct with edema, tumor) forces the medial edge of the temporal lobe - especially the uncus - to herniate medially and downward over the free tentorial edge into the tentorial notch.
This is distinct from central herniation, in which symmetric downward displacement of the diencephalon and brainstem occurs due to bilateral/diffuse increased ICP.
- Neuroanatomy through Clinical Cases, 3rd Ed.
- Goldman-Cecil Medicine
Structures Compressed and Their Clinical Effects
1. Oculomotor Nerve (CN III)
- The CN III runs along the dorsal surface of the uncus as it exits the midbrain. Uncal herniation compresses the parasympathetic fibers on the outer surface of CN III first (these fibers are on the periphery of the nerve).
- Result: ipsilateral fixed, dilated pupil ("blown pupil") - the classic early sign
- In 85% of cases, the blown pupil is ipsilateral to the lesion
- Later: complete CN III palsy with ptosis, exotropia ("down-and-out" eye), and ophthalmoplegia
2. Cerebral Peduncle (Corticospinal Tract)
- Compression of the ipsilateral cerebral peduncle by the herniating uncus causes contralateral hemiplegia (corticospinal fibers cross at the pyramidal decussation in the medulla)
- However, if the midbrain is pushed far enough that the contralateral peduncle is compressed against the opposite incisural edge, this causes ipsilateral hemiplegia - this is Kernohan's notch phenomenon (false localizing sign)
- The pupil is a more reliable lateralizing sign than hemiplegia (>90% accuracy)
3. Reticular Activating System (Midbrain)
- Distortion of the midbrain reticular formation disrupts the ascending arousal system
- Result: progressive impairment of consciousness - drowsiness → stupor → coma
- Pupillary dilation from uncal herniation with a preserved level of consciousness is rare
4. Posterior Cerebral Artery (PCA)
- The PCAs pass upward through the tentorial notch
- Compression causes PCA territory infarction - bilateral involvement produces cortical blindness
Classic Clinical Triad of Uncal Herniation
| Sign | Mechanism |
|---|---|
| "Blown" (fixed, dilated) pupil - ipsilateral | CN III parasympathetic compression |
| Contralateral hemiplegia (or ipsilateral in Kernohan's) | Cerebral peduncle compression |
| Progressive coma | Midbrain reticular formation distortion |
- Neuroanatomy through Clinical Cases, 3rd Ed.
Herniation Stages and Progression
Uncal herniation has a predictable rostrocaudal progression if untreated:
- Early uncal stage: ipsilateral pupillary dilation, sluggish pupil; patient may still be alert (rare to have preserved consciousness with full blown pupil)
- Late uncal / early midbrain stage: fully blown pupil, hemiplegia, declining consciousness
- Midbrain-upper pons stage: bilateral fixed midposition pupils (~5 mm), decorticate then decerebrate posturing
- Lower pons-upper medulla: pupils fixed, no doll's eye reflex, flaccidity
- Medullary stage: ataxic breathing, cardiovascular collapse, death
Comparison: Uncal vs. Central Herniation
| Feature | Uncal Herniation | Central Herniation |
|---|---|---|
| Cause | Lateral/asymmetric mass | Diffuse ICP elevation or bilateral mass |
| First sign | Ipsilateral blown pupil | Diencephalic dysfunction (small reactive pupils, Cheyne-Stokes breathing) |
| Lateralizing signs | Prominent and early | Symmetric and later |
| Consciousness | Impaired, but pupil change may precede it | Gradual decline |
Key Anatomical Points Summary
- The tentorium cerebelli is a rigid, largely inextensible dural partition - it cannot expand to accommodate herniation
- The tentorial notch (incisura) is the pathway for herniation; everything that runs through it (CN III, PCA, midbrain, RAS) is vulnerable
- The herniation groove left by uncus compressing CN III can be seen at autopsy as a groove on CN III
- Upward transtentorial herniation can also occur from large posterior fossa masses, pushing cerebellar tissue upward through the notch
Sources:
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma
- Neuroanatomy through Clinical Cases, 3rd Edition
- Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.