Define immunity. What are different types of immunity? Explain in detail about the complement system and add a note on AIDS for 10 marks.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have all the information needed to write a comprehensive, well-structured 10-mark answer. Let me compile it:
Immunity, Types of Immunity, Complement System, and AIDS
1. Definition of Immunity
Immunity is defined as protection from infectious pathogens. In its broader sense, immunity includes host reactions against cancers (tumor immunity), tissue transplants, and even self antigens (autoimmunity). The immune system is vital for survival because it protects us from infectious pathogens that abound in the environment and from the development of cancer.
Robbins, Cotran & Kumar Pathologic Basis of Disease
2. Types of Immunity
The mechanisms of immunity fall into two broad categories:
A. Innate Immunity (Natural / Native Immunity)
Innate immunity refers to intrinsic mechanisms that are poised to react immediately, constituting the first line of defense. It is mediated by cells and molecules that recognize products of microbes and dead cells and induce rapid protective host reactions. It responds within hours of encountering a pathogen.
Components of Innate Immunity:
| Component | Role |
|---|---|
| Epithelial barriers (skin, GI, respiratory tracts) | Block entry of microbes; produce antimicrobial molecules (defensins) |
| Phagocytes (neutrophils, macrophages) | Sense, ingest, and destroy invaders |
| Dendritic cells | Capture antigens; serve as sentinels that detect danger |
| Natural killer (NK) cells | Provide early protection against viruses and intracellular bacteria |
| Innate lymphoid cells (ILCs) | Activated by cytokines; produce inflammatory cytokines in early responses |
| Plasma proteins (complement, MBL, CRP) | Opsonization, complement activation, killing of extracellular microbes |
Pattern Recognition: Innate immune cells recognize pathogen-associated molecular patterns (PAMPs) on microbes and damage-associated molecular patterns (DAMPs) from injured cells via pattern recognition receptors (PRRs) such as Toll-like receptors (TLRs).
B. Adaptive Immunity (Acquired / Specific Immunity)
Adaptive immunity consists of mechanisms that are stimulated by exposure to microbes and foreign substances ("adapt to"). It develops more slowly than innate immunity but is more powerful in combating infections. The adaptive immune response has two arms:
| Arm | Cells | Mechanism |
|---|---|---|
| Cell-mediated (Cellular) | T lymphocytes (CD4+ helper, CD8+ cytotoxic) | Kill intracellular microbes and infected cells |
| Humoral | B lymphocytes -> Plasma cells | Produce antibodies that neutralize and opsonize extracellular pathogens |
Key features of Adaptive Immunity:
- Specificity - targets a precise antigen
- Memory - rapid and stronger response upon re-exposure
- Self-limitation - response winds down after antigen is cleared
- Self-tolerance - does not attack the host's own tissues
The diagram below shows the principal components and timing of innate vs. adaptive immunity:
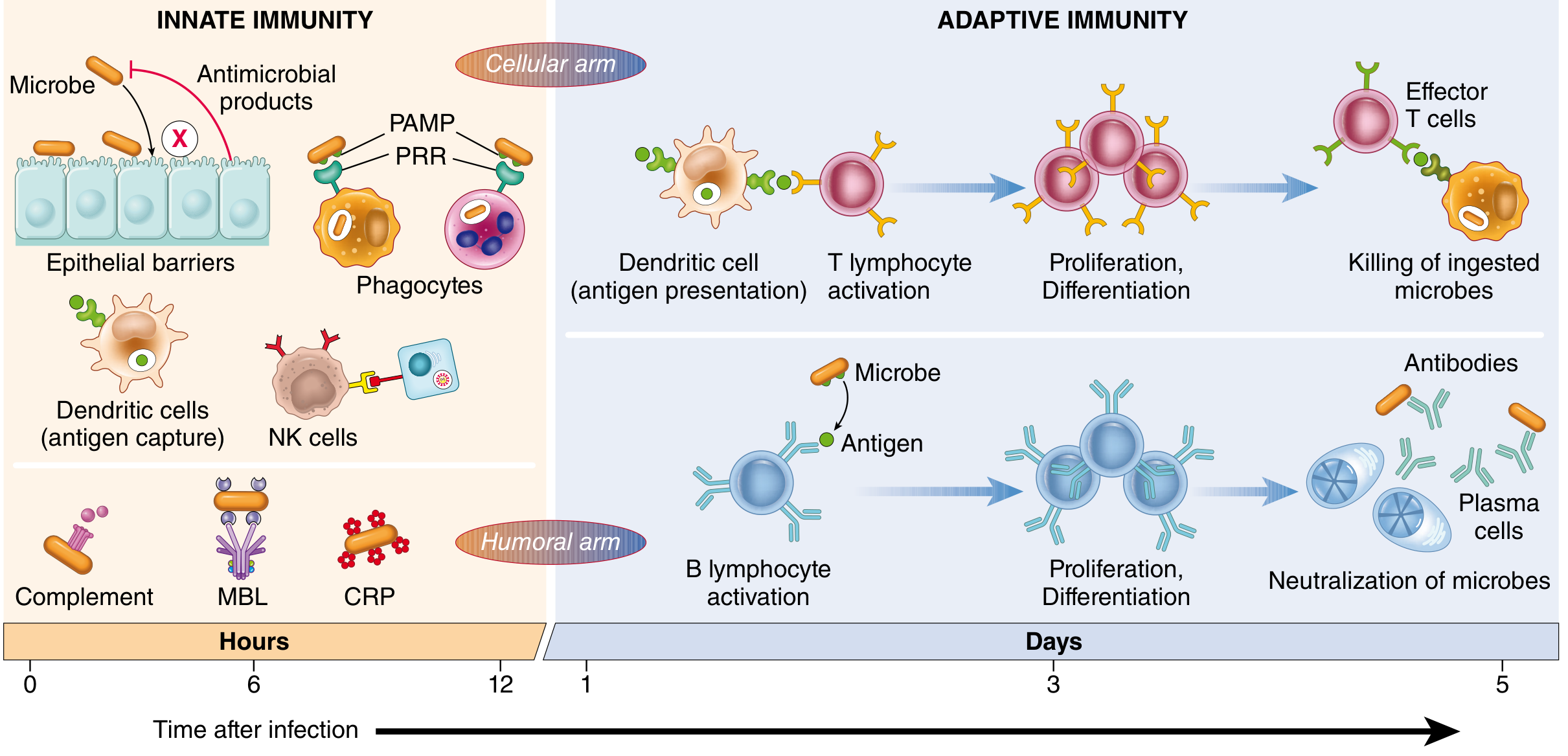
Fig. 6.1 - Innate immunity acts within hours; adaptive immunity develops over days. Both have cellular and humoral arms. (Robbins, Cotran & Kumar)
C. Other Classifications
Immunity can also be classified as:
- Active immunity - generated by the individual's own immune response (natural infection or vaccination); long-lasting
- Passive immunity - conferred by transfer of antibodies (e.g., maternal IgG across placenta, immunoglobulin therapy); immediate but short-lived
- Herd immunity - indirect protection of unimmunized individuals when a sufficient proportion of the population is immune
3. The Complement System
Definition
The complement system is a collection of plasma proteins (more than 20 proteins, some numbered C1 through C9) that function mainly in host defense against microbes and in pathologic inflammatory reactions. Complement proteins participate in both innate and adaptive immunity for defense against microbial pathogens.
The complement proteins are present in inactive (proforms) in plasma. They are activated during inflammatory reactions in a cascade of enzymatic reactions capable of tremendous amplification.
Activation Pathways
The critical step in complement activation is proteolytic cleavage of C3, the most abundant complement component. Cleavage of C3 can occur by one of three pathways:
1. Classical Pathway
- Trigger: Fixation of C1 to antibody (IgM or IgG) that has combined with antigen
- Leads to sequential binding of C2 and C4
- Culminates in formation of a multiprotein enzyme (C3 convertase) that cleaves C3
- This pathway links adaptive immunity (antibodies) to complement
2. Alternative Pathway
- Trigger: Microbial surface molecules such as endotoxin (LPS), complex polysaccharides, cobra venom - in the absence of antibody
- Spontaneous cleavage of C3 is amplified and stabilized on microbes
- This pathway operates as part of innate immunity
3. Lectin Pathway (Mannose-Binding Lectin Pathway)
- Trigger: Plasma mannose-binding lectin (MBL) binds to carbohydrates (mannose residues) on microbes
- Activates a protease homologous to C1; subsequent steps identical to the classical pathway
- Also functions in innate immunity (no antibody required)
Convergence: All three pathways lead to the formation of C3 convertase, which splits C3 into:
- C3a (released into plasma)
- C3b (covalently attached to the microbial surface)
C3b then binds previously generated fragments to form C5 convertase, which cleaves C5 into:
- C5a (released - potent inflammatory mediator)
- C5b (remains on cell surface)
C5b then binds late components (C6-C9) to form the Membrane Attack Complex (MAC).
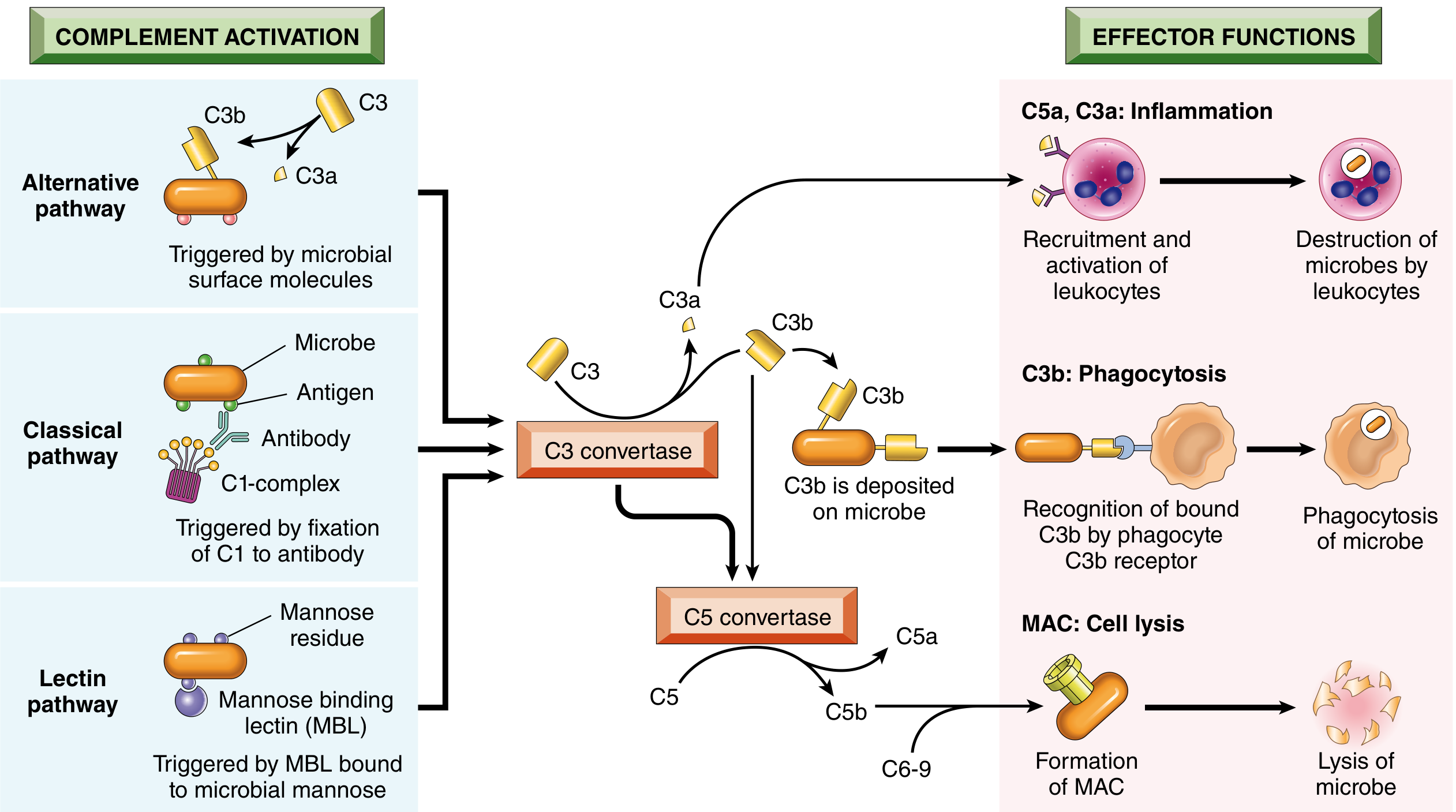
Fig. 3.11 - Activation and functions of the complement system. All three pathways converge on C3 convertase. (Robbins, Cotran & Kumar Pathologic Basis of Disease)
Functions of the Complement System
The complement system has three main functions:
1. Inflammation (Anaphylatoxins)
- C5a, C3a, and C4a are cleavage products that stimulate:
- Histamine release from mast cells -> increased vascular permeability and vasodilation
- Recruitment and chemotaxis of neutrophils, monocytes, eosinophils, and basophils (especially C5a)
- Activation of the lipoxygenase pathway in neutrophils -> further inflammatory mediators
- Called anaphylatoxins because they mimic mast cell mediators involved in anaphylaxis
2. Opsonization and Phagocytosis
- C3b and iC3b (inactive C3b), when fixed to a microbial cell wall, act as opsonins
- Neutrophils and macrophages bear cell surface receptors for these complement fragments (CR1, CR3)
- This promotes efficient phagocytosis of the coated microbes
3. Cell Lysis (Membrane Attack Complex - MAC)
- MAC is composed of C5b + C6 + C7 + C8 + multiple C9 molecules
- Deposition of MAC on cell membranes creates holes/pores in the membrane
- This allows intracellular water and ions to leak out -> osmotic lysis
- Particularly important for killing microbes with thin cell walls (e.g., Neisseria bacteria)
- Deficiency of terminal complement components (C5-C9) predisposes to Neisseria infections
Regulation of Complement
Complement activation is tightly controlled by regulatory proteins to prevent damage to healthy host cells:
| Regulator | Mechanism | Clinical Significance |
|---|---|---|
| C1 inhibitor (C1 INH) | Blocks activation of C1 (classical pathway) | Inherited deficiency causes hereditary angioedema |
| Decay-accelerating factor (DAF / CD55) | Prevents formation of C3 convertases (GPI-anchored) | Deficiency in PNH (paroxysmal nocturnal hemoglobinuria) |
| CD59 | Inhibits MAC formation (GPI-anchored) | Deficiency in PNH |
| Factor H | Inhibits alternative pathway by promoting C3b cleavage | Mutations cause atypical hemolytic uremic syndrome (aHUS); polymorphisms linked to age-related macular degeneration |
Paroxysmal nocturnal hemoglobinuria (PNH): An acquired deficiency of the enzyme that creates GPI anchors leads to deficiency of DAF and CD59 -> excessive complement activation -> lysis of red blood cells.
Complement in Disease
- In autoimmune diseases, antibodies against self antigens activate complement via the classical pathway -> tissue injury
- Inherited deficiencies of early complement proteins (C1, C4, C2) increase susceptibility to infections and SLE-like disorders
- Inhibitors of C5 (e.g., eculizumab) and C3 are now approved therapies for complement-mediated diseases like PNH and aHUS
4. Note on AIDS (Acquired Immunodeficiency Syndrome)
Etiology
AIDS is caused by the Human Immunodeficiency Virus (HIV), an RNA retrovirus that contains the enzyme reverse transcriptase. Two types exist: HIV-1 (responsible for most worldwide infections, multiple subtypes) and HIV-2 (less virulent, mainly West Africa). HIV-1 has an incubation period that may extend up to 11 years before clinical AIDS manifests.
Pathogenesis - How HIV Destroys Immunity
HIV gains entry primarily into CD4+ helper T cells by:
- gp120 (viral envelope glycoprotein) binds to CD4 molecules on helper T cells
- Interaction with co-receptors - mainly CCR5 (C-C chemokine receptor 5), and CXCR4
- gp41 anchors the virus into the T-cell membrane, allowing fusion
- Viral RNA (with reverse transcriptase) is injected into the T-cell cytoplasm
- Reverse transcriptase converts viral RNA into double-stranded DNA
- Viral DNA enters the nucleus and is integrated into the host genome (becoming a provirus) via integrase
- The provirus drives production of new viral particles, which bud out and infect more CD4+ T cells
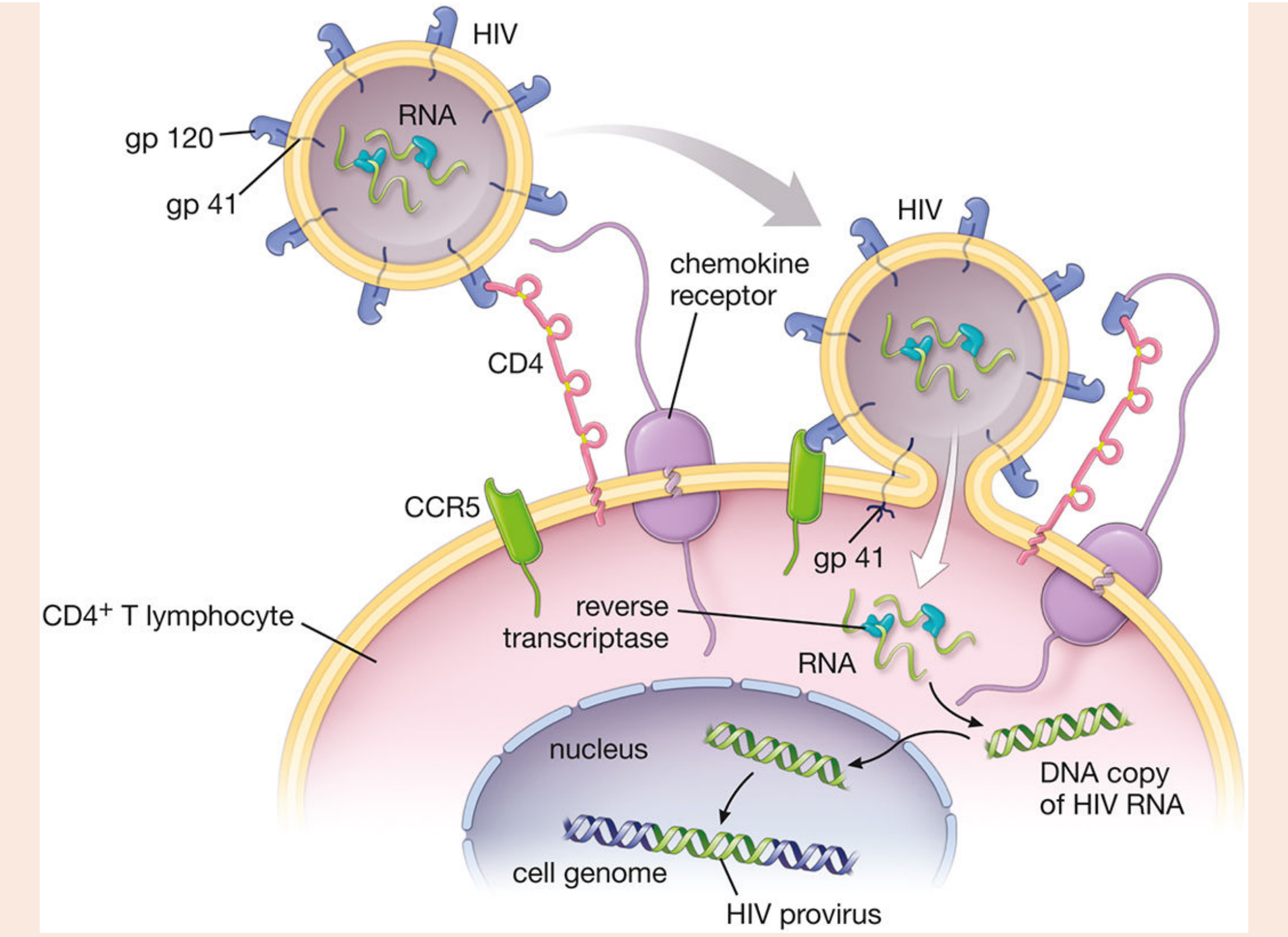
Schematic of HIV interaction with CD4+ T lymphocyte showing receptor binding, reverse transcription, and proviral integration. (Histology: A Text and Atlas)
The immune system responds by generating cytotoxic CD8+ T cells and antibodies against viral particles. CD8+ T cells kill HIV-infected CD4+ T cells, which further reduces the CD4+ count. As CD4+ helper T-cell population becomes progressively depleted, cell-mediated immunity collapses.
Clinical Staging (CDC Classification)
| Stage | CD4 Count | Features |
|---|---|---|
| Stage A (1, 2, 3) | Any | Asymptomatic, acute HIV, or persistent generalized lymphadenopathy |
| Stage B | 200-499 cells/µL | Symptomatic conditions not in Stage C |
| Stage C (AIDS) | < 200 cells/µL | Opportunistic infections and AIDS-defining illnesses |
AIDS is classified as Stage C (CDC): CD4+ count < 200 cells/µL OR diagnosis of one or more AIDS-defining opportunistic illnesses.
AIDS-Defining Opportunistic Illnesses (CDC Stage 3 / AIDS)
- Infections: Pneumocystis jirovecii pneumonia (PCP), Toxoplasmosis of the brain, CMV retinitis, Cryptococcosis, Mycobacterium avium complex (MAC), Histoplasmosis, Cryptosporidiosis, Esophageal/pulmonary Candidiasis, TB, Herpes simplex (chronic)
- Malignancies: Kaposi's sarcoma, Burkitt's lymphoma, Immunoblastic lymphoma, Primary CNS lymphoma, Invasive cervical cancer
- Other: HIV encephalopathy, Wasting syndrome, Progressive multifocal leukoencephalopathy (PML)
Treatment - Antiretroviral Therapy (ART)
- AZT (azidothymidine) was the first drug used, an inhibitor of reverse transcriptase
- Currently, the most effective treatment is multidrug ART (combination therapy):
- NRTIs (nucleoside reverse transcriptase inhibitors) + one of the following:
- NNRTIs (non-nucleoside reverse transcriptase inhibitors)
- Protease inhibitors (block viral protease)
- Integrase strand transfer inhibitors (INSTIs) (prevent viral DNA integration)
- ART offers synergistic effects, reduced side effects, and reduced drug resistance compared to monotherapy
- ART effectively raises CD4+ counts, prevents AIDS, and improves longevity, but does not cure HIV infection
- No vaccine is currently available
Summary Table
| Parameter | Detail |
|---|---|
| Causative agent | HIV-1 / HIV-2 (RNA retrovirus) |
| Target cell | CD4+ helper T lymphocytes |
| Entry receptor | CD4 (with CCR5/CXCR4 co-receptors) |
| Key enzyme | Reverse transcriptase, Integrase |
| AIDS diagnosis | CD4+ < 200/µL or opportunistic illness |
| Treatment | Combination ART |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Histology: A Text and Atlas (Eroschenko); Harrison's Principles of Internal Medicine 22E
In more detail
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
IMMUNITY - Detailed Study Notes
PART 1: DEFINITION OF IMMUNITY
Immunity is defined as the state of protection from infectious disease. In classical terms, it refers to the resistance of a host to pathogens. In its broader sense, however, immunity encompasses:
- Host defense against infections (bacteria, viruses, fungi, parasites)
- Tumor immunity (defense against cancer cells)
- Transplant rejection (immune reactions against foreign tissue)
- Autoimmunity (immune reactions against self antigens)
The immune system is vital for survival because, without it, individuals become easy prey to infections and certain cancers. However, the same immune system can itself cause tissue injury, as seen in allergies, hypersensitivity reactions, and autoimmune diseases.
Robbins, Cotran & Kumar Pathologic Basis of Disease
PART 2: TYPES OF IMMUNITY
The mechanisms of immunity broadly fall into two categories - Innate Immunity and Adaptive Immunity - which together make up a coordinated system of host defense.
2.1 INNATE IMMUNITY (Natural / Native Immunity)
Definition: Innate immunity refers to defense mechanisms that are always present, ready to combat microbes and other offending agents. It is the first line of defense, responding within minutes to hours of infection, before adaptive immunity can develop.
Key Features
| Property | Innate Immunity |
|---|---|
| Onset | Immediate (minutes-hours) |
| Specificity | Broad (recognizes shared patterns) |
| Memory | Absent (or minimal) |
| Receptors | Germline-encoded; identical in all cells |
| Receptor variety | ~100 receptors recognizing ~1000 molecular patterns |
A. Recognition Strategy - PAMPs, DAMPs, and PRRs
The innate immune system does not recognize every unique antigen. Instead it detects conserved molecular structures shared among classes of pathogens:
- PAMPs (Pathogen-Associated Molecular Patterns) - microbial structures that are essential for infectivity (and therefore cannot be easily mutated), e.g., LPS (Gram-negative bacteria), peptidoglycan (Gram-positive), flagellin, viral RNA/DNA, mannans (fungi)
- DAMPs (Damage-Associated Molecular Patterns) - molecules released by injured and necrotic cells, e.g., uric acid, ATP, heat shock proteins, HMGB1, cytosolic DNA
- PRRs (Pattern Recognition Receptors) - cellular receptors that recognize PAMPs and DAMPs; located in all cellular compartments where microbes may be found
B. Classes of Pattern Recognition Receptors
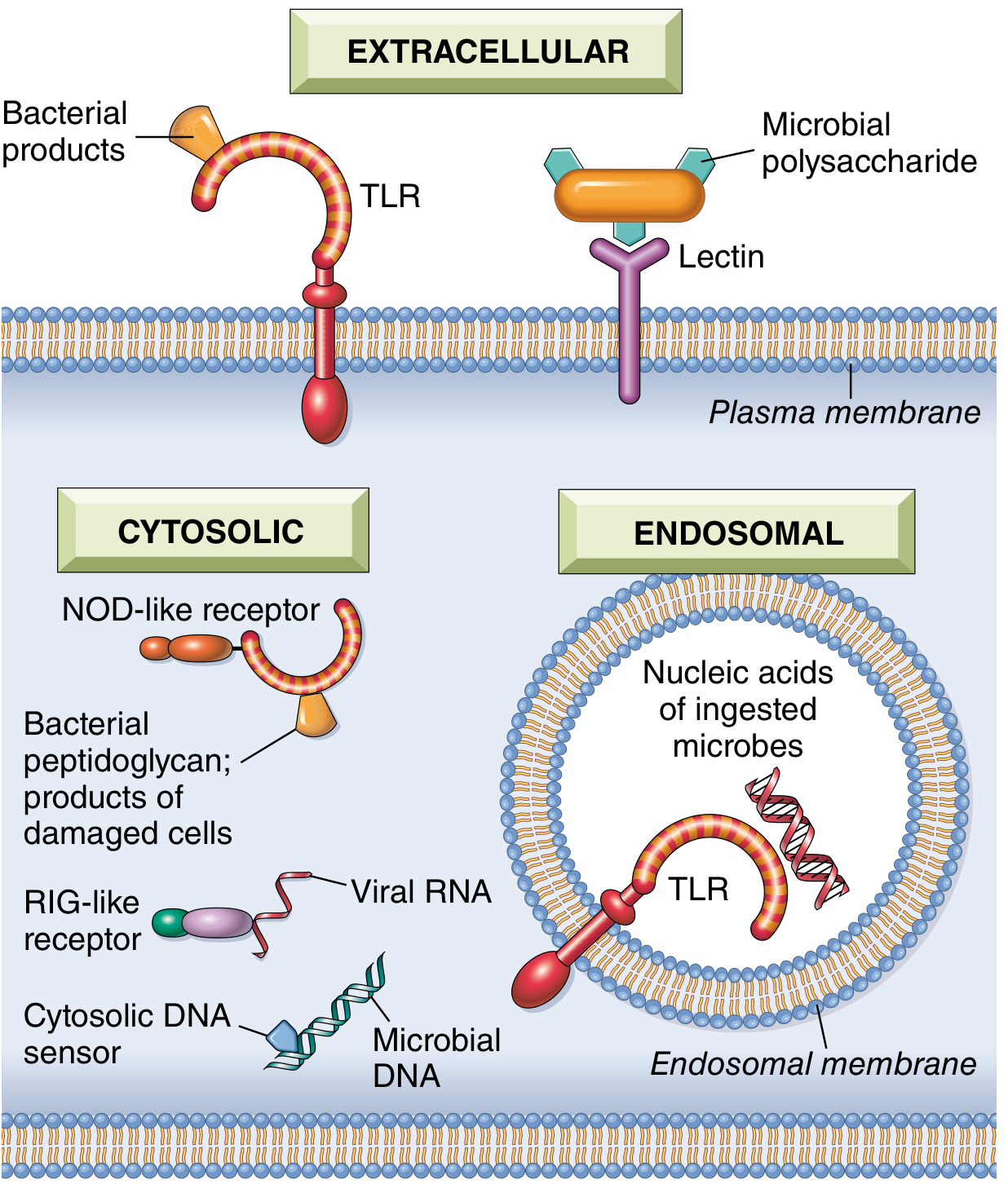
Fig. 6.2 - PRRs in different cellular compartments: plasma membrane TLRs, endosomal TLRs, cytosolic NOD-like receptors, RIG-like receptors, and cytosolic DNA sensors. (Robbins, Cotran & Kumar)
1. Toll-Like Receptors (TLRs)
- Family of 10 receptors in mammals; present on plasma membranes and endosomal vesicles
- Each TLR recognizes a different set of microbial molecules
- Signaling: All TLRs signal via a common pathway activating two transcription factors:
- NF-kB - stimulates synthesis of cytokines and adhesion molecules critical for leukocyte recruitment
- IRFs (Interferon Regulatory Factors) - stimulate production of antiviral type I interferons (IFN-α, IFN-β)
- Examples: TLR4 recognizes LPS; TLR3 recognizes dsRNA; TLR9 recognizes CpG DNA
- Loss-of-function TLR mutations cause rare but serious immunodeficiency syndromes
2. NOD-like Receptors (NLRs) and the Inflammasome
- Cytosolic receptors (named after founding member NOD-2)
- Recognize products of necrotic/damaged cells (uric acid, ATP, K+ loss) and some microbial products
- Several NLRs signal via the inflammasome - a cytosolic multiprotein complex that activates caspase-1, which cleaves pro-IL-1β into biologically active IL-1
- IL-1 promotes fever and acute phase response
- Example: NLRP3 inflammasome detects cholesterol crystals (atherosclerosis) and uric acid crystals (gout)
3. RIG-like Receptors (RLRs)
- Located in the cytosol; detect viral RNA of viruses replicating in the cytosol
- Stimulate production of type I interferon (IFN)
4. Cytosolic DNA Sensors (cGAS-STING pathway)
- Detect microbial (and aberrant self) DNA in the cytosol
- Activate the STING (Stimulator of Interferon Genes) pathway -> type I IFN
- Excessive STING activation causes systemic interferonopathies
5. C-type Lectin Receptors (CLRs / Dectins)
- On plasma membrane of macrophages and DCs
- Recognize fungal glycans and elicit inflammatory responses to fungi
6. Mannose Receptors
- Recognize terminal mannose residues on microbial glycoproteins (unlike mammalian glycoproteins)
- Induce phagocytosis of microbes
C. Cellular Components of Innate Immunity
1. Epithelial Barriers
- Skin, GI tract, and respiratory tract epithelium block physical entry of microbes
- Produce antimicrobial molecules: defensins, lysozyme, collectins
- Intraepithelial lymphocytes combat microbes at these sites
- Mucus trapping and mucociliary clearance in the respiratory tract
2. Phagocytes - Neutrophils and Macrophages
- Neutrophils (PMNs): first cells recruited to sites of infection; kill bacteria by oxidative burst (ROS), lysosomal enzymes (myeloperoxidase), and neutrophil extracellular traps (NETs)
- Macrophages: tissue-resident (Kupffer cells in liver, microglia in brain, alveolar macrophages in lung) or recruited from circulating monocytes; phagocytose and destroy microbes; produce pro-inflammatory cytokines (TNF, IL-1, IL-6, IL-12); act as APCs to initiate adaptive immunity
- Both cell types carry surface receptors for PAMPs and for complement fragments (opsonins)
3. Dendritic Cells (DCs)
- Specialized sentinels present in epithelia, lymphoid organs, and most tissues
- Capture protein antigens and present them to T lymphocytes (antigen-presenting function)
- Rich collection of PRRs; secrete cytokines critical for inflammation and antiviral defense
- Bridge innate and adaptive immunity - upon activation, DCs mature and migrate to lymph nodes to initiate T-cell responses
4. Natural Killer (NK) Cells
- Large granular lymphocytes making up 5-10% of peripheral blood lymphocytes
- Recognize and kill virus-infected cells and tumor cells without prior sensitization
- Mechanism of regulation (missing-self hypothesis):
- Carry activating receptors that recognize stress-induced ligands on infected/tumor cells
- Carry inhibitory receptors that recognize MHC class I molecules on healthy cells
- Virus infection -> upregulates activating ligands + downregulates MHC class I -> NK cell activation and killing
- Express CD16 (FcγRIII) - binds Fc tail of IgG -> antibody-dependent cellular cytotoxicity (ADCC)
- Kill by releasing perforins and granzymes
5. Innate Lymphoid Cells (ILCs)
- Tissue-resident lymphocytes lacking antigen receptors
- Activated by cytokines from sites of tissue damage
- Classified into ILC1, ILC2, ILC3 based on cytokines produced (mirroring Th1, Th2, Th17 T cell subsets)
- Sources of early inflammatory cytokines (IFN-γ, IL-5, IL-17)
6. Mast Cells and Basophils
- Contain granules rich in histamine, heparin, and inflammatory mediators
- Activated by IgE (in allergic reactions) and by PAMPs; release preformed and newly synthesized mediators
D. Soluble Effector Molecules of Innate Immunity
| Molecule | Source | Function |
|---|---|---|
| Complement proteins | Liver | Opsonization, inflammation, cell lysis |
| Mannose-binding lectin (MBL) | Liver | Opsonization; activates lectin complement pathway |
| C-reactive protein (CRP) | Liver | Opsonization; activates classical complement pathway |
| Defensins | Epithelial cells | Direct antimicrobial peptides |
| Type I Interferons (IFN-α/β) | Virally infected cells | Antiviral state; NK cell activation |
| Cytokines (TNF, IL-1, IL-6, IL-12) | Macrophages, DCs | Inflammation, fever, acute phase response |
2.2 ADAPTIVE IMMUNITY (Acquired / Specific Immunity)
Definition: Adaptive immunity consists of mechanisms that are stimulated by ("adapt to") exposure to microbes and foreign substances. It is more powerful but develops more slowly (days). It is characterized by specificity, diversity, memory, and self-limitation.
Key Features Compared to Innate Immunity
| Property | Innate | Adaptive |
|---|---|---|
| Onset | Hours | Days |
| Receptors | Germline-encoded, limited diversity | Somatically recombined, vast diversity |
| Receptor variety | ~100 receptor types | Millions of unique receptors |
| Memory | Absent (or minimal) | Yes (long-lived memory cells) |
| Self-tolerance | Fixed | Actively maintained |
| Specificity | Broad (pattern recognition) | Precise (single antigen) |
A. Two Arms of Adaptive Immunity
1. Humoral Immunity
- Mediated by B lymphocytes and their secreted products: antibodies (immunoglobulins)
- Protects against extracellular microbes and their toxins
- Antibody functions: neutralization, opsonization (enhanced phagocytosis), complement activation, ADCC, neonatal immunity (IgG crosses placenta; IgA in breast milk)
2. Cell-Mediated Immunity
- Mediated by T lymphocytes
- Responsible for defense against intracellular microbes (viruses, mycobacteria) and cancer cells
- Also mediates delayed-type hypersensitivity and transplant rejection
B. Lymphocytes - The Key Cells of Adaptive Immunity
Clonal Selection: The fundamental concept. Lymphocytes specific for many antigens pre-exist before antigen exposure. When antigen appears, it selectively activates antigen-specific lymphocytes. Each clone bears identical receptors; there are approximately 10^12 lymphocytes in a healthy adult.
Naive vs. Effector vs. Memory Cells:
- Naive: Mature lymphocytes that have never encountered their antigen; circulate among blood, lymphoid organs, and tissues
- Effector: Activated lymphocytes that perform immune functions (killing, antibody production)
- Memory: Long-lived cells that survive after infection is cleared; respond faster and more vigorously upon re-exposure (basis of vaccination)
C. T Lymphocytes
T cells are thymus-derived and express the T-cell receptor (TCR), which recognizes peptide fragments of antigens displayed by MHC molecules on antigen-presenting cells (APCs).
Key Subsets:
| Subset | Surface Marker | MHC Restriction | Function |
|---|---|---|---|
| Helper T cells | CD4+ | MHC Class II | Activate macrophages, help B cells produce antibodies, coordinate immune response via cytokines |
| Cytotoxic T lymphocytes (CTLs) | CD8+ | MHC Class I | Kill virus-infected cells and tumor cells |
| Regulatory T cells (Tregs) | CD4+CD25+FoxP3+ | MHC Class II | Suppress immune responses; prevent autoimmunity |
CD4+ Helper T Cell Subsets (Th cells):
| Subset | Key Cytokine | Functions |
|---|---|---|
| Th1 | IFN-γ | Macrophage activation; defense against intracellular pathogens |
| Th2 | IL-4, IL-5, IL-13 | B cell activation; IgE production; eosinophil activation; allergy |
| Th17 | IL-17, IL-22 | Defense against extracellular bacteria and fungi at mucosal surfaces |
| Tfh (T follicular helper) | IL-21 | Help B cells in germinal centers; antibody class switching |
MHC Restriction - Critical Concept:
- MHC Class I molecules (HLA-A, HLA-B, HLA-C): expressed on all nucleated cells and platelets; present peptides from cytosolic (intracellular) proteins (viruses, tumor antigens) to CD8+ CTLs
- MHC Class II molecules (HLA-DP, HLA-DQ, HLA-DR): expressed on professional APCs only (DCs, macrophages, B cells); present peptides from exogenous (endocytosed) antigens to CD4+ T cells
- The HLA system is highly polymorphic (thousands of alleles in humans), making it a major barrier to organ transplantation
T Cell Activation requires TWO signals:
- Signal 1 - TCR binds MHC-peptide complex on APC
- Signal 2 - Costimulatory molecules: CD28 on T cell binds B7 (CD80/CD86) on APC
- Without Signal 2 -> anergy (tolerance, not activation)
- Activated T cells produce IL-2 (autocrine growth factor) and express IL-2R -> clonal expansion
D. B Lymphocytes and Humoral Immunity
- B cells (bone marrow-derived) express membrane-bound immunoglobulins as their antigen receptors (BCR)
- BCR can recognize native antigens (proteins, polysaccharides, lipids, nucleic acids) directly - no MHC presentation required
- When activated, B cells:
- Proliferate
- Differentiate into plasma cells (secrete antibodies) and memory B cells
- Undergo somatic hypermutation (in germinal centers) -> affinity maturation
- Undergo class switching (IgM -> IgG, IgA, IgE) under cytokine influence from Th cells
Antibody Isotypes and Functions:
| Isotype | Major Function |
|---|---|
| IgM | First antibody produced; strong complement activator; pentameric |
| IgG | Most abundant; opsonization; complement activation; placental transfer; ADCC |
| IgA | Mucosal immunity (saliva, tears, breast milk, GI/respiratory secretions) |
| IgE | Allergic reactions; antiparasitic immunity; binds mast cells/basophils |
| IgD | B-cell surface receptor; function poorly understood |
2.3 OTHER CLASSIFICATIONS OF IMMUNITY
Active Immunity
- Generated by the individual's own immune response
- Natural active: result of infection
- Artificial active: result of vaccination
- Characterized by immunologic memory; long-lasting (years to lifetime)
Passive Immunity
- Conferred by transfer of preformed antibodies
- Natural passive: maternal IgG across the placenta; IgA via breast milk
- Artificial passive: injection of immunoglobulins (e.g., anti-tetanus, anti-rabies)
- No memory generated; immediate but short-lived (weeks to months)
Herd (Community) Immunity
- When a sufficient proportion of a population is immune, unimmunized individuals are indirectly protected because the chain of transmission is broken
PART 3: THE COMPLEMENT SYSTEM - IN DETAIL
3.1 Definition and Overview
The complement system is a collection of more than 20 plasma proteins (soluble proteins and their membrane receptors) that function in host defense against microbes and in pathologic inflammatory reactions. Some proteins are numbered C1 through C9; others include factors B, D, P (properdin), MBL-associated serine proteases (MASPs), and regulatory proteins.
The complement proteins exist in plasma in inactive proforms. They are activated during inflammatory reactions in a cascade of enzymatic reactions capable of tremendous amplification - each enzyme step activates multiple substrate molecules.
Complement participates in both innate and adaptive immunity:
- Alternative and lectin pathways function in innate immunity (no antibody needed)
- Classical pathway links adaptive immunity (antibodies) to complement
3.2 The Three Activation Pathways
The pivotal step in all three pathways is proteolytic cleavage of C3, the most abundant complement component.
PATHWAY 1: CLASSICAL PATHWAY
Trigger: Binding of C1 to antibody (IgM or IgG) that has combined with antigen
Sequence:
- C1 (a complex of C1q, C1r, C1s) binds via C1q to the Fc region of antibody-antigen complexes
- C1q binding activates C1r, which activates C1s (a protease)
- C1s cleaves C4 into C4a (released) and C4b (covalently binds surface)
- C4b binds C2; C1s cleaves C2 into C2a and C2b
- C4b2a = Classical C3 convertase (cleaves C3)
- C4b2a3b = Classical C5 convertase (cleaves C5)
Key points:
- Requires preformed antibody -> bridges adaptive and innate immunity
- IgM is the most efficient complement activator (one molecule); IgG requires multiple molecules
PATHWAY 2: ALTERNATIVE PATHWAY
Trigger: Microbial surface molecules - LPS (endotoxin), complex polysaccharides, cobra venom, zymosan (fungal cell wall) - in the absence of antibody
Sequence:
- C3 undergoes slow spontaneous hydrolysis in plasma (C3 "tick-over") generating C3(H2O)
- C3(H2O) binds Factor B; Factor D (circulating protease) cleaves Factor B into Ba and Bb
- C3(H2O)Bb = initial C3 convertase, cleaves C3 into C3a and C3b
- C3b is deposited on microbial surfaces; binds Factor B; Factor D cleaves to form C3bBb = Alternative C3 convertase
- Properdin (Factor P) stabilizes C3bBb (extends its half-life)
- C3bBbC3b = Alternative C5 convertase
Amplification loop: C3b produced by any pathway can re-enter the alternative pathway and generate more C3b -> amplification of complement activation on microbial surfaces
PATHWAY 3: LECTIN PATHWAY (Mannose-Binding Lectin Pathway)
Trigger: Plasma Mannose-Binding Lectin (MBL) binds to mannose residues on microbial carbohydrates (mammalian glycoproteins typically have terminal sialic acid, not mannose)
Sequence:
- MBL binds microbial mannose residues; MBL is associated with MASPs (MBL-Associated Serine Proteases) - MASP-1 and MASP-2
- MASP-2 (homologous to C1s) cleaves C4 and C2
- Subsequent steps identical to classical pathway
- C4b2a = Lectin pathway C3 convertase
Key points:
- Antibody-independent innate immune pathway
- MBL is an acute-phase protein; levels rise during infection
Common Convergence Point
All three pathways generate C3 convertase, which cleaves C3 into:
- C3a (released into plasma - anaphylatoxin)
- C3b (covalently deposited on the activating surface - opsonin)
C3b then binds the respective C3 convertase to form C5 convertase, which cleaves C5 into:
- C5a (released - most potent anaphylatoxin and chemotactic factor)
- C5b (stays on surface - nucleates MAC formation)
3.3 Terminal Pathway - Membrane Attack Complex (MAC)
Formation:
- C5b binds C6, then C7 (C5b-7 complex inserts into lipid bilayer)
- C8 binds C5b-7
- Multiple C9 molecules polymerize around C5b-8 to form the MAC (C5b-6789n)
Result:
- MAC creates a transmembrane pore (10 nm diameter) in the cell membrane
- Allows free flow of water and ions into the cell -> osmotic lysis
- Effective against microbes with thin cell walls, especially Neisseria (gonorrhea, meningitis)
Fig. 3.11 - The three activation pathways converging on C3 convertase; effector functions of C3a/C5a (inflammation), C3b (opsonization), and MAC (cell lysis). (Robbins, Cotran & Kumar Pathologic Basis of Disease)
3.4 Functions of the Complement System
Function 1 - Inflammation (Anaphylatoxins)
C5a is the most potent; C3a and C4a are weaker anaphylatoxins.
Actions:
- Histamine release from mast cells and basophils -> vasodilation and increased vascular permeability
- Chemotaxis: C5a is a powerful chemotactic agent for neutrophils, monocytes, eosinophils, and basophils; recruits them to sites of infection
- Leukocyte activation: C5a activates the lipoxygenase pathway in neutrophils/monocytes -> further release of inflammatory mediators (leukotrienes)
- Called "anaphylatoxins" because their effects resemble those of mast cell mediators in anaphylaxis
Function 2 - Opsonization and Phagocytosis
- C3b and its cleavage product iC3b (inactive C3b), when fixed to microbial cell walls, act as opsonins
- Phagocytes (neutrophils and macrophages) express surface receptors for complement fragments:
- CR1 (CD35) - binds C3b and C4b
- CR3 (CD11b/CD18) - binds iC3b
- Opsonized microbes are recognized and efficiently phagocytosed
- This function is especially important for encapsulated bacteria (S. pneumoniae, H. influenzae) that resist phagocytosis otherwise
Function 3 - Cell Lysis via MAC
- As described above, the MAC creates pores in cell membranes -> osmotic lysis
- Critical against thin-walled microbes especially Neisseria meningitidis and N. gonorrhoeae
- Deficiency of terminal complement components (C5-C9) -> recurrent Neisseria infections
3.5 Regulation of Complement Activation
Complement regulation is essential to protect host cells from inadvertent injury. Regulatory proteins are expressed on normal cells and are designed to limit complement deposition on host tissues.
| Regulatory Protein | Location | Mechanism | Clinical Significance |
|---|---|---|---|
| C1 Inhibitor (C1-INH) | Plasma | Blocks and inactivates activated C1r and C1s; limits classical pathway activation | Deficiency causes Hereditary Angioedema (HAE) - episodes of swelling (bradykinin-mediated) |
| C4b-binding protein (C4BP) | Plasma | Binds C4b; accelerates decay of C3 convertase; cofactor for Factor I | |
| Factor I | Plasma | Serine protease that cleaves C3b and C4b (requires cofactors: Factor H, C4BP, MCP) | Deficiency causes secondary C3 consumption and susceptibility to infections |
| Factor H | Plasma | Competes with Factor B for C3b binding; cofactor for Factor I; promotes C3b cleavage; limits alternative pathway | Mutations/polymorphisms cause atypical Hemolytic Uremic Syndrome (aHUS) and Age-related Macular Degeneration (AMD) |
| Decay Accelerating Factor (DAF / CD55) | Cell surface (GPI-anchored) | Accelerates decay of C3 and C5 convertases on host cell surfaces; prevents complement build-up | GPI deficiency in Paroxysmal Nocturnal Hemoglobinuria (PNH) |
| CD59 (Protectin / MIRL) | Cell surface (GPI-anchored) | Binds C5b-8 and prevents C9 polymerization; blocks MAC formation on host cells | GPI deficiency in PNH -> complement-mediated lysis of RBCs, WBCs, and platelets |
| Membrane Cofactor Protein (MCP / CD46) | Cell surface | Cofactor for Factor I-mediated cleavage of C3b and C4b | Mutations cause aHUS |
| Clusterin and Vitronectin (S protein) | Plasma | Bind to C5b-7 complex; prevent MAC insertion into host cell membranes (fluid-phase MAC inhibitors) |
Paroxysmal Nocturnal Hemoglobinuria (PNH): An acquired clonal disorder caused by a somatic mutation in the PIG-A gene (which encodes an enzyme required for GPI anchor biosynthesis). This results in deficiency of all GPI-anchored proteins on hematopoietic cells, including CD55 and CD59 -> uncontrolled complement activation -> intravascular hemolysis, thrombosis, cytopenias.
3.6 Complement in Disease
| Disorder | Complement Mechanism |
|---|---|
| Hereditary Angioedema | C1-INH deficiency -> uncontrolled C4/C2 cleavage and bradykinin generation -> episodic angioedema |
| Paroxysmal Nocturnal Hemoglobinuria | PIG-A mutation -> loss of CD55/CD59 -> RBC lysis |
| Atypical HUS | Factor H/I/MCP mutations -> uncontrolled alternative pathway -> endothelial damage, thrombosis |
| Age-related Macular Degeneration | Factor H polymorphisms -> complement dysregulation in retina |
| SLE / Immune complex diseases | Classical pathway activated by immune complexes -> tissue injury |
| Neisseria infections | C5-C9 deficiency -> inability to form MAC -> recurrent Neisseria bacteremia/meningitis |
| C3 deficiency | Recurrent pyogenic infections, immune complex diseases (SLE-like) |
| C1q/C4/C2 deficiency | SLE-like autoimmune disease (impaired clearance of apoptotic cells and immune complexes) |
Therapeutic Complement Inhibitors (approved):
- Eculizumab (anti-C5 monoclonal antibody) - approved for PNH and aHUS
- Ravulizumab (longer-acting anti-C5) - PNH
- Pegcetacoplan (C3 inhibitor) - PNH
- Avacopan (C5a receptor antagonist) - ANCA vasculitis
PART 4: AIDS - A DETAILED NOTE
4.1 Introduction and Epidemiology
Acquired Immunodeficiency Syndrome (AIDS) is caused by the Human Immunodeficiency Virus (HIV), an RNA retrovirus of the lentivirus family. HIV is one of the most significant global health challenges of the 20th and 21st centuries.
Global Statistics (Harrison's Principles, 2025):
- An estimated 88.4 million people have become infected with HIV since the start of the pandemic
- In 2023, 1.3 million new infections occurred worldwide (including 120,000 children <15 years)
- 30.7 million people (77% of all HIV-positive individuals) are currently on antiretroviral therapy (ART)
- Sub-Saharan Africa (WHO Eastern and Southern Africa region) is most severely affected: >5.7% adult prevalence, >50% of worldwide HIV burden
Two Types of HIV:
- HIV-1: Responsible for most infections worldwide; divided into groups M, N, O, P; Group M has subtypes A-K; Subtype C is most prevalent globally (~50% of infections); Subtype B predominates in Western countries
- HIV-2: Less virulent; lower transmissibility; mainly in West Africa; lacks the vpu gene (has vpx instead)
4.2 Structure of HIV
HIV-1 is a spherical enveloped retrovirus, ~120 nm in diameter.
Key structural components:
- Envelope glycoproteins: gp120 (surface unit - binds CD4) and gp41 (transmembrane unit - mediates membrane fusion)
- Core (capsid): p24 protein
- Matrix: p17/p18 proteins (inner membrane lining)
- Genome: Two copies of single-stranded (+) RNA with reverse transcriptase, integrase, and protease
- Key genes:
- gag - encodes core structural proteins (p24, p17)
- pol - encodes reverse transcriptase, integrase, protease
- env - encodes envelope glycoproteins (gp120, gp41)
- tat, rev - regulatory genes
- nef, vif, vpr, vpu - accessory genes that enhance viral replication and pathogenesis
- LTRs (Long Terminal Repeats) - flank the genome; contain regulatory elements for gene expression
4.3 Transmission
HIV is transmitted by:
- Sexual contact (most common globally) - both heterosexual and male-to-male; mucosal trauma facilitates entry
- Blood and blood products - transfusions, needle sharing among injection drug users
- Vertical (mother-to-child) transmission:
- Intrapartum (during delivery) - most common
- Perinatally (in utero) - less common
- Via breast milk (postnatal)
- Occupational exposure - needlestick injuries in healthcare workers
HIV is NOT transmitted by: casual contact, air, water, food, insect bites, shared utensils, hugging, coughing, or any other route.
4.4 Pathogenesis of HIV Disease
Step 1 - Entry into CD4+ T Cells
- gp120 on the HIV envelope binds the CD4 receptor on helper T cells with high affinity
- This binding induces a conformational change, exposing a co-receptor binding site on gp120
- gp120 then binds a co-receptor:
- CCR5 (C-C chemokine receptor 5) - used by R5-tropic (macrophage-tropic) viruses, predominantly during early/transmitted infection
- CXCR4 (CXC chemokine receptor 4) - used by X4-tropic (T-cell-tropic) viruses, emerging in later disease stages
- Co-receptor binding exposes gp41, which anchors the virus into the T-cell membrane and mediates fusion of viral and cellular membranes
- Viral RNA with reverse transcriptase is injected into the T-cell cytoplasm
Schematic of HIV-T cell interaction: gp120 binds CD4, co-receptor binding exposes gp41, viral RNA enters cytoplasm, reverse transcriptase generates DNA, proviral integration. (Histology: A Text and Atlas, Eroschenko)
Important: Individuals with homozygous CCR5 deletion (Δ32 mutation) are highly resistant to HIV infection, as R5-tropic viruses (which dominate early infection) cannot enter their cells.
Step 2 - Reverse Transcription and Integration
- Reverse transcriptase converts viral ssRNA into double-stranded viral DNA (error-prone, ~1 error per genome per cycle - source of HIV's extraordinary genetic diversity and drug resistance)
- The newly synthesized viral DNA (with the viral integrase enzyme) is transported into the nucleus
- Integrase inserts the viral DNA into the host cell genome -> provirus
- The provirus can remain latent for years (in resting CD4+ T cells) - this forms the latent reservoir, the primary barrier to cure
Step 3 - Viral Replication and Spread
- Activation of the infected T cell (e.g., by another infection or antigen) triggers transcription of the provirus
- New viral RNA is transcribed, translated, and viral proteins are assembled
- New virus particles bud from the T-cell surface, acquiring their lipid envelope in the process
- Viral protease cleaves polyproteins into mature viral proteins during or after budding (essential for infectivity)
- New virions infect other CD4+ T cells, macrophages, and dendritic cells
Step 4 - Acute HIV Infection
- Occurs 2-4 weeks after initial infection in ~50% of individuals
- Characterized by high-level plasma viremia (millions of copies/mL)
- Acute mononucleosis-like syndrome: fever, lymphadenopathy, pharyngitis, rash, myalgias, headache
- Massive viral replication in gut-associated lymphoid tissue (GALT) depletes CD4+ T cells from the intestinal mucosa
- Immune response (CD8+ CTLs, antibodies) partially controls viremia -> viral set point is established
- The viral set point (after ~1 year) correlates with the rate of long-term disease progression
Step 5 - Chronic HIV Infection and CD4+ T-Cell Depletion
Mechanisms of CD4+ T-cell loss:
- Direct cytopathic effects of viral replication in CD4+ T cells (most important)
- CD8+ CTL killing of HIV-infected CD4+ T cells
- Pyroptosis - inflammatory caspase-1-dependent cell death; HIV replication in GALT triggers IL-1β and IL-18 release -> bystander killing of uninfected CD4+ T cells
- Depletion in GALT of IL-17-producing T cells -> impaired defense against extracellular bacteria and fungi at mucosal surfaces
- Microbial translocation: HIV damages gut mucosal barrier -> bacterial LPS enters circulation -> chronic systemic immune activation -> drives HIV replication (vicious cycle) and contributes to non-AIDS comorbidities
Step 6 - Persistent Immune Activation
- HIV replication is persistent and drives chronic immune activation throughout the course of untreated disease
- HIV replicates most efficiently in activated CD4+ T cells - chronic activation fuels further viral replication
- Even in patients on ART with suppressed viremia (<20 copies/mL), low-level immune activation persists due to:
- Residual low-level viral replication
- Transcription from defective integrated proviruses
- Microbial translocation
- Chronic immune activation contributes to non-AIDS comorbidities:
- Accelerated cardiovascular disease
- Metabolic disorders (diabetes, dyslipidemia)
- Bone fragility
- Non-AIDS cancers
- Neurocognitive dysfunction
- Accelerated aging syndrome
4.5 Clinical Stages of HIV/AIDS
Stage A - Acute and Early Infection
- Primary HIV infection (acute retroviral syndrome, if symptomatic)
- Asymptomatic infection - may last years (average ~10 years without treatment)
- Persistent Generalized Lymphadenopathy (PGL) - lymph node enlargement >1 cm in 2 or more non-contiguous sites for >3 months
- CD4+ count: typically >500 cells/µL
Stage B - Symptomatic, Non-AIDS
- CD4+ count: 200-499 cells/µL
- Conditions attributable to HIV-related immunodeficiency but not AIDS-defining:
- Oral thrush (oropharyngeal candidiasis)
- Recurrent vaginal candidiasis
- Oral hairy leukoplakia (EBV)
- Herpes zoster (shingles)
- Constitutional symptoms (fever, night sweats, weight loss)
- Peripheral neuropathy
Stage C - AIDS (Advanced HIV Disease)
Diagnosis of AIDS requires: CD4+ count < 200 cells/µL AND/OR presence of an AIDS-defining condition (regardless of CD4+ count)
CDC AIDS-Defining Illnesses (Stage 3 Opportunistic Illnesses):
| Category | Examples |
|---|---|
| Pulmonary | Pneumocystis jirovecii pneumonia (PCP), recurrent pneumonia, pulmonary TB |
| CNS | Toxoplasmosis of brain, Cryptococcal meningitis, Primary CNS lymphoma, Progressive multifocal leukoencephalopathy (PML - JC virus), HIV encephalopathy |
| GI | Esophageal candidiasis, CMV colitis, Cryptosporidiosis (chronic, >1 month), Isosporiasis |
| Disseminated | Mycobacterium avium complex (MAC), Histoplasmosis, Coccidioidomycosis, CMV (non-GI) |
| Skin/Eyes | Kaposi's sarcoma, CMV retinitis, Herpes simplex (chronic >1 month) |
| Cancers | Kaposi's sarcoma, Burkitt's lymphoma, Immunoblastic lymphoma, Primary CNS lymphoma, Invasive cervical cancer |
| Systemic | HIV wasting syndrome, Salmonella septicemia (recurrent) |
| Bacteremia | Multiple/recurrent bacterial infections (in children) |
PCP (Pneumocystis jirovecii pneumonia) is the most common AIDS-defining opportunistic infection in developed countries.
Mycobacterium tuberculosis is the most common opportunistic infection globally in people with HIV.
4.6 Laboratory Monitoring
| Test | Purpose | Target Values |
|---|---|---|
| CD4+ T-cell count | Indicator of immunodeficiency; guides prophylaxis and ART initiation | >500: normal; 200-500: moderate immunosuppression; <200: AIDS |
| HIV viral load (HIV RNA copies/mL) | Reflects active replication; best predictor of progression; ART monitoring | Goal: undetectable (<20-50 copies/mL) on ART |
| HIV antibody/antigen tests | Diagnosis | 4th-generation p24Ag+HIV Ab combo tests detect infection ~2-3 weeks after exposure |
| CD4:CD8 ratio | Disease progression monitoring | Normal ~2:1; inverted in AIDS |
| Resistance testing (genotypic) | Guide ART selection, especially on failing regimen |
4.7 Antiretroviral Therapy (ART)
ART does not cure HIV but suppresses viral replication to undetectable levels, allowing immune reconstitution, preventing AIDS-defining illnesses, and dramatically extending life expectancy.
Classes of Antiretroviral Drugs:
| Class | Mechanism | Examples |
|---|---|---|
| NRTIs (Nucleoside Reverse Transcriptase Inhibitors) | Competitive inhibitors of reverse transcriptase; chain terminators | Zidovudine (AZT), Tenofovir, Emtricitabine, Lamivudine, Abacavir |
| NNRTIs (Non-Nucleoside Reverse Transcriptase Inhibitors) | Non-competitive allosteric inhibitors of reverse transcriptase | Efavirenz, Nevirapine, Rilpivirine, Doravirine |
| Protease Inhibitors (PIs) | Block viral protease -> prevent maturation of viral particles | Ritonavir, Atazanavir, Darunavir, Lopinavir |
| INSTIs (Integrase Strand Transfer Inhibitors) | Block HIV integrase -> prevent viral DNA integration | Raltegravir, Dolutegravir, Bictegravir, Cabotegravir |
| Entry Inhibitors / Fusion Inhibitors | Block gp41-mediated fusion | Enfuvirtide (T-20), Ibalizumab |
| CCR5 Antagonists | Block CCR5 co-receptor | Maraviroc |
Standard ART Regimen (current preferred):
- 2 NRTIs + 1 INSTI (e.g., Tenofovir-Emtricitabine + Dolutegravir or Bictegravir)
- ART is now recommended for all HIV-infected individuals regardless of CD4+ count
- ART also prevents transmission: U=U (Undetectable = Untransmittable) - individuals with sustained undetectable viral load cannot sexually transmit HIV
PMTCT (Prevention of Mother-to-Child Transmission): Maternal ART during pregnancy, IV zidovudine during labor, infant prophylaxis, and avoidance of breastfeeding (where safe) can reduce transmission to <2%.
4.8 Prevention
- Pre-Exposure Prophylaxis (PrEP): Daily tenofovir-emtricitabine (or cabotegravir long-acting injectable) for HIV-negative high-risk individuals; >99% effective when taken correctly
- Post-Exposure Prophylaxis (PEP): 28-day ART course started within 72 hours of exposure
- Condom use, harm reduction programs, needle exchange programs
- No licensed HIV vaccine currently exists, though research continues
4.9 Summary Table - AIDS
| Parameter | Detail |
|---|---|
| Causative agent | HIV-1 (predominantly) / HIV-2 |
| Viral type | RNA retrovirus (lentivirus family) |
| Primary target cell | CD4+ helper T lymphocytes (also macrophages, DCs) |
| Entry receptor | CD4 + CCR5 or CXCR4 co-receptor |
| Key viral enzyme | Reverse transcriptase, Integrase, Protease |
| AIDS diagnosis | CD4+ <200/µL OR CDC-defined opportunistic illness |
| Latent reservoir | Resting CD4+ T cells (major barrier to cure) |
| Treatment | Combination ART (2 NRTIs + INSTI preferred) |
| Goal of ART | Undetectable viral load, CD4+ restoration |
| Prognosis with ART | Near-normal life expectancy |
| No cure/vaccine | Currently unavailable |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease 11th ed.; Cellular and Molecular Immunology (Abbas, Lichtman & Pillai); Histology: A Text and Atlas (Eroschenko); Harrison's Principles of Internal Medicine 22nd Edition (2025)
This is a shared conversation. Sign in to Orris to start your own chat.