myasthenia gravis consultant level
Reading File
Finding Sources
Searching PubMed
"myasthenia gravis"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content to write a full consultant-level review. Let me compile the answer:
Myasthenia Gravis: Consultant-Level Review
1. Definition and Epidemiology
Myasthenia gravis (MG) is the most common primary disorder of neuromuscular transmission (NMT). It is an autoimmune disease in which circulating antibodies target proteins at the neuromuscular junction (NMJ), most commonly the acetylcholine receptor (AChR), disrupting normal transmission and producing fatigable muscle weakness. The NMJ lacks a blood-nerve barrier, making it uniquely vulnerable to circulating immune factors.
Epidemiology:
- US prevalence ~20/100,000 (~60,000 patients); increasing over the past 50 years due to better ascertainment, older populations, and reduced mortality
- Bimodal distribution: early onset peak in 2nd-3rd decades (female predominance, ~3:1 F:M below age 40); late onset peak in 6th-8th decades (male predominance)
- The majority of US MG patients are now over age 50, with men now outnumbering women overall
- Bradley and Daroff's Neurology in Clinical Practice, p. 2770
2. Pathophysiology
2a. AChR-Antibody MG (85% of generalized MG)
Three antibody mechanisms damage the postsynaptic membrane:
| Mechanism | Effect |
|---|---|
| Binding antibodies | Complement activation → destruction of postsynaptic junctional folds + AChR |
| Blocking antibodies | Directly prevent ACh binding to AChR |
| Modulating antibodies | Cross-link receptor subunits → internalization/degradation; associated with thymoma |
Net result: with repetitive use, fewer receptor sites are available for ACh, producing the hallmark fatigable weakness.
2b. MuSK-Antibody MG (~10% of generalized MG; up to 50% of seronegative GMG)
Antibodies target muscle-specific tyrosine kinase (MuSK), a surface membrane component essential for NMJ development. Key distinctions:
- More commonly affects bulbar, facial, and neck muscles - respiratory crisis is more frequent and severe
- Patients may worsen with cholinesterase inhibitors (ChEIs) - unlike AChR-MG
- Responds well to plasma exchange and rituximab
- Thymic pathology is less common
2c. LRP4-Antibody MG (minority of double-seronegative patients)
LRP4 (low-density lipoprotein receptor-related protein 4) is a co-receptor for agrin and MuSK signalling. Typically milder phenotype.
2d. Seronegative MG
~15% of GMG patients are seronegative for AChR, MuSK, and LRP4 antibodies. Still autoimmune in pathophysiology (PLEX and IVIg may confirm this); some have low-affinity cell-bound AChR antibodies detectable only by specialised assays.
- Robbins & Kumar Basic Pathology, p. 507-511; Bradley and Daroff's Neurology, p. 2775
3. Thymic Pathology
Thymic abnormalities occur in ~75% of patients:
- Thymic hyperplasia (germinal centre formation): 60-70% of cases - predominantly in younger, AChR-antibody positive women
- Thymoma (neoplasm of thymic epithelium): 10-15% of cases - nearly all thymomatous MG patients have elevated AChR-abs; "modulating" antibodies predominate
- Thymoma is a paraneoplastic cause of MG; initial evaluation requires CT thorax with contrast
4. Clinical Presentation
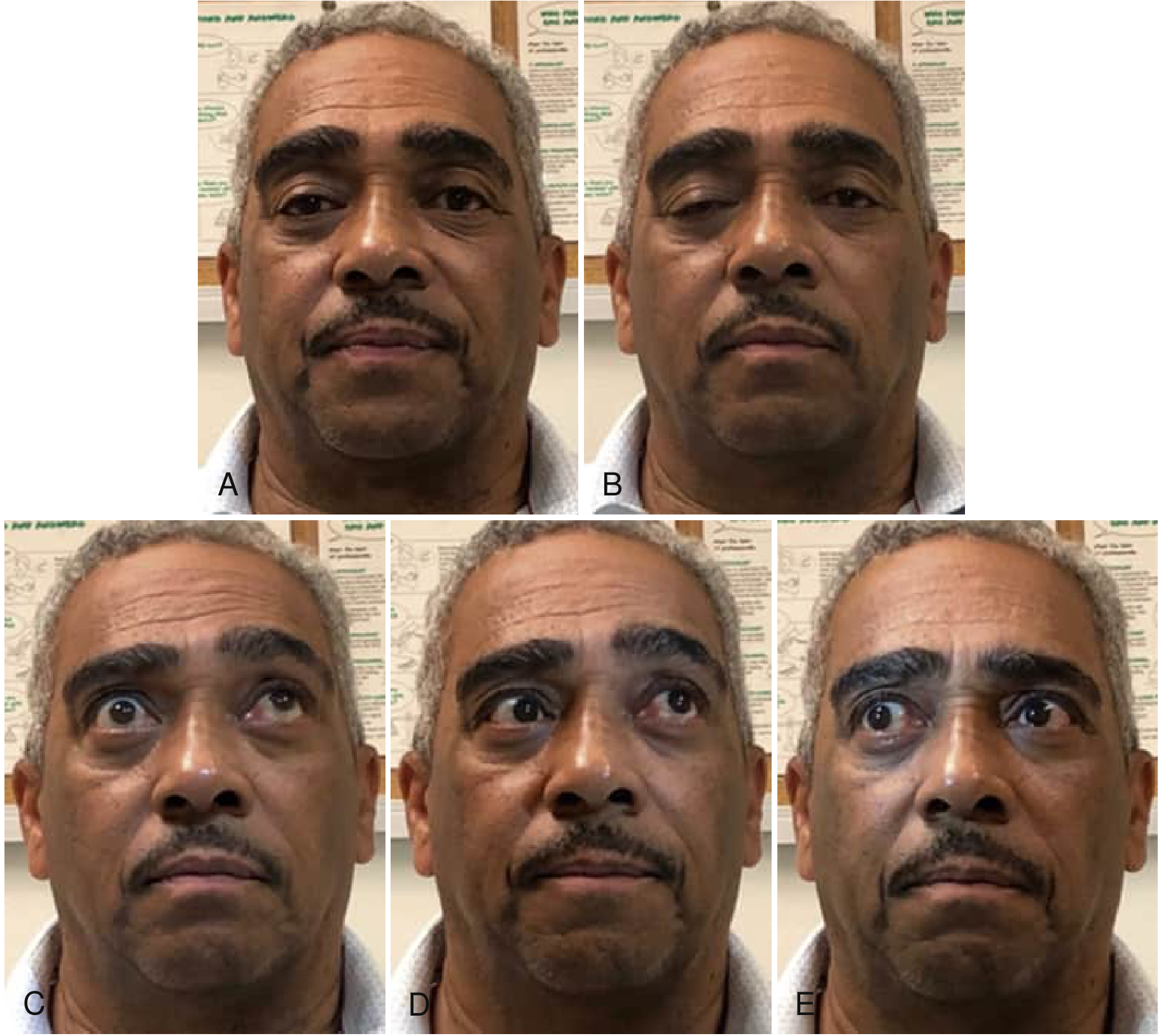
Ocular (earliest and most common features)
- Ptosis and diplopia are the initial symptom in ~two-thirds of patients
- Nearly all develop both within 2 years of onset
- Ptosis worsens with sustained upgaze (fatigable - see image below); typically worst in the evening
- Ice bag test: improvement in ptosis ≥2 mm after 2 min of ice application has pooled sensitivity 0.94, specificity 0.97
Bulbar
- Dysarthria (nasal, slurred voice worsening over conversation), dysphagia, and difficulty chewing are initial symptoms in ~1 in 6 patients
- "Dropped head" syndrome from neck extensor weakness
Limb/Generalised
- Proximal limb weakness (difficulty combing hair, rising from chair)
- Weakness least in morning, worsens through the day and with exercise
Respiratory
- Rarely the presenting symptom but may develop in bulbar-prominent MG
- Forced vital capacity (FVC) and negative inspiratory force (NIF) are the key bedside monitors
Two clinical forms:
- Ocular MG (OMG): weakness confined to ocular muscles; ~50% of OMG patients will generalise within 2 years; seropositivity is ~50%
- Generalised MG (GMG): ocular plus bulbar/limb/respiratory involvement
5. Diagnosis
Serological Testing (first-line)
| Antibody | Sensitivity (GMG) | Sensitivity (OMG) | Notes |
|---|---|---|---|
| AChR binding | ~85% | ~50% | Specific; near 100% specificity for MG |
| AChR blocking | ~55% | Add-on if binding negative | |
| MuSK | Up to 50% of AChR-neg GMG | Order in AChR-seronegative patients | |
| LRP4 | Minority of double-seroneg | Specialised labs |
- False positives occur in: autoimmune liver disease, SLE, inflammatory neuropathies, ALS, penicillamine-treated RA, thymoma without MG
- AChR-ab level does not reliably correlate with disease severity and should not be used to monitor clinical response alone
- Repeat testing is appropriate if initial testing within 6-12 months of symptom onset was negative
Electrodiagnostic Studies
Repetitive nerve stimulation (RNS):
- Decrement in compound muscle action potential (CMAP) amplitude >10-15% at 2-3 Hz stimulation
- Sensitivity ~50-75% for GMG; lower for OMG
- Proximal muscles (trapezius, facial) have higher yield
Single-fibre EMG (SFEMG):
- Most sensitive test for NMJ dysfunction
- Increased jitter (variability in inter-potential interval) and blocking
- Sensitivity >95% for GMG if proximal muscles tested
- Not specific for MG (abnormal in any NMJ disorder and some myopathies)
Ice Bag Test
- Bedside test for ptosis: improvement ≥2 mm after 2-min ice application = positive
- Sensitivity 0.94, specificity 0.97 - excellent for ocular MG at the bedside
- Now preferred over edrophonium due to better safety profile and availability
Edrophonium (Tensilon) Test
- Short-acting ChEI; positive in 60-95% of OMG and 72-95% GMG
- Largely fallen out of favour due to: widespread antibody testing, drug availability issues, and risk of bradycardia/bronchospasm; atropine must be available
Imaging
- CT thorax with contrast: mandatory in all newly diagnosed MG to screen for thymoma/mediastinal mass
Diagnostic Criteria Summary
Diagnosis is established by:
- Typical clinical pattern (fatigable weakness of characteristic distribution)
- Plus: elevated AChR or MuSK antibodies OR unequivocal response to ChEIs OR abnormal RNS/SFEMG
- Bradley and Daroff's Neurology, p. 2773-2776; Rosen's Emergency Medicine, p. 2261
6. Classification
MGFA (Myasthenia Gravis Foundation of America) Clinical Classification:
| Class | Description |
|---|---|
| I | Ocular muscle weakness only |
| IIa | Mild generalised weakness, predominantly limb/axial |
| IIb | Mild generalised weakness, predominantly bulbar/respiratory |
| IIIa | Moderate generalised weakness, predominantly limb/axial |
| IIIb | Moderate generalised, predominantly bulbar/respiratory |
| IVa | Severe generalised, predominantly limb/axial |
| IVb | Severe generalised, predominantly bulbar/respiratory |
| V | Intubated with/without mechanical ventilation |
7. Treatment
7a. Symptomatic: Cholinesterase Inhibitors
Pyridostigmine (Mestinon)
- First-line symptomatic treatment
- Inhibits acetylcholinesterase → increases ACh at synapse → improved NMT
- Starting dose: 30-60 mg every 4-6 hours (up to 120 mg per dose in severe cases)
- Maximum total daily dose generally 600 mg/day
- Side effects: muscarinic effects (diarrhoea, cramps, increased secretions, bradycardia); excess doses can paradoxically worsen weakness (cholinergic crisis - now rare)
- Caution: MuSK-MG patients may worsen with pyridostigmine
7b. Immunosuppression: Long-term Disease Modification
Corticosteroids
- Most rapid-onset immunosuppressant (weeks)
- Prednisolone 1-1.5 mg/kg/day (alternate-day dosing reduces side effects)
- Important pitfall: up to 50% of patients experience transient early worsening in the first 2-3 weeks of steroid initiation - start inpatient or with slow dose escalation in moderate-severe disease
- Long-term steroid-sparing agents are almost always needed
Azathioprine (AZA)
- First-line steroid-sparing agent; RCT evidence of efficacy
- Standard dose: 2-3 mg/kg/day
- Onset of benefit: 6-18 months - the key clinical limitation
- Check thiopurine methyltransferase (TPMT) status before initiating
- Monitor: full blood count, LFTs
- Side effects: myelosuppression, hepatotoxicity, increased lymphoma risk (long-term)
Mycophenolate Mofetil (MMF)
- Widely used despite lack of definitive RCT evidence (two RCTs failed to show benefit vs prednisolone alone)
- Dose: 1000-1500 mg twice daily
- Better tolerated than AZA
- Contraindicated in pregnancy (teratogenic - category D); two reliable contraceptive methods required; stop ≥4 months before planned conception
- Side effects: GI (diarrhoea, nausea), rare PML
Tacrolimus
- Calcineurin inhibitor; RCT evidence in MG; approved for MG in Japan
- Useful as steroid-sparing agent in AZA/MMF-intolerant patients or for rapid response
- Monitor: renal function, blood glucose (inhibits insulin), potassium, drug levels
- Drug interactions including grapefruit
Cyclosporine
- RCT evidence; reserved for refractory cases due to nephrotoxicity, hypertension, drug interactions
Cyclophosphamide
- For severe, refractory GMG after failure of standard therapy
- Pulsed IV (500 mg/m²) or high-dose (50 mg/kg × 4 days) regimens
- Significant toxicity: myelosuppression, haemorrhagic cystitis, infertility, malignancy
7c. Short-term Immunomodulation
Plasma Exchange (PLEX / Plasmapheresis)
- Removes circulating autoantibodies rapidly
- Effective in up to 95% of patients in acute myasthenic crisis
- Typically 5 exchanges over 1-2 weeks
- Onset of benefit: days
- Indications: myasthenic crisis, pre-operative preparation, bridge to IS therapy, or chronic treatment in refractory patients
- Limitations: IV access, cardiovascular stress, coagulopathy, need for anticoagulation
Intravenous Immunoglobulin (IVIg)
- Comparable efficacy to PLEX in acute exacerbations; practical alternative
- Dose: 1-2 g/kg over 2-5 days
- Onset: days to weeks
- Mainstay of ED crisis management alongside PLEX
- Side effects: headache, aseptic meningitis, thrombosis, haemolysis; contraindicated in IgA deficiency
7d. Targeted Biologics (Newer Therapies)
Rituximab (anti-CD20)
- Depletes B cells; especially effective in MuSK-MG (often dramatic response)
- Also used in refractory AChR-MG
- Cochrane review 2025 [PMID: 40607605]: systematic review of evidence
- Avoid in pregnancy (crosses placenta; haematological abnormalities in neonates)
Eculizumab (anti-C5 complement inhibitor)
- FDA/EMA approved for refractory generalised AChR-antibody positive MG
- Blocks terminal complement activation → prevents NMJ destruction
- Requires meningococcal vaccination ≥2 weeks before initiating
- Maintenance every 2 weeks IV; expensive
Ravulizumab
- Long-acting anti-C5; every-8-week dosing; FDA approved
FcRn Inhibitors (efgartigimod, rozanolixizumab, nipocalimab)
- Block the neonatal Fc receptor → increased IgG catabolism → rapid reduction in all IgG antibodies including AChR-abs
- Efgartigimod (Vyvgart): FDA approved 2021 for generalised AChR-positive MG
- Meta-analysis 2025 [PMID: 40288289]: confirmed efficacy and safety; rapid onset (1-2 weeks)
- Network meta-analysis 2025 [PMID: 40346603]: FcRn inhibitors and complement inhibitors showed superior efficacy vs standard immunosuppression in refractory GMG
7e. Thymectomy
- Mandatory for thymoma (regardless of MG severity)
- Recommended for non-thymomatous AChR-positive GMG in patients aged 18-65 years - the MGTX RCT (2016) demonstrated improved outcomes (less immunosuppression, better QMG scores) at 3 years after transsternal thymectomy vs medical therapy alone
- Less clear benefit in: MuSK-MG, OMG, elderly, seronegative MG
- Benefit is delayed (months to years post-surgery)
- Video-assisted thoracoscopic (VATS) or robotic approaches are standard
8. Myasthenic Crisis
Definition
Respiratory failure or severe bulbar compromise requiring mechanical ventilation or intubation. Occurs in ~20% of MG patients at some point.
Precipitants (Box - drugs that worsen MG)
| Category | Examples |
|---|---|
| Cardiovascular | Beta-blockers, calcium channel blockers, quinine, lidocaine, procainamide |
| Antibiotics | Aminoglycosides, fluoroquinolones, clindamycin, polymyxins, tetracyclines |
| Neurological | Phenytoin, neuromuscular blocking agents |
| Other | Corticosteroids (first 2-3 weeks), thyroid replacement, infection, surgery, pregnancy, aspiration |
Management
- Airway first: Respiratory failure is from muscle weakness, not hypoxaemia - supplemental O₂ alone is insufficient
- Monitor with capnometry (detects CO₂ retention early, before oximetry desaturation)
- BiPAP if airway can be protected; endotracheal intubation if not
- Indicators for intubation: FVC <15-20 mL/kg, NIF weaker than -20 to -25 cmH₂O
- PLEX or IVIg: mainstays of acute crisis management (comparable efficacy)
- Hold or reduce pyridostigmine during crisis (increased secretions worsen respiratory mechanics and risk aspiration)
- Identify and treat precipitant (infection, medication, aspiration)
- Immunosuppression: bridge to or intensify long-term IS
Cholinergic Crisis vs Myasthenic Crisis
| Feature | Myasthenic Crisis | Cholinergic Crisis |
|---|---|---|
| Cause | Insufficient drug/disease progression | Excess ChEI |
| Pupils | Normal/dilated | Miotic |
| Secretions | Normal | Increased (salivation, sweating, bronchospasm) |
| Muscle fasciculations | Absent | Present |
| Response to more pyridostigmine | Improves | Worsens |
9. Special Populations
Pregnancy
- Fertility unaffected; OCP does not worsen MG
- ~2/3 of patients report some worsening at some point during pregnancy or puerperium
- Greatest risk: first trimester and puerperium
- Safe drugs: pyridostigmine, prednisolone, azathioprine (with caution)
- Avoid: mycophenolate (teratogenic - category D), cyclophosphamide, rituximab
- Neonatal MG: transient in neonates from placental transfer of maternal antibodies; resolves over weeks
- Uterine smooth muscle is not affected (normal labour)
- Magnesium sulphate for pre-eclampsia is contraindicated (blocks NMJ)
Ocular MG
- 50% generalise within 2 years
- Pyridostigmine first-line; early immunotherapy with low-dose steroids may prevent generalisation
- Patients without generalisation by 2 years are unlikely to do so
Elderly
- Increasing demographic; often present late/atypically
- Higher rates of thymoma
- Greater vulnerability to steroid and immunosuppressant side effects
- Drug interactions more likely (renal/hepatic function)
Lambert-Eaton Myasthenic Syndrome (LEMS) - key differential
| MG | LEMS | |
|---|---|---|
| Antibody | Anti-AChR (or MuSK) | Anti-VGCC (P/Q type) |
| Site | Postsynaptic | Presynaptic |
| Reflexes | Normal | Reduced/absent (facilitated post-exercise) |
| Strength | Worse with use | Improves with brief use |
| Autonomic | No | Yes (dry mouth, erectile dysfunction) |
| Association | Thymoma | Small cell lung cancer (60%) |
| ChEI response | Good | Poor |
| RNS | Decrement | Increment at high frequency |
10. Outcome and Prognosis
- Most patients have normal life expectancy with modern treatment
- ~10% remain treatment-refractory
- Minimal manifestation status (MMS) or pharmacological remission is achievable in the majority
- Spontaneous remission occurs in ~10-20% (higher in prepubertal juvenile MG)
- Thymectomy in non-thymomatous GMG approximately doubles the rate of MMS at 3 years
Recent Evidence Updates (2024-2026)
- FcRn inhibitors (efgartigimod, rozanolixizumab, nipocalimab) have an established role in refractory GMG with rapid onset of action - network meta-analysis confirmed superiority over standard IST [PMID: 40346603]
- Rituximab Cochrane review (2025) confirms evidence for use, particularly in MuSK-MG [PMID: 40607605]
- FcRn inhibitor meta-analysis (2025) confirms class efficacy and safety [PMID: 40288289]
Primary sources: Bradley and Daroff's Neurology in Clinical Practice (9e); Robbins & Kumar Basic Pathology; Rosen's Emergency Medicine; Fishman's Pulmonary Diseases; Kandel's Principles of Neural Science; supplemented by PubMed systematic reviews 2024-2026.
This is a shared conversation. Sign in to Orris to start your own chat.