Topic is types of antigen and antibody reactions
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material from the textbooks. Let me compile the complete, well-structured answer.
Types of Antigen-Antibody (Ag-Ab) Reactions
Antigen-antibody reactions are the cornerstone of the adaptive immune response and the basis of almost all clinical immunological tests. These reactions are governed by non-covalent forces and are reversible.
I. Fundamental Nature of Ag-Ab Binding
The basic reaction is:
Ag + Ab ⇌ Ag-Ab Complex
The binding involves multiple weak non-covalent forces acting cooperatively:
- Hydrophobic bonds
- Hydrogen bonds
- Van der Waals forces
- Ionic (electrostatic) interactions
These forces only become effective when the antigen fits snugly into the complementary antigen-binding site (paratope) on the antibody.
Key Concepts: Affinity vs. Avidity
| Parameter | Definition | Notes |
|---|---|---|
| Affinity | Strength of binding at a single Ag-Ab combining site | Expressed as Ka (association constant) or Kd (dissociation constant) |
| Avidity | Total binding strength of all binding sites combined (functional affinity) | Relevant for multivalent antigens and antibodies like IgM |
-
High-affinity antibodies have Ka ~ 10^8-10 M^-1 (or Kd ~ 10^-8 to 10^-10 M = "nM binders")
-
IgG has 2 binding sites; IgM has 10 (pentamer), giving it far greater avidity despite moderate per-site affinity
-
An IgG molecule binds at least 10,000x more strongly to a multivalent antigen when both sites are engaged vs. only one
-
Roitt's Essential Immunology, p. 165-167; Henry's Clinical Diagnosis, p. 1027
II. Zones of Ag-Ab Reaction (Precipitin Curve)
When antigen is added in increasing amounts to a fixed quantity of antibody, three zones emerge:
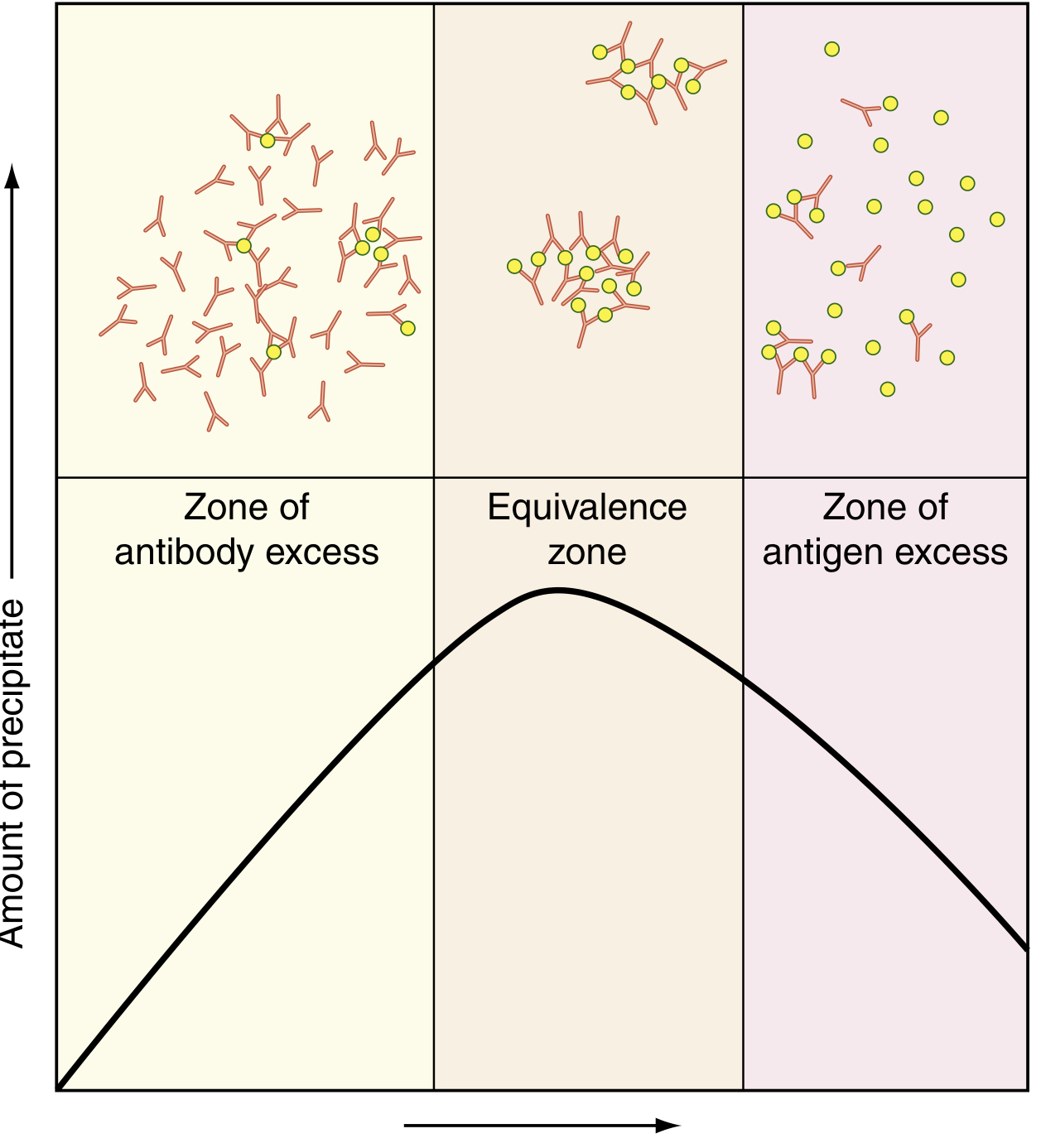
| Zone | Condition | Complex Formed | Precipitate |
|---|---|---|---|
| Zone of Antibody Excess (Prozone) | Excess Ab, few Ag | Small, soluble complexes | Little or none |
| Zone of Equivalence | Ag:Ab ratio optimal | Large, insoluble lattice | Maximum - visible precipitate |
| Zone of Antigen Excess (Postzone) | Excess Ag, few Ab | Small, soluble complexes | Little or none |
Clinical relevance - Prozone/Hook effect: In high-titer antibody states (e.g., syphilis), saturating all antibody sites prevents complex formation, giving a falsely negative result. Diluting the specimen restores positivity. - Henry's Clinical Diagnosis, p. 1088
III. Primary Types of Ag-Ab Reactions
1. Precipitation Reactions
Soluble antigen reacts with antibody to form an insoluble precipitate (lattice/network). Requires:
- Bivalent or multivalent antibody (cross-links antigens)
- Multivalent antigen (must have ≥2 identical determinants for lattice)
Subtypes:
| Method | Description | Use |
|---|---|---|
| Single immunodiffusion | Ag diffuses through Ab-containing gel | Qualitative |
| Double immunodiffusion (Ouchterlony) | Both Ag and Ab diffuse toward each other | Identify Ag-Ab identity/cross-reactivity |
| Immunoelectrophoresis | Electrophoresis + diffusion | Paraprotein analysis |
| Single radial immunodiffusion (Mancini) | Ag diffuses into Ab-gel; ring diameter ∝ Ag concentration | Quantitative Ig measurement |
| Rocket electrophoresis | Ag electrophoresed into Ab gel | Semiquantitative |
| Nephelometry/Turbidimetry | Light scattering by immune complexes | Highly sensitive, automated quantitation |
- Henry's Clinical Diagnosis, p. 1027
2. Agglutination Reactions
Particulate antigens (or particles coated with antigen/antibody) are cross-linked by antibody to form visible clumps (agglutinates). More sensitive than precipitation because the particle amplifies the reaction.
Subtypes:
| Type | Antigen Carrier | Examples |
|---|---|---|
| Direct agglutination | Bacteria or cells themselves | ABO blood typing, Widal test (typhoid) |
| Hemagglutination | Red blood cells | Blood grouping, crossmatching |
| Latex agglutination | Latex particles coated with Ag or Ab | Lancefield streptococcal typing, cryptococcal antigen in CSF |
| Indirect (passive) agglutination | Soluble Ag coated onto RBCs or latex | TPHA for syphilis |
| Hemagglutination Inhibition (HI) | Inhibition of viral HA by antibody | Influenza antibody titration, rubella serology |
| Reverse passive agglutination | Ab coated onto particles to detect Ag | Detecting bacterial antigens |
Key principle: Agglutination is caused by bivalent/multivalent antibody forming bridges between adjacent antigen-carrying particles - Henry's Clinical Diagnosis, p. 1087
3. Complement Fixation / Complement Activation
When antibody (IgG or IgM) binds its antigen, conformational changes in the Fc region expose C1q binding sites on the CH2 domain. This initiates the classical complement pathway:
- C1q binds → C1r and C1s activated
- C4 and C2 cleaved → C3 convertase (C4b2a) formed
- C3 cleaved → C3b (opsonin) + C3a (anaphylatoxin)
- C5 cleaved → C5b initiates MAC (membrane attack complex)
- MAC (C5b-9) lyses the target cell
Consequences:
- Opsonization (C3b coats pathogen → enhanced phagocytosis)
- Inflammation (C3a, C5a - anaphylatoxins/chemotaxis)
- Cytolysis (MAC)
Complement fixation tests use this principle diagnostically: if patient Ab + Ag fixes complement, there is none left to lyse indicator RBCs (positive test = no hemolysis). - Sherris & Ryan's Medical Microbiology, p. 73
4. Neutralization Reactions
Antibody physically blocks the biological activity of an antigen (toxin, virus) by binding to its active site or receptor-binding domain.
Subtypes:
| Target | Mechanism | Examples |
|---|---|---|
| Viral neutralization | Ab binds viral attachment protein → prevents cell entry | Influenza, HIV, SARS-CoV-2 neutralizing antibodies |
| Toxin neutralization | Ab occupies active site of toxin | Antitoxins to diphtheria, tetanus, botulinum toxins |
| Enzyme neutralization | Ab inhibits enzymatic activity | Anti-streptolysin O (ASO) test |
Neutralization of botulinum toxin illustrates synergy: no single mAb was protective in mice, but combinations of mAbs provided complete protection. This is the "bonus effect" of multivalent binding - Roitt's Essential Immunology, p. 167
5. Opsonization
Antibody (especially IgG) coats the surface of a pathogen. Phagocytes (macrophages, neutrophils) express Fc receptors (FcγR) that bind the Fc portion of surface-bound antibody, triggering enhanced phagocytosis.
- IgG + complement C3b together provide the most potent opsonization (via FcR + CR1 on phagocytes)
- CH3 domain of IgG mediates binding to macrophages, monocytes, and cytotoxic K cells (per the Biological Properties of Immunoglobulin Domains table) - Henry's Clinical Diagnosis, p. 1087
6. Antibody-Dependent Cellular Cytotoxicity (ADCC)
Antibody (IgG) coats target cells (e.g., virus-infected cells, tumor cells). NK cells and other effector cells bearing FcγRIII (CD16) bind via their Fc receptor and kill the Ab-coated target without MHC restriction.
7. Immune Complex Formation (Type III Hypersensitivity)
When large amounts of Ag-Ab complexes form and are not cleared efficiently (usually in antigen excess - small soluble complexes evade macrophages), they deposit in vessel walls, glomeruli, and synovium, triggering:
- Complement activation
- Neutrophil recruitment
- Tissue damage
Examples: Serum sickness, post-streptococcal glomerulonephritis, SLE. - Henry's Clinical Diagnosis, p. 1088
IV. Laboratory Methods to Detect Ag-Ab Reactions
| Method | Principle | Sensitivity |
|---|---|---|
| Precipitation (gel diffusion) | Lattice formation | Low (~0.1-0.5 mg/dL) |
| Agglutination | Particle cross-linking | Moderate (naked eye) |
| Complement fixation | Hemolytic indicator | Moderate |
| ELISA/EIA | Enzyme label; direct, indirect, sandwich | Very high |
| Immunofluorescence | FITC-labeled Ab, fluorescence microscopy | High |
| Radioimmunoassay (RIA) | Radioactive label | Very high |
| Surface Plasmon Resonance (SPR) | Optical changes on metal surface; measures Kon and Koff | Real-time kinetics |
| Nephelometry | Light scattering by immune complexes | High (automated) |
Equilibrium dialysis (historical): Semi-permeable membrane separates Ab from hapten; measures Kd by comparing concentrations at equilibrium. - Cellular and Molecular Immunology, p. 1587
V. Summary Table: Types of Ag-Ab Reactions
| Reaction Type | Antibody Class | Outcome | Clinical Relevance |
|---|---|---|---|
| Precipitation | IgG, IgM | Insoluble lattice | Immunodiffusion, nephelometry |
| Agglutination | IgM > IgG | Particle clumping | Blood typing, serology |
| Complement activation | IgG, IgM | Lysis, opsonization, inflammation | Killing of pathogens |
| Neutralization | IgG, IgA (mucosa) | Block toxin/virus activity | Vaccination, passive immunity |
| Opsonization | IgG (especially IgG1, IgG3) | Enhanced phagocytosis | Defense against encapsulated bacteria |
| ADCC | IgG | Target cell killing | Antiviral, antitumor |
| Immune complex deposition | IgG, IgA | Tissue inflammation | Autoimmunity, hypersensitivity |
Sources: Roitt's Essential Immunology; Henry's Clinical Diagnosis and Management by Laboratory Methods; Sherris & Ryan's Medical Microbiology; Cellular and Molecular Immunology (Janeway/Abbas)
This is a shared conversation. Sign in to Orris to start your own chat.