acess to abdominal aorta and inferiror vena cava
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive answer. Here it is:
Surgical Access to the Abdominal Aorta and Inferior Vena Cava
Anatomical Overview
The abdominal aorta begins at the aortic hiatus of the diaphragm at vertebra T12, descends anterior to the vertebral bodies (L1-L4), and bifurcates into the common iliac arteries just to the left of midline at L4 - roughly 2.5 cm below the umbilicus. The IVC forms at L5 (junction of common iliac veins, just to the right of midline) and ascends to the right of the aorta, exiting through the central tendon of the diaphragm at T8.
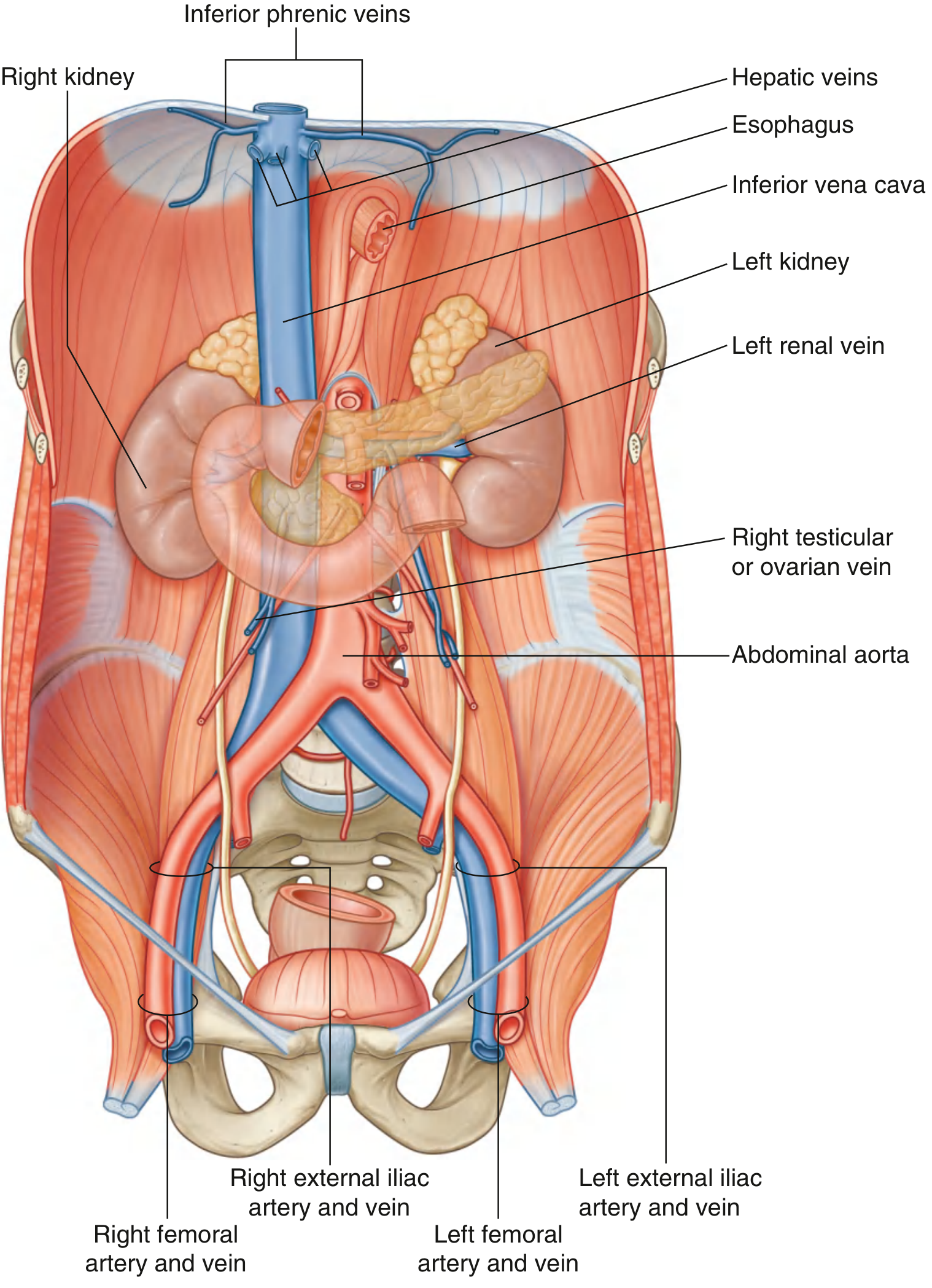
Fig. 4.169 - Gray's Anatomy for Students: Abdominal aorta and IVC with their relations and tributaries
Key Relations (Surgical Importance)
| Structure | Aorta | IVC |
|---|---|---|
| Anterior | Pancreas/splenic vein, left renal vein, 3rd part of duodenum | Right common iliac artery, root of mesentery, 3rd duodenum, pancreatic head, portal vein, liver |
| Right side | IVC, cisterna chyli, thoracic duct, azygos vein | - |
| Left side | Left crus of diaphragm | Aorta |
| Posterior | Lumbar veins (cross it), vertebral bodies | Vertebral column |
Surgical Approaches to the Abdominal Aorta
All approaches below are described in Maingot's Abdominal Operations.
1. Supraceliac Aortic Exposure (Most Expeditious)
This is the most important and versatile technique in abdominal vascular emergencies. The supraceliac aorta is generally free of aneurysmal/atherosclerotic disease, making clamping safer. Visceral ischemia must be limited to ≤45 minutes.
Steps:
- Divide the gastrohepatic ligament between clamps (Fig. 13-2A)
- Mobilize the left lobe of the liver by dividing its diaphragmatic attachments if needed
- Identify the aorta to the right of the esophagus (NGT/OGT helps distinguish them if unclear)
- Divide the left crus of the diaphragm completely - this is critical. Fibers are divided at the "2 o'clock" position slightly to the left of midline with scissors or cautery
- Identify and clip or spare the phrenic arteries
- Encircle the aorta between thumb and index finger, lift gently off the spine to confirm complete mobilization
- Apply a straight aortic clamp under direct vision
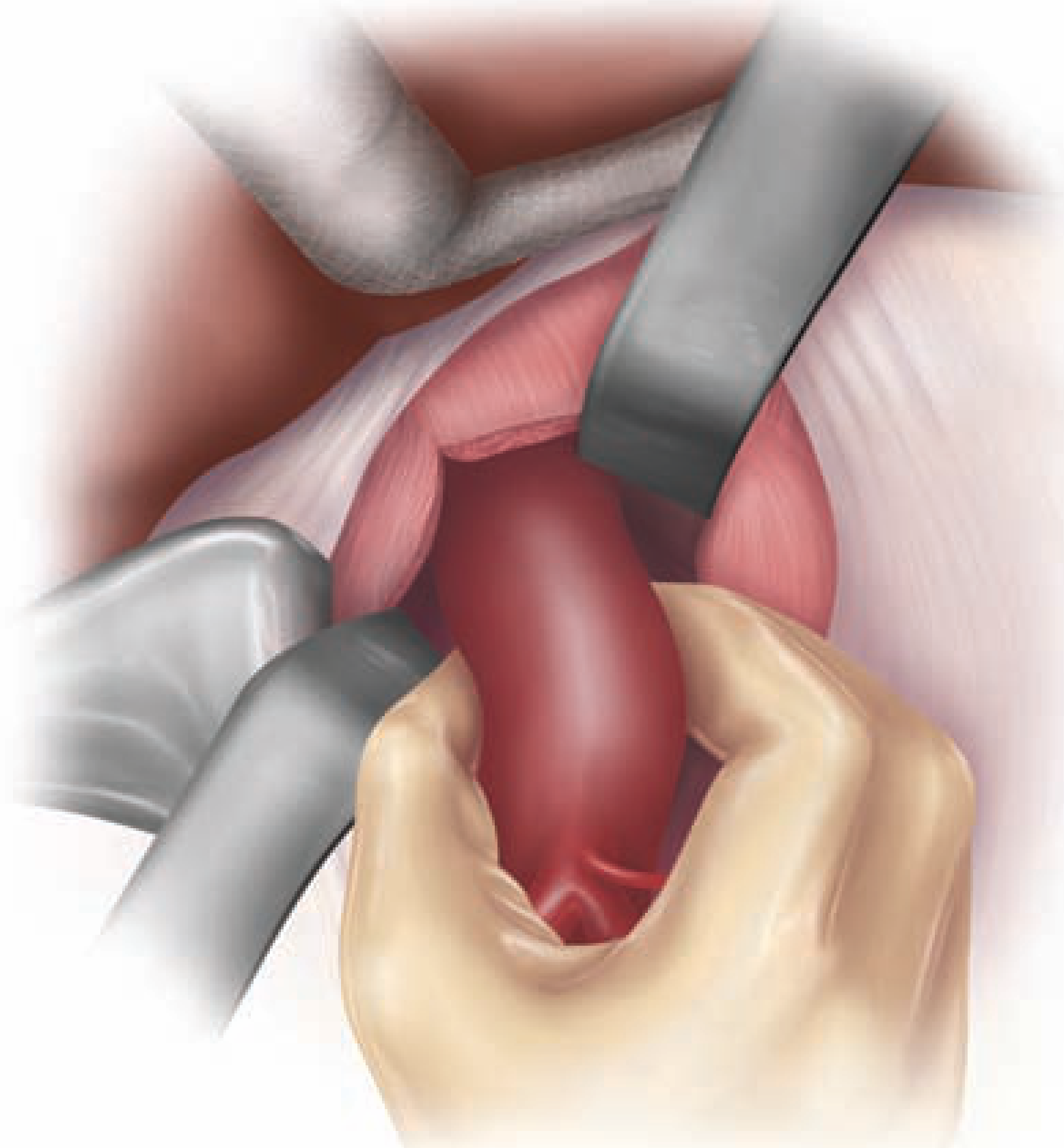
Fig. 13-2C - Maingot's: Aorta encircled bluntly using finger dissection after complete division of crural fibers
Pitfall: Incomplete division of crural fibers will cause any applied clamp to slip anteriorly - potentially catastrophic.
2. Infrarenal Aortic Exposure
The most commonly used approach for elective aortic surgery (AAA repair, aortoiliac reconstruction).
Steps:
- Incise the ligament of Treitz and mobilize the 4th part of the duodenum superiorly and to the right
- Divide the inferior mesenteric vein between clamps if it impairs exposure (risk of avulsion under tension)
- The left renal vein marks the superior extent of infrarenal dissection - it almost never requires division. If additional mobilization is needed, ligate gonadal and lumbar tributaries; divide adrenal vein if retracting IVC inferiorly
- Note: ~1% of patients have a retroaortic left renal vein - at risk during cross-clamping if unrecognized
- Cauterize or ligate lymphatics anterior to the aorta (large ones ligated to prevent chyle leak)
- Encircle the aorta digitally (thumb + index finger), raise it off the spine, and apply cross-clamp under direct vision
- A vessel loop/tape can be placed around the infrarenal aorta for additional control
3. Visceral Aortic Exposure
Rarely required for acute emergencies. Achieved via left medial visceral rotation (Mattox maneuver) - the left colon, spleen, pancreas tail, and stomach are rotated medially, exposing the entire left side of the aorta from the diaphragm to the bifurcation.
4. Iliac Artery Exposure
- Proximal common iliac: reflect small bowel mesentery to the right, expose the aortic bifurcation
- External iliac: mobilize right or left colon along Toldt's line, reflect toward midline
- Identify and protect the ureter as it crosses the iliac bifurcation
- Warning: The confluence of iliac veins lies directly behind the right common iliac artery - this is the most common site of iatrogenic vascular injury during aortoiliac surgery. Use blunt dissection to separate artery from vein.
Surgical Exposure of the IVC
The IVC is the most commonly injured vessel in penetrating abdominal trauma.
Approach - Right Medial Visceral Rotation:
- Mobilize the right colon (along the white line of Toldt)
- Perform an extended Kocher maneuver - rotate the duodenum and head of the pancreas medially for more proximal (suprarenal/retrohepatic) exposure
- This exposes the IVC and confluence of the iliac veins
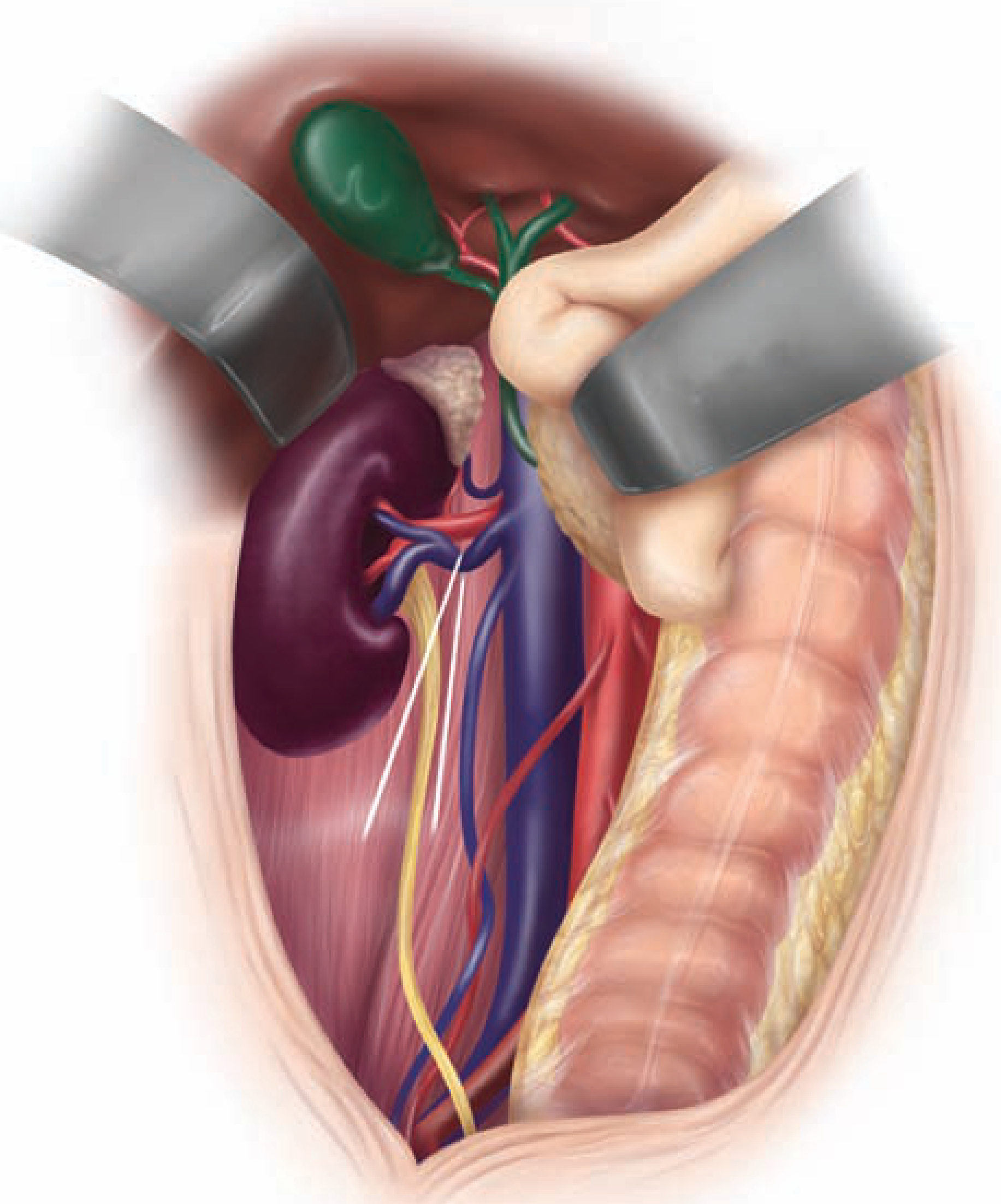
Fig. 13-7 - Maingot's: Right medial visceral rotation exposing IVC region (right colon reflected, ureter in yellow, IVC/aorta visible)
Key surgical principles for venous control:
- Avoid circumferential mobilization of the IVC whenever possible - posterior lumbar tributaries are fragile and easily torn
- Compression (sponge sticks) is the primary means of IVC hemorrhage control given its low-pressure nature
- Avoid vascular clamps where possible; use partial-occlusion clamps or Allis clamps for wound coaption
- Posterior IVC injuries require extensive mobilization and ligation of multiple lumbar tributaries
Proximal Arterial Control - Endovascular Options
In cases where open dissection is dangerous:
- Intra-aortic balloon occlusion from a remote access site (e.g., retrograde from femoral artery) can achieve proximal control
- The balloon must be buttressed against a rigid sheath to prevent migration from repetitive arterial pressure
- A Foley catheter balloon can control visceral back bleeding from collaterals (e.g., during ruptured aneurysm repair combined with supraceliac clamping)
- For routine/emergent cases, open exposure remains the fastest and most reliable method
Summary Table
| Level | Approach | Key Maneuver | Landmark |
|---|---|---|---|
| Supraceliac aorta | Transabdominal | Divide gastrohepatic lig + left crus | Esophagus (left), aorta (right) |
| Suprarenal aorta | Left medial visceral rotation | Mattox maneuver | Left renal vein inferiorly |
| Infrarenal aorta | Midline/retroperitoneal | Divide ligament of Treitz, mobilize 4th duodenum | Left renal vein (superior limit) |
| Iliac arteries | Retroperitoneal | Reflect colon along Toldt | Ureter at iliac bifurcation |
| IVC/iliac veins | Right medial visceral rotation | Extended Kocher maneuver | IVC right of aorta, fragile posterior tributaries |
Sources: Maingot's Abdominal Operations, Chapter 13 (Vascular Exposure and Control); Gray's Anatomy for Students, pp. 450-453
give short answer
Access to Abdominal Aorta and IVC
Abdominal Aorta
Incision: Midline laparotomy
Supraceliac Aorta
- Divide gastrohepatic ligament → enter lesser sac
- Divide left crus of diaphragm at "2 o'clock" position
- Encircle aorta by finger dissection → apply straight clamp
Infrarenal Aorta (most common)
- Divide ligament of Treitz → mobilize 4th part of duodenum upward and to the right
- Left renal vein = superior limit of dissection
- Encircle aorta digitally → apply cross-clamp
Inferior Vena Cava
Approach: Right medial visceral rotation
- Mobilize right colon along white line of Toldt
- Extended Kocher maneuver (reflect duodenum + pancreatic head medially) for proximal exposure
- IVC lies to the right of the aorta
Key principles:
- Avoid circumferential dissection (fragile posterior lumbar tributaries)
- Use compression (sponge sticks) as primary hemostatic method - low-pressure system
- Avoid clamps where possible; use partial-occlusion clamps only when needed
Danger zones: Iliac vein confluence lies behind the right common iliac artery - most common site of iatrogenic injury. Always identify and protect the ureter at the iliac bifurcation.
This is a shared conversation. Sign in to Orris to start your own chat.