Anatomy of angle and gonioscopic appearance for 20m
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Searching PubMed
gonioscopy anterior chamber angle
Anatomy of the anterior chamber angle and gonioscopic appearance (20-mark style)
1) Why gonioscopy is needed
The iridocorneal angle cannot be seen directly at slit lamp because of total internal reflection at the tear film-air interface. A goniolens (similar refractive index to cornea) eliminates this and allows angle visualization.
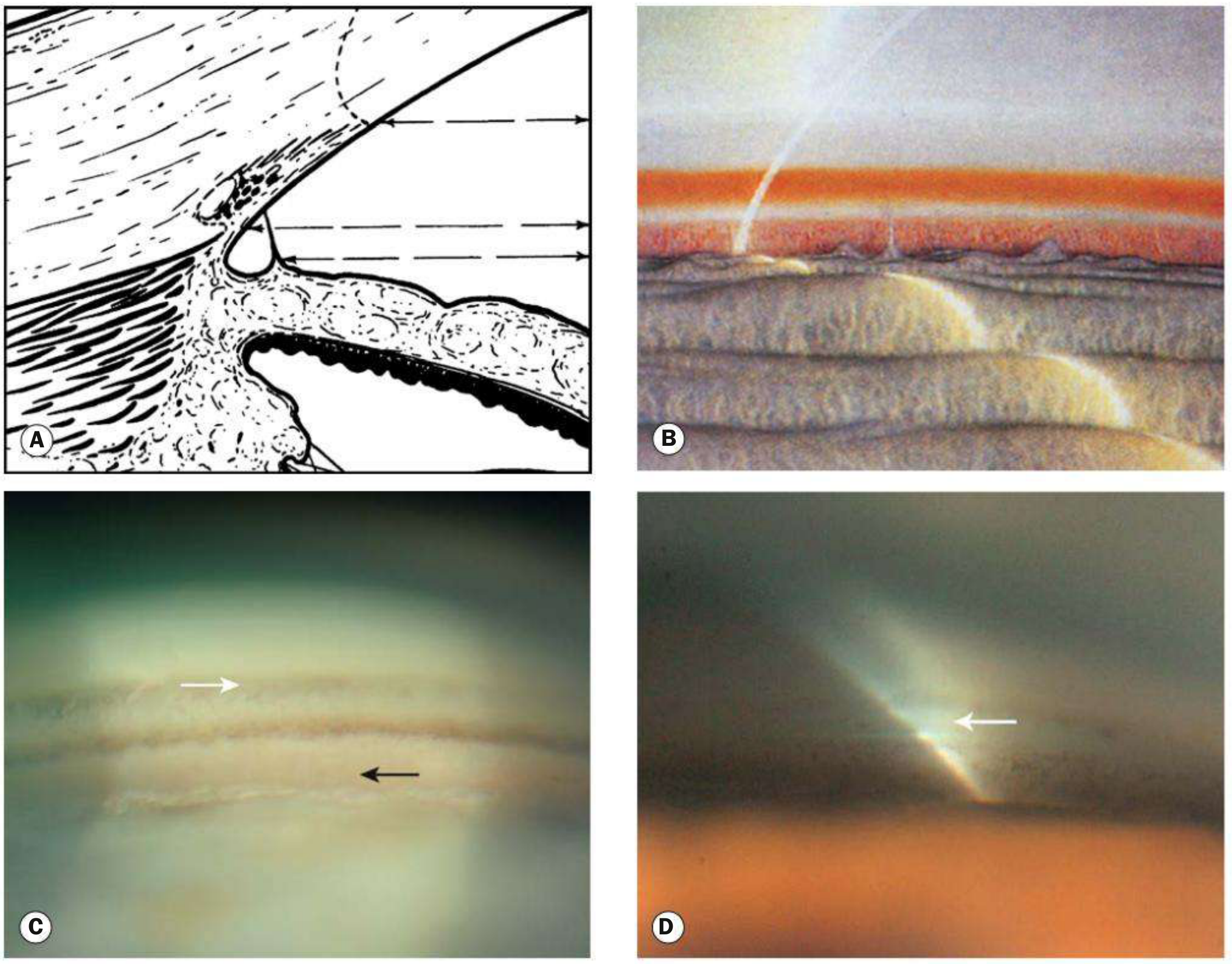
2) Angle anatomy in order (anterior to posterior) and how each looks on gonioscopy
-
Schwalbe line (SL)
- Most anterior landmark
- Appears as a thin whitish line, sometimes pigmented
- Can be highlighted with the corneal wedge technique
- Prominent pigment at/just anterior to SL is a Sampaolesi line
-
Trabecular meshwork (TM)
- From SL to scleral spur
- Anterior TM: pale, relatively nonfunctional
- Posterior TM: more pigmented, functional outflow portion
- Pigmentation generally increases with age, often greatest inferiorly
-
Schlemm canal
- Sometimes visible as a darker line deep to posterior TM
- Blood may be seen in canal physiologically or with raised episcleral venous pressure
-
Scleral spur (SS)
- White/yellow-white narrow band just posterior to TM
- Key landmark separating TM from ciliary body band
-
Ciliary body band (CBB)
- Dull brown/grey band posterior to SS
- Width varies with iris insertion/refractive status
- Often broader in myopes, narrower in hyperopes
-
Angle recess / iris root
- Posterior dip of peripheral iris insertion
- May be less visible in physiologically anterior insertion
3) Normal additional findings
- Iris processes: fine lacy strands from peripheral iris toward SS/CBB, common normal variant (especially young/brown irides)
- Radial vessels in angle recess can be normal
4) Abnormal gonioscopic findings (high yield)
- Peripheral anterior synechiae (PAS): broad adhesions of iris to angle structures; unlike fine iris processes
- Neovascularization of angle (NVA): abnormal vessels crossing SS onto TM
- Excessive pigmentation: pigment dispersion, pseudoexfoliation, prior inflammation/trauma
- Angle recession / cyclodialysis / trabecular dialysis in trauma
- Blood in Schlemm canal in venous congestion states
5) Methods of gonioscopy
- Indirect gonioscopy (most clinic use): mirror lenses at slit lamp (e.g., Goldmann/4-mirror)
- Direct gonioscopy: usually supine, often in OR (e.g., Koeppe), useful in infants/surgery
- Indentation (dynamic) gonioscopy:
- Distinguishes appositional closure (angle opens with indentation)
- From synechial closure (does not open)
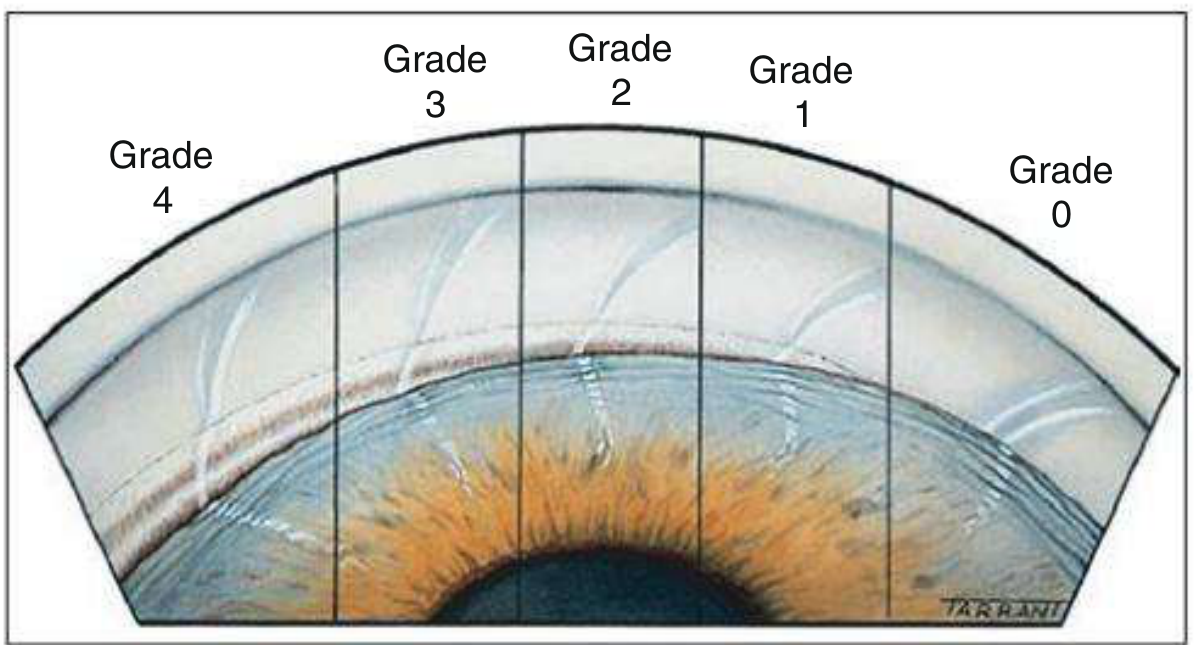
6) Grading of angle width (Shaffer)
- Grade 4 (35-45°): wide open, CBB visible
- Grade 3 (25-35°): open, SS visible
- Grade 2 (~20°): TM visible, SS not seen (narrower)
- Grade 1 (~10°): only SL ± upper TM visible, high closure risk
- Slit: no clear iridocorneal contact but no identifiable angle structures
- Grade 0 (0°): closed (iridocorneal contact)
Clinical point: document each quadrant separately; superior angle is often narrowest.
Key diagrams
Exam-ready short conclusion
Gonioscopy is the gold standard for anterior chamber angle assessment. A systematic approach identifies landmarks in sequence (SL, TM, SS, CBB, recess), assesses pigmentation and abnormal tissue/vessels, and grades width (commonly Shaffer). Dynamic gonioscopy is essential to differentiate appositional from synechial closure.
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., Ch. 1 and Ch. 11.
Can you refer becker shaffers and shields textbook
Yes. I can reference Becker-Shaffer’s Diagnosis and Therapy of the Glaucomas and Shields if they are available in this library.
If you want, I can now give the same 20-mark angle/gonioscopy answer rewritten specifically in Becker-Shaffer/Shields style with textbook-based citations.
Yes
Anatomy of angle and gonioscopic appearance (20 marks)
(Structured in Becker-Shaffer/Shields exam style)
1. Introduction
Gonioscopy is the clinical method to evaluate the anterior chamber angle, which cannot be directly visualized because of total internal reflection at the cornea-air interface. It is essential for classification and management of glaucoma.
2. Applied anatomy of the angle (anterior to posterior)
-
Schwalbe’s line
- Peripheral termination of Descemet membrane
- Most anterior gonioscopic landmark
- Appears as a thin glistening line, sometimes pigmented
- Pigment anterior to it may form a Sampaolesi line
-
Trabecular meshwork
- Extends from Schwalbe’s line to scleral spur
- Anterior non-pigmented TM: less functional
- Posterior pigmented TM: principal aqueous outflow zone, usually more pigmented
-
Schlemm’s canal
- External to juxtacanalicular trabeculum
- May appear as a dark line; occasional blood reflux may be seen
-
Scleral spur
- White band posterior to TM
- Important landmark separating TM from ciliary body band
-
Ciliary body band
- Brown/gray band posterior to scleral spur
- Width depends on iris insertion and ciliary body position
-
Angle recess and iris root
- Deepest posterior part where peripheral iris inserts
3. Normal gonioscopic appearance
- Open angle shows sequential visibility of landmarks from Schwalbe line to ciliary body band
- Physiologic trabecular pigmentation increases with age and is often maximal inferiorly
- Iris processes: fine lacy strands from iris root to trabeculum/scleral spur, normal variant
- Fine radial vessels at iris root may be normal
4. Technique points (high-yield)
- Perform in dim illumination with narrow slit beam to avoid artificial angle widening
- Use minimal lens pressure during static assessment
- Examine all 4 quadrants
- Use corneal wedge to identify Schwalbe line
- Indentation gonioscopy differentiates:
- Appositional closure: opens with indentation
- Synechial closure (PAS): does not open
5. Grading of angle width (Shaffer)
- Grade 4 (35-45°): wide open, closure impossible
- Grade 3 (25-35°): open, closure unlikely
- Grade 2 (~20°): narrow, closure possible
- Grade 1 (~10°): very narrow, closure probable
- Grade 0 (0°): closed
(Also mention Scheie and Spaeth systems in long answers; Shaffer is most commonly used for quick clinical grading.)
6. Abnormal gonioscopic findings
-
Peripheral anterior synechiae (PAS)
Broad iris adhesions to angle structures, unlike fine iris processes -
Increased trabecular pigmentation
Pigment dispersion syndrome, pseudoexfoliation, post-inflammatory causes -
Neovascularization of angle (NVA)
Abnormal vessels crossing scleral spur onto trabeculum, may progress to synechial closure -
Angle recession/traumatic signs
Widened ciliary body band, irregular angle after blunt trauma -
Blood in Schlemm canal
Seen with raised episcleral venous pressure or vascular anomalies
7. Clinical relevance
Gonioscopy determines whether glaucoma is open-angle, angle-closure, or secondary; guides laser peripheral iridotomy decisions; and is mandatory before angle procedures (trabeculoplasty, MIGS, goniotomy).
8. Conclusion
A systematic gonioscopic examination requires precise recognition of angle landmarks, correct grading, and identification of pathologic changes. Mastery of these features is fundamental in glaucoma diagnosis and treatment planning.
If you want, I can format this into a 1-page viva sheet (rapid recall) and a full 20-mark theory answer version side by side.
This is a shared conversation. Sign in to Orris to start your own chat.