Antimicrobials classification with mechanism of actions and drug interactions
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I have extensive, authoritative content. Now I'll compile the comprehensive answer.
Antimicrobials: Classification, Mechanisms of Action, and Drug Interactions
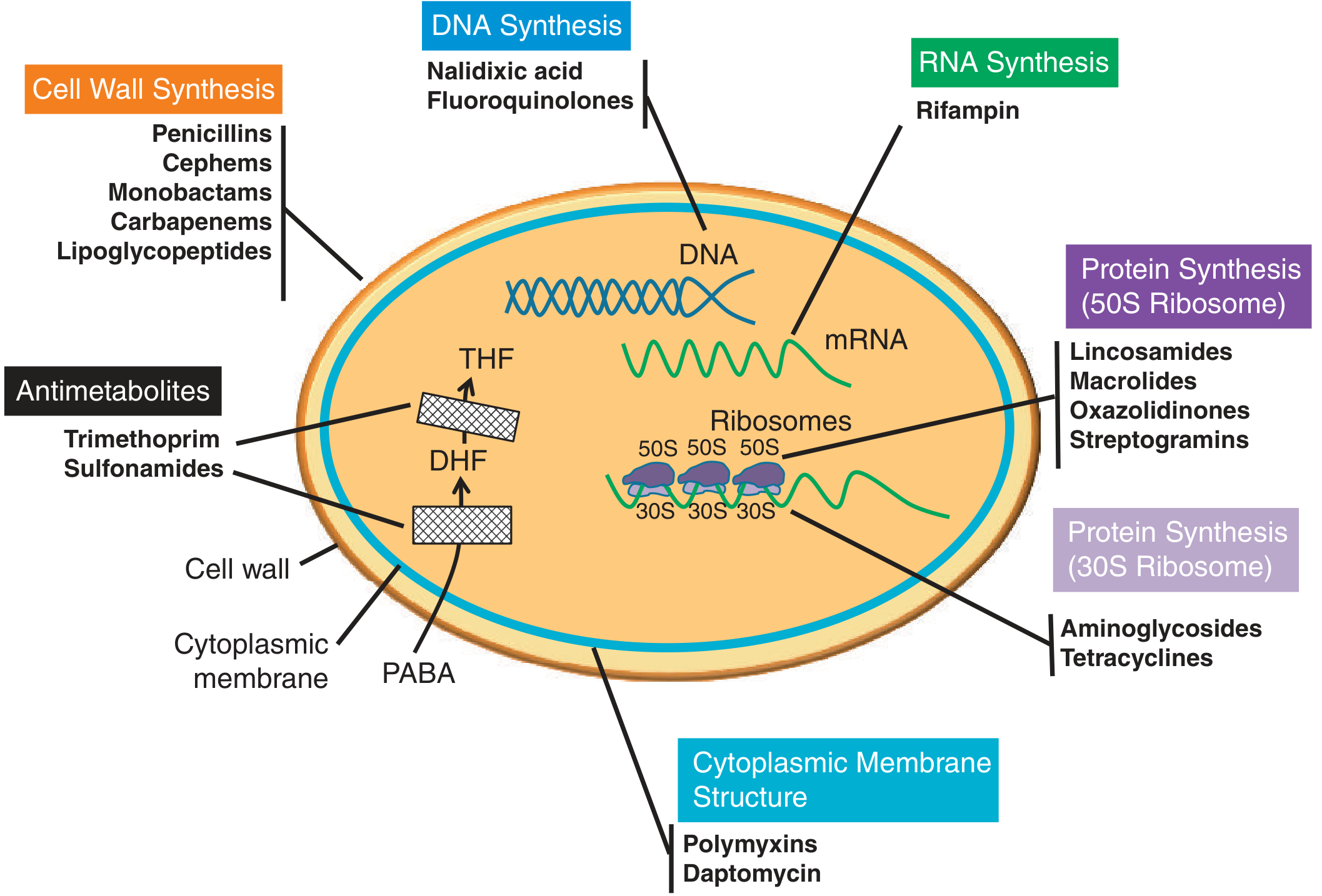
Figure 85.1 - Mode of action for commonly used antimicrobials (Tietz Textbook of Laboratory Medicine, 7th Ed.)
Antimicrobials can be classified by: (1) chemical structure (e.g., beta-lactams, aminoglycosides), (2) mechanism of action (e.g., cell wall synthesis inhibitors), or (3) target organism type (antibacterial, antifungal, antiviral). The mechanism-of-action framework is the most clinically useful and is organized below.
1. Cell Wall Synthesis Inhibitors
Peptidoglycan is the major structural component of the bacterial cell wall - a rigid mesh of disaccharide chains (N-acetylglucosamine and N-acetylmuramic acid) cross-linked by pentapeptide bridges via penicillin-binding proteins (PBPs).
A. Beta-Lactams
Drugs: Penicillins, Cephalosporins (1st-5th gen), Carbapenems, Monobactams (aztreonam)
Mechanism: The beta-lactam ring is structurally similar to pentapeptides, so PBPs mistakenly incorporate it into the cell wall. The drug then irreversibly inhibits transpeptidation (cross-linking of glycan strands), reducing cell wall rigidity and leading to autolysis. This accounts for their bactericidal activity.
Resistance: (1) Beta-lactamase production - enzymes that degrade the ring; (2) Altered PBP binding site (e.g., MRSA via mecA gene); (3) Reduced outer-membrane permeability (gram-negatives only). When these occur together (efflux + porin loss + beta-lactamase), the result is high-level resistance.
Beta-lactam/beta-lactamase inhibitor combinations: Clavulanate, sulbactam, tazobactam, avibactam, vaborbactam, relebactam are combined with penicillins or carbapenems. The inhibitor binds and inactivates beta-lactamase, restoring activity of the beta-lactam partner.
Drug interactions:
- Probenecid blocks tubular secretion of penicillins and cephalosporins, raising serum levels (sometimes exploited therapeutically)
- Aminoglycosides can be inactivated if mixed in the same IV bag with penicillins (physical incompatibility)
- Warfarin: Some cephalosporins (especially those with an N-methylthiotetrazole side chain like cefoperazone, cefamandole) inhibit vitamin K metabolism, potentiating anticoagulant effect
- Oral contraceptives: Broad-spectrum penicillins may reduce enterohepatic recirculation of estrogen (clinical significance debated)
- Methotrexate: Penicillins reduce renal excretion of methotrexate, raising toxicity risk
Subclasses:
| Subclass | Examples | Spectrum |
|---|---|---|
| Penicillinase-labile penicillins | Penicillin G/V, Ampicillin | Gram-positive, some gram-negative |
| Penicillinase-stable penicillins | Oxacillin, Nafcillin, Methicillin | MSSA, staph |
| Beta-lactam/beta-lactamase inhibitors | Amoxicillin-clavulanate, Pip-tazo, Ceftazidime-avibactam | Broad (including many resistant strains) |
| Cephalosporins 1st gen | Cefazolin, Cephalexin | Gram-positive |
| Cephalosporins 3rd gen | Ceftriaxone, Cefotaxime | Broad, gram-negative |
| Cephalosporins 4th gen | Cefepime | Broad, including Pseudomonas |
| Cephalosporins 5th gen (anti-MRSA) | Ceftaroline | Includes MRSA |
| Carbapenems | Imipenem, Meropenem, Ertapenem | Broadest bacterial coverage |
| Monobactams | Aztreonam | Aerobic gram-negatives only |
B. Glycopeptides / Lipoglycopeptides
Drugs: Vancomycin (glycopeptide); Dalbavancin, Oritavancin, Telavancin (lipoglycopeptides)
Mechanism: Large molecules that bind the D-Ala-D-Ala terminus of the peptidoglycan pentapeptide cross-bridge, blocking the substrate for the transpeptidase (rather than the enzyme itself as beta-lactams do). This prevents cross-linking, compromises structural integrity, and causes cell lysis. Lipoglycopeptides additionally depolarize the cell membrane due to their lipophilic side chain. Active against gram-positive bacteria (including anaerobes).
Resistance:
- Alteration of the D-Ala-D-Ala terminus to D-Ala-D-Lac or D-Ala-D-Ser (encoded by van genes - VRE mechanism)
- Cell wall thickening limiting access to target pentapeptides (vancomycin-intermediate Staphylococcus aureus, VISA)
Drug interactions:
- Aminoglycosides + vancomycin: Synergistic nephrotoxicity and ototoxicity - TDM required
- NSAIDs, loop diuretics (furosemide): Increased risk of nephrotoxicity and ototoxicity
- Neuromuscular blocking agents: Vancomycin may potentiate blockade
2. Cytoplasmic Membrane Disruptors
A. Lipopeptides
Drugs: Daptomycin, Polymyxins B and E (colistin)
Daptomycin: Anionic molecule that interacts with calcium to become positively charged, then inserts into the gram-positive cytoplasmic membrane, causing depolarization and rapid bactericidal cell death. Used for MRSA and VRE. Resistance is associated with cell envelope charge modifications, often correlating with prior vancomycin exposure.
Polymyxins: Positively charged molecules that bind LPS in the outer membrane of aerobic gram-negative bacteria, disrupting the membrane. Used as last-resort agents for multidrug-resistant gram-negatives (e.g., carbapenem-resistant Acinetobacter, Pseudomonas). Resistance is low overall; the plasmid-mediated mcr-1 gene (LPS modification) is a major emerging concern.
Drug interactions:
- Daptomycin + statins: Risk of myopathy/rhabdomyolysis - statins should be held
- Daptomycin + fibrates: Potential muscle toxicity
- Polymyxins + aminoglycosides: Additive nephrotoxicity
- Polymyxins + neuromuscular blocking drugs: May potentiate blockade
3. Protein Synthesis Inhibitors - 30S Ribosome
A. Aminoglycosides
Drugs: Gentamicin, Tobramycin, Amikacin, Streptomycin, Neomycin
Mechanism: Irreversibly bind the 30S ribosomal subunit and interfere with translation and translocation, halting protein synthesis. Primarily bactericidal against aerobic gram-negative bacteria; used in combination with cell wall agents for gram-positives (e.g., enterococcal endocarditis).
Resistance: (1) Ribosomal target mutation (mainly affects streptomycin); (2) Decreased membrane permeability (mainly in Pseudomonas); (3) Aminoglycoside-modifying enzymes on transposons/plasmids - acetyltransferases (AAC), adenyltransferases (ANT), phosphotransferases (APH).
Drug interactions:
- Vancomycin / loop diuretics (furosemide, ethacrynic acid): Potentiated nephrotoxicity and ototoxicity
- Neuromuscular blocking agents: Potentiation of neuromuscular blockade
- Amphotericin B: Additive nephrotoxicity
- NSAIDs: May reduce renal clearance, raising serum concentrations
- Penicillins (same IV bag): Chemical inactivation (physical incompatibility)
B. Tetracyclines
Drugs: Tetracycline, Doxycycline, Minocycline, Tigecycline (glycylcycline)
Mechanism: Reversibly bind the 30S ribosomal subunit, blocking the binding of aminoacyl-tRNA to the A site of the ribosome. Bacteriostatic. Broad spectrum including atypicals (Chlamydia, Mycoplasma, Rickettsia), some protozoa.
Resistance: Efflux pumps, ribosomal protection proteins. Tigecycline is a substrate for fewer efflux pumps.
Drug interactions:
- Divalent/trivalent cations (Ca²⁺, Mg²⁺, Al³⁺, Fe²⁺): Antacids, dairy, iron supplements chelate tetracyclines, drastically reducing oral absorption - must separate by 2 hours
- Warfarin: Tetracyclines may enhance anticoagulant effect (reduced vitamin K-producing gut flora)
- Oral contraceptives: May reduce efficacy (limited evidence)
- Isotretinoin: Combined with tetracyclines markedly raises risk of benign intracranial hypertension (pseudotumor cerebri) - contraindicated
- Methoxyflurane: Life-threatening nephrotoxicity reported
4. Protein Synthesis Inhibitors - 50S Ribosome
A. Macrolides
Drugs: Erythromycin, Clarithromycin, Azithromycin
Mechanism: Bind the 23S rRNA of the 50S ribosomal subunit, blocking translocation of peptidyl-tRNA (peptide elongation arrest). Bacteriostatic (bactericidal at high concentrations). Cover gram-positives, atypicals, H. influenzae.
Resistance: Methylation of 23S rRNA (erm genes, MLSB resistance), efflux pumps (mef genes).
Drug interactions:
- CYP3A4 inhibition (erythromycin > clarithromycin >> azithromycin): Raise levels of: statins (rhabdomyolysis risk), warfarin, cyclosporine, tacrolimus, benzodiazepines, carbamazepine, colchicine
- QT prolongation: Additive risk with antiarrhythmics (amiodarone, sotalol, quinidine), antipsychotics, methadone, fluoroquinolones - potentially fatal torsades de pointes
- Digoxin: Macrolides alter gut flora that metabolize digoxin, raising digoxin levels (toxicity risk)
- Terfenadine/Cisapride: Life-threatening cardiac arrhythmias (historic; these drugs withdrawn)
B. Lincosamides
Drugs: Clindamycin, Lincomycin
Mechanism: Bind to the 23S rRNA of the 50S subunit, inhibiting transpeptidation and the initial elongation phase. Bacteriostatic against aerobic/anaerobic gram-positive bacteria. Gram-negatives are intrinsically resistant (poor outer membrane permeability).
Resistance: Methylation of 23S rRNA by erm genes (same mechanism as macrolide MLSB resistance - hence cross-resistance). Inducible clindamycin resistance in MRSA detected by the D-zone test.
Drug interactions:
- Neuromuscular blocking agents: Clindamycin potentiates neuromuscular blockade
- Kaolin-pectin: Reduced oral absorption
- Erythromycin: Pharmacodynamic antagonism (compete for the same ribosomal binding site - avoid combining)
C. Oxazolidinones
Drugs: Linezolid, Tedizolid
Mechanism: Bind the 23S rRNA of the 50S subunit at the P site, preventing formation of the 70S initiation complex. Unique mechanism not shared by other antibiotic classes, so no cross-resistance. Used for MRSA, VRE, drug-resistant TB. Bacteriostatic against most organisms.
Drug interactions:
- MAO inhibition: Linezolid is a non-selective MAO inhibitor - major risk of serotonin syndrome with SSRIs, SNRIs, TCAs, meperidine, tramadol, triptans; also hypertensive crisis with tyramine-rich foods
- Adrenergic agents (dopamine, norepinephrine): Enhanced pressor response due to MAO inhibition
- Myelosuppression: Additive bone marrow suppression with other myelosuppressive agents
D. Streptogramins
Drugs: Quinupristin-dalfopristin (Synercid)
Mechanism: Dalfopristin binds the 50S subunit, blocking elongation; quinupristin binds adjacent to the dalfopristin site and prevents translocation. Together they are synergistic and bactericidal against most organisms (bacteriostatic against Enterococcus faecium).
Drug interactions:
- CYP3A4 inhibition: Raises levels of cyclosporine, tacrolimus, statins, calcium channel blockers, midazolam
E. Chloramphenicol
Mechanism: Binds 50S subunit, inhibiting the peptidyl transferase reaction. Broad spectrum, bacteriostatic.
Drug interactions:
- Warfarin, phenytoin, tolbutamide: Chloramphenicol inhibits CYP2C9 - raises levels of all three (toxicity)
- Bone marrow suppressants: Additive aplastic anemia risk
- Phenobarbital, rifampin: Induce chloramphenicol metabolism, reducing levels
5. DNA/Nucleic Acid Synthesis Inhibitors
A. Fluoroquinolones
Drugs: 1st gen: Nalidixic acid; 2nd gen: Ciprofloxacin, Norfloxacin; 3rd gen: Levofloxacin; 4th gen: Moxifloxacin, Gatifloxacin
Mechanism: Inhibit DNA gyrase (topoisomerase II) and topoisomerase IV, enzymes required for maintaining chromosomal supercoiling, DNA strand breakage, and rejoining during replication. This arrests synthesis and leads to bactericidal cell death.
- Gram-negatives: primarily target DNA gyrase
- Gram-positives: primarily target topoisomerase IV
- Moxifloxacin/higher generations also cover anaerobes and have enhanced gram-positive activity
Resistance: Target site mutations (gyrA, parC), upregulation of efflux pumps, plasmid-mediated resistance genes (qnr - protect topoisomerase from inhibition).
Drug interactions:
- Divalent/trivalent cations (antacids, Ca²⁺, Mg²⁺, Fe²⁺, zinc): Chelation - reduces oral absorption by 50-90%; separate by 2-4 hours
- Warfarin: Fluoroquinolones inhibit CYP1A2 (ciprofloxacin) or CYP3A4, raising warfarin levels; also kill gut flora that produce vitamin K - enhanced anticoagulation
- QT prolongation: Additive with macrolides, antiarrhythmics, antipsychotics - risk of torsades de pointes
- NSAIDs: Combined use may lower seizure threshold (antagonism of GABA-A receptors)
- Theophylline: Ciprofloxacin significantly inhibits CYP1A2 - raises theophylline levels (seizures, arrhythmias)
- Antidiabetics: Fluoroquinolones cause dysglycemia (gatifloxacin most implicated) - both hypoglycemia and hyperglycemia
- Corticosteroids: Increased risk of tendon rupture (already a fluoroquinolone class effect)
B. Nitroimidazoles
Drugs: Metronidazole, Tinidazole
Mechanism: Once inside anaerobic bacteria (or protozoa), the nitro group is reduced to a toxic compound that inhibits DNA synthesis and causes strand breakage, leading to cell death. Only active in low-oxygen/anaerobic environments. Bactericidal.
Resistance: Decreased uptake, altered reduction efficiency, nim genes converting the drug to a non-toxic by-product.
Drug interactions:
- Alcohol / Disulfiram-like reaction: Metronidazole inhibits aldehyde dehydrogenase - combining with alcohol causes flushing, nausea, vomiting, tachycardia (avoid alcohol during treatment and 48 h after)
- Warfarin: Inhibits CYP2C9, markedly potentiating anticoagulation - INR must be monitored closely
- Lithium: Metronidazole can reduce renal clearance of lithium (toxicity)
- Phenytoin: Metronidazole inhibits its metabolism, raising phenytoin levels
- Disulfiram: Combined use can cause psychosis/confusion
C. Rifamycins
Drugs: Rifampin (rifampicin), Rifabutin, Rifaximin, Rifapentine
Mechanism: Inhibit DNA-dependent RNA polymerase (binds the beta-subunit encoded by rpoB), thereby blocking bacterial transcription. Must always be used in combination because resistance (via rpoB mutation) emerges rapidly during monotherapy.
Drug interactions (rifampin is one of the most potent CYP inducers known):
- Potent CYP3A4/2C9/2C19/1A2 inducer + P-glycoprotein inducer: Dramatically lowers plasma levels of: warfarin, oral contraceptives (contraceptive failure), protease inhibitors (HIV), NNRTIs, cyclosporine, tacrolimus, digoxin, statins, voriconazole, methadone, benzodiazepines, steroids, sulfonylureas
- Isoniazid + rifampin: Combined use increases risk of hepatotoxicity above that of either drug alone
- Azole antifungals: Rifampin reduces azole levels dramatically (therapeutic failure)
6. Antimetabolites (Folate Synthesis Inhibitors)
A. Sulfonamides
Drugs: Sulfamethoxazole, Sulfadiazine, Sulfasalazine, Dapsone
Mechanism: Structural analogues of para-aminobenzoic acid (PABA). They competitively inhibit dihydropteroate synthase, the enzyme that incorporates PABA into dihydrofolic acid (DHF). Bacteria cannot use exogenous folate and must synthesize it de novo, so this blocks their folate production. Bacteriostatic.
B. Trimethoprim / TMP-SMX (Co-trimoxazole)
Drugs: Trimethoprim alone; Trimethoprim-sulfamethoxazole (TMP-SMX, Co-trimoxazole)
Mechanism: Trimethoprim inhibits dihydrofolate reductase (DHFR), the enzyme that reduces DHF to tetrahydrofolic acid (THF). The combination TMP-SMX produces sequential blockade of the folate pathway - sulfonamide blocks step 1 (PABA → DHF), trimethoprim blocks step 2 (DHF → THF). This sequential blockade is synergistic and effectively bactericidal.
Drug interactions:
- Warfarin: TMP-SMX inhibits CYP2C9 and displaces warfarin from protein binding - significantly raises INR
- Methotrexate: Both compete for the same enzyme (DHFR) - additive antifolate toxicity (bone marrow suppression, megaloblastic anemia)
- Phenytoin: TMP-SMX inhibits CYP2C9, raising phenytoin levels
- ACE inhibitors / potassium-sparing diuretics: Trimethoprim blocks distal tubular potassium secretion (like amiloride) - risk of hyperkalemia, especially with enalapril, spironolactone
- Cyclosporine: TMP-SMX may raise nephrotoxicity risk
- Dofetilide: Trimethoprim raises dofetilide levels (severe arrhythmia risk - contraindicated)
- Oral hypoglycemics (sulfonylureas): Sulfonamides potentiate hypoglycemic effect
Summary Table: Classification by Mechanism
| Mechanism | Drug Classes | Key Drugs |
|---|---|---|
| Cell wall synthesis | Beta-lactams, Glycopeptides, Lipoglycopeptides | Penicillins, Cephalosporins, Carbapenems, Vancomycin |
| Cell membrane disruption | Lipopeptides, Polymyxins | Daptomycin, Colistin |
| 30S ribosome inhibition | Aminoglycosides, Tetracyclines | Gentamicin, Doxycycline |
| 50S ribosome inhibition | Macrolides, Lincosamides, Oxazolidinones, Streptogramins, Chloramphenicol | Azithromycin, Clindamycin, Linezolid |
| DNA synthesis | Fluoroquinolones, Nitroimidazoles | Ciprofloxacin, Metronidazole |
| RNA synthesis | Rifamycins | Rifampin |
| Folate synthesis | Sulfonamides, DHFR inhibitors | TMP-SMX |
Key Drug Interaction Categories (Quick Reference)
| Interaction Type | Drugs | Risk |
|---|---|---|
| QT prolongation | Macrolides + Fluoroquinolones + antipsychotics | Torsades de pointes |
| Nephro/ototoxicity | Aminoglycosides + Vancomycin + loop diuretics | Kidney/hearing damage |
| CYP3A4 inhibition | Erythromycin, Clarithromycin, Quinupristin | Raised statin/cyclosporine levels |
| CYP3A4 induction | Rifampin | Reduced levels of most drugs |
| MAO inhibition | Linezolid + SSRIs/SNRIs | Serotonin syndrome |
| Chelation | Fluoroquinolones + Tetracyclines + antacids/iron | Reduced absorption |
| Disulfiram-like | Metronidazole + alcohol | Flushing, nausea |
| Hyperkalemia | TMP + ACE inhibitors/K-sparing diuretics | Life-threatening K⁺ rise |
| Anticoagulation | Metronidazole, TMP-SMX, fluoroquinolones + warfarin | Bleeding |
| Neuromuscular blockade | Aminoglycosides, Clindamycin, Polymyxins + NMBAs | Prolonged paralysis |
Sources: Tietz Textbook of Laboratory Medicine, 7th Ed., Chapter 85; Lippincott Illustrated Reviews: Pharmacology, Chapter 28; Goodman & Gilman's The Pharmacological Basis of Therapeutics, Chapter 5
This is a shared conversation. Sign in to Orris to start your own chat.