Thyroid 101
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have a comprehensive picture from multiple authoritative textbooks. Let me compile the full Thyroid 101 overview.
Thyroid 101 - A Complete Overview
1. Anatomy
The thyroid gland is a butterfly-shaped endocrine organ that sits in the anterior neck, just inferior to the larynx and straddling the trachea. It has two lobes connected by a narrow isthmus. Key anatomical points:
- Weight: ~20-30 g in an adult
- Blood supply: highly vascular - blood flow is approximately 5x the gland's weight per minute, comparable only to the adrenal cortex
- Microscopic structure: thousands of closed follicles (100-300 micrometers in diameter) filled with colloid and lined by cuboidal follicular (thyrocyte) epithelium
- Colloid contains thyroglobulin (Tg), the major secretory glycoprotein and hormone precursor
- C cells (parafollicular cells) scattered between follicles - they secrete calcitonin, which regulates plasma calcium
Guyton and Hall Textbook of Medical Physiology
2. Hormone Synthesis - Step by Step
The HPT axis (Hypothalamus - Pituitary - Thyroid) controls the whole process:
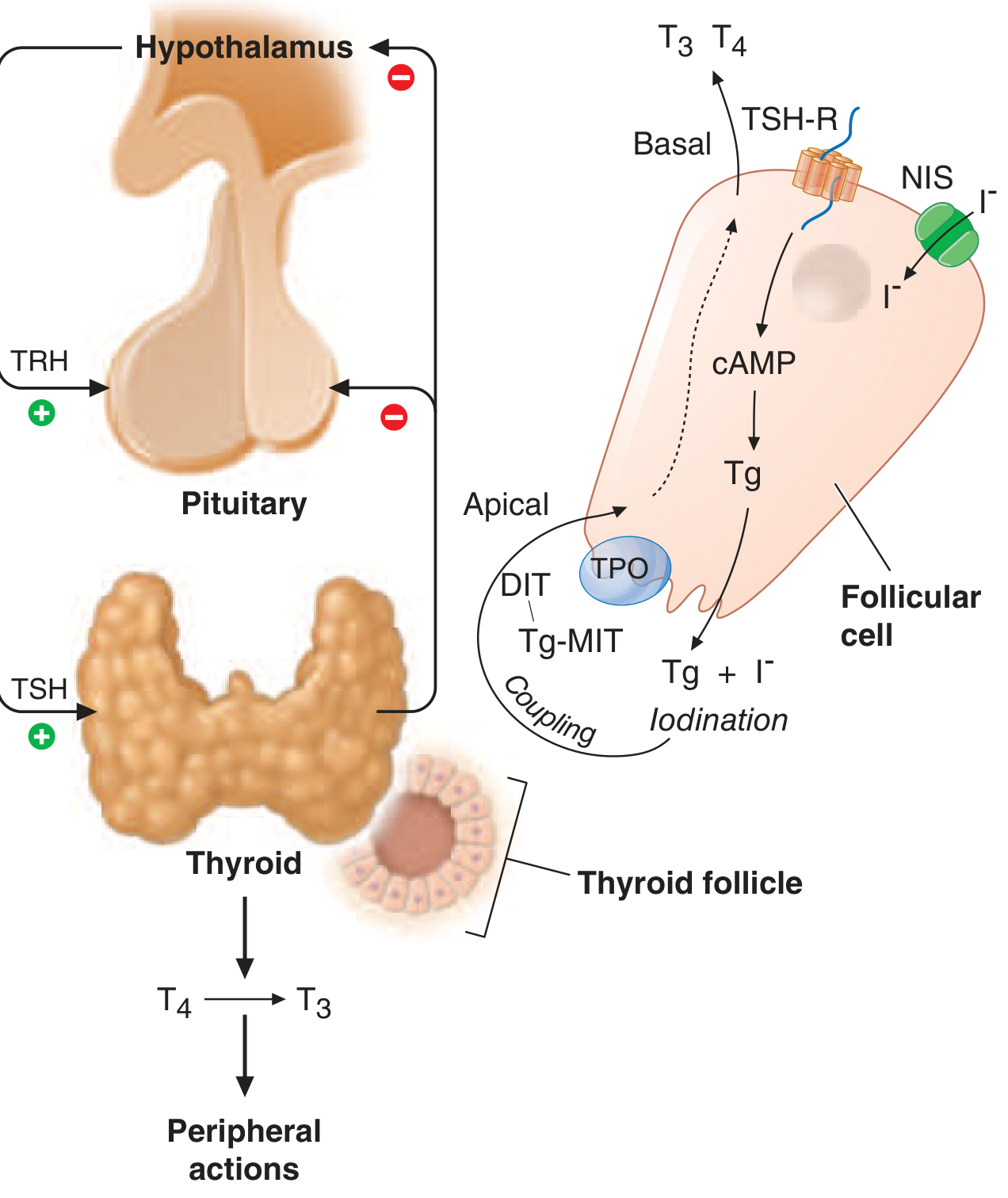
Step-by-step synthesis:
| Step | What Happens |
|---|---|
| 1. Iodide trapping | Sodium-iodide symporter (NIS) on the basolateral membrane co-transports 2 Na⁺ + 1 I⁻ into the follicular cell (secondary active transport driven by Na/K-ATPase). Concentrates I⁻ 20-40x above plasma |
| 2. Iodide efflux | Pendrin (Cl⁻/I⁻ exchanger) on the apical membrane transports I⁻ into the colloid. Mutation → Pendred syndrome (goiter + deafness) |
| 3. Organification | Thyroid peroxidase (TPO) at the apical membrane oxidizes I⁻ to reactive iodine and attaches it to tyrosine residues on thyroglobulin → forms monoiodotyrosine (MIT) and diiodotyrosine (DIT) |
| 4. Coupling | TPO couples MIT + DIT → T3 (triiodothyronine); DIT + DIT → T4 (thyroxine). The hormones remain bound to thyroglobulin in the colloid |
| 5. Storage | Colloid acts as a reservoir - humans can survive 2 months on zero dietary iodine before hormone levels fall |
| 6. Secretion | On TSH stimulation, follicular cells endocytose colloid → lysosomes hydrolyze thyroglobulin → free T4 and T3 released into capillaries |
| 7. Recycling | MIT and DIT not secreted - deiodinase recovers the iodine for reuse. This provides ~2x more iodine than NIS intake |
Ganong's Review of Medical Physiology, 26E; Harrison's 22E
Daily secretion: ~80 µg T4, ~4 µg T3, ~2 µg reverse T3 (rT3)
3. Transport in Blood
Once in the circulation, thyroid hormones are lipophilic and bind heavily to plasma proteins:
| Protein | T4 bound (%) | T3 bound (%) |
|---|---|---|
| Thyroxine-binding globulin (TBG) | 67% | 46% |
| Transthyretin (TBPA) | 20% | 1% |
| Albumin | 13% | 53% |
- T4: 99.98% bound; free T4 only ~2 ng/dL; half-life ~6-7 days
- T3: 99.8% bound; free T3 ~0.3 ng/dL; shorter half-life, more rapid action
- Only free hormone is biologically active and feeds back to the pituitary
Key modifiers of TBG levels:
- TBG ↑: estrogens, pregnancy, OCP → total T4 rises but patient is euthyroid (free T4 normal)
- TBG ↓: glucocorticoids, androgens, nephrotic syndrome
Ganong's Review of Medical Physiology, 26E
4. Peripheral Metabolism: T4 → T3
T4 is a prohormone. The majority of circulating T3 (the active form) comes from peripheral deiodination of T4 by deiodinase enzymes in liver, kidney, and other tissues:
- Type 1 & 2 deiodinase: remove iodine from the outer ring → produce active T3
- Type 3 deiodinase: remove iodine from the inner ring → produce reverse T3 (rT3), which is inactive
- T3 is ~3-4x more potent than T4 at the nuclear receptor
5. Mechanism of Action
Thyroid hormones act primarily on nuclear receptors (TR-α and TR-β):
- Free T3/T4 diffuses across the cell membrane
- T3 binds thyroid receptor → receptor-hormone complex binds thyroid response elements (TREs) on DNA → alters gene transcription
Major physiological effects:
- Increase basal metabolic rate (O₂ consumption, heat generation)
- Stimulate protein synthesis and carbohydrate/fat metabolism
- Essential for normal growth, brain development (especially fetal/neonatal)
- Increase sensitivity to catecholamines (↑ heart rate, cardiac output)
- Required for normal GI motility
- Regulate bone turnover
6. The HPT Feedback Axis
Hypothalamus
↓ TRH (+)
Anterior Pituitary
↓ TSH (+)
Thyroid Gland
↓ T4 / T3 (+)
Peripheral Tissues
↕
Free T3/T4 — negative feedback on both hypothalamus & pituitary
- TSH (thyroid-stimulating hormone) is the master regulator - even tiny changes in free T4/T3 cause large inverse TSH changes
- TSH acts via Gs-protein → cAMP → drives all steps of hormone synthesis and thyroid growth
7. Clinical Conditions at a Glance
Hypothyroidism
Cause: Most commonly Hashimoto's thyroiditis (autoimmune destruction); also iodine deficiency, post-thyroidectomy, post-radioiodine
TSH/hormone pattern: TSH ↑, free T4 ↓
Symptoms (think: everything slowed down):
- Fatigue, cold intolerance, weight gain, constipation
- Bradycardia, dry skin, hair loss, myxedema (non-pitting edema)
- Delayed relaxation of deep tendon reflexes
- Elevated TSH is the most sensitive screening test
Treatment: Levothyroxine (LT4) - typical dose 1.6 µg/kg/day. Goal: TSH in lower half of normal range. Check TSH 6-8 weeks after dose changes.
Harrison's Principles of Internal Medicine 22E
Hyperthyroidism / Thyrotoxicosis
Cause: Most commonly Graves' disease (TSH-receptor stimulating antibodies); also toxic multinodular goiter, toxic adenoma
TSH/hormone pattern: TSH ↓, free T4/T3 ↑
Symptoms (think: everything sped up):
- Palpitations, tachycardia, atrial fibrillation
- Heat intolerance, sweating, weight loss despite increased appetite
- Tremor, anxiety, irritability
- Diarrhea/hyperdefecation, increased bowel motility
- Systolic hypertension, increased cardiac output, reduced peripheral vascular resistance
Cardiovascular note: Thyrotoxicosis carries the highest morbidity risk via AF, cardiac hypertrophy, and heart failure. The risk of cardiovascular death is higher than in euthyroid individuals. Beta-blockers (propranolol) help control adrenergic symptoms even though catecholamine levels are actually normal.
Treatment: Beta-blockers (symptom control), thionamides (PTU, methimazole - block TPO), radioiodine ablation, thyroidectomy
Tietz Textbook of Laboratory Medicine, 7E; Harrison's 22E
Graves' Disease - Special Features
- Diffuse goiter (smooth, enlarged thyroid)
- Ophthalmopathy (proptosis, lid lag, periorbital edema) - from retroorbital inflammation
- Pretibial myxedema (dermopathy) - orange-peel skin on shins
- TSH-receptor antibodies (TRAb/TSI) are diagnostic
8. Lab Interpretation Quick Reference
| Condition | TSH | Free T4 | Free T3 |
|---|---|---|---|
| Primary hypothyroidism | ↑↑ | ↓ | ↓ |
| Subclinical hypothyroidism | ↑ | Normal | Normal |
| Hyperthyroidism | ↓↓ | ↑ | ↑ |
| Subclinical hyperthyroidism | ↓ | Normal | Normal |
| Secondary hypothyroidism (pituitary) | ↓ or normal | ↓ | ↓ |
| Non-thyroidal illness ("sick euthyroid") | Variable | ↓ T3, ↑ rT3 | ↓ |
| High TBG (e.g., pregnancy) | Normal | Normal | Normal |
TSH is the single best first-line test for thyroid function in outpatient screening. Free T4 adds information once TSH is abnormal.
9. Iodine - The Essential Substrate
- Minimum dietary requirement: ~50 mg/year (~1 mg/week)
- Normal uptake: ~10-25% of ingested radioiodine absorbed by thyroid in 24h; up to 70-90% in Graves' disease
- Both deficiency AND excess inhibit thyroid function (Wolff-Chaikoff effect for excess)
- Worldwide, iodine deficiency affects ~2 billion people and is the leading preventable cause of intellectual disability (cretinism in severe neonatal deficiency)
- NIS expression in the thyroid (but not most other tissues) is the basis for radioiodine scanning and treatment of thyroid cancer
Harrison's 22E; Ganong's 26E; Guyton & Hall
Sources consulted:
- Harrison's Principles of Internal Medicine 22E (2025)
- Ganong's Review of Medical Physiology, 26E
- Guyton and Hall Textbook of Medical Physiology
- Tietz Textbook of Laboratory Medicine, 7E
This is a shared conversation. Sign in to Orris to start your own chat.