Neurological cell and how oligodendrocytes extend multiple process and allow them to mylenate multipe segment of multiple neuron
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive content from two authoritative textbooks and three diagrams. Here is the full answer:
Oligodendrocytes: Structure, Processes, and Myelination of Multiple Neurons
Overview of Neuroglial Cells
The CNS contains four major types of glial cells: astrocytes, oligodendrocytes, microglia, and ependymal cells. Oligodendrocytes are the dedicated myelinating cells of the CNS - their PNS counterpart is the Schwann cell, but the two differ fundamentally in how many axons they can myelinate.
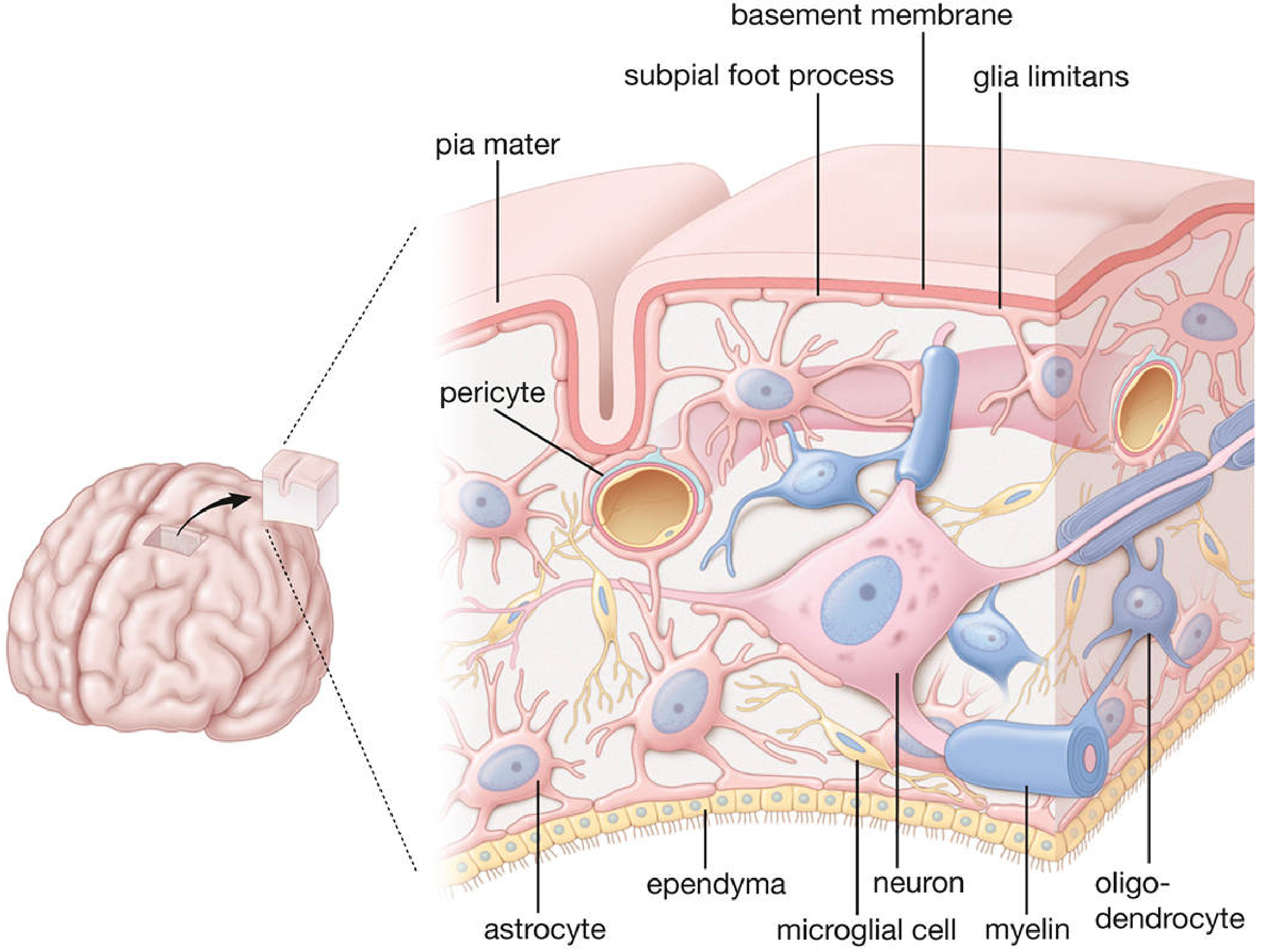
What Is an Oligodendrocyte?
Oligodendrocytes appear in specially stained light-microscopy preparations as small cells with relatively few processes compared to astrocytes. Their name reflects this - "oligo" = few, "dendro" = tree-like processes. In white matter, they are often aligned in rows between axons.
- The cell body (soma) may sit at some distance from the axons it is myelinating
- In gray matter, oligodendrocytes do not produce myelin and instead exist as peri-neuronal satellite cells
- In white matter, each oligodendrocyte has 15 to 30 processes, each connecting a separate myelin sheath back to the cell body
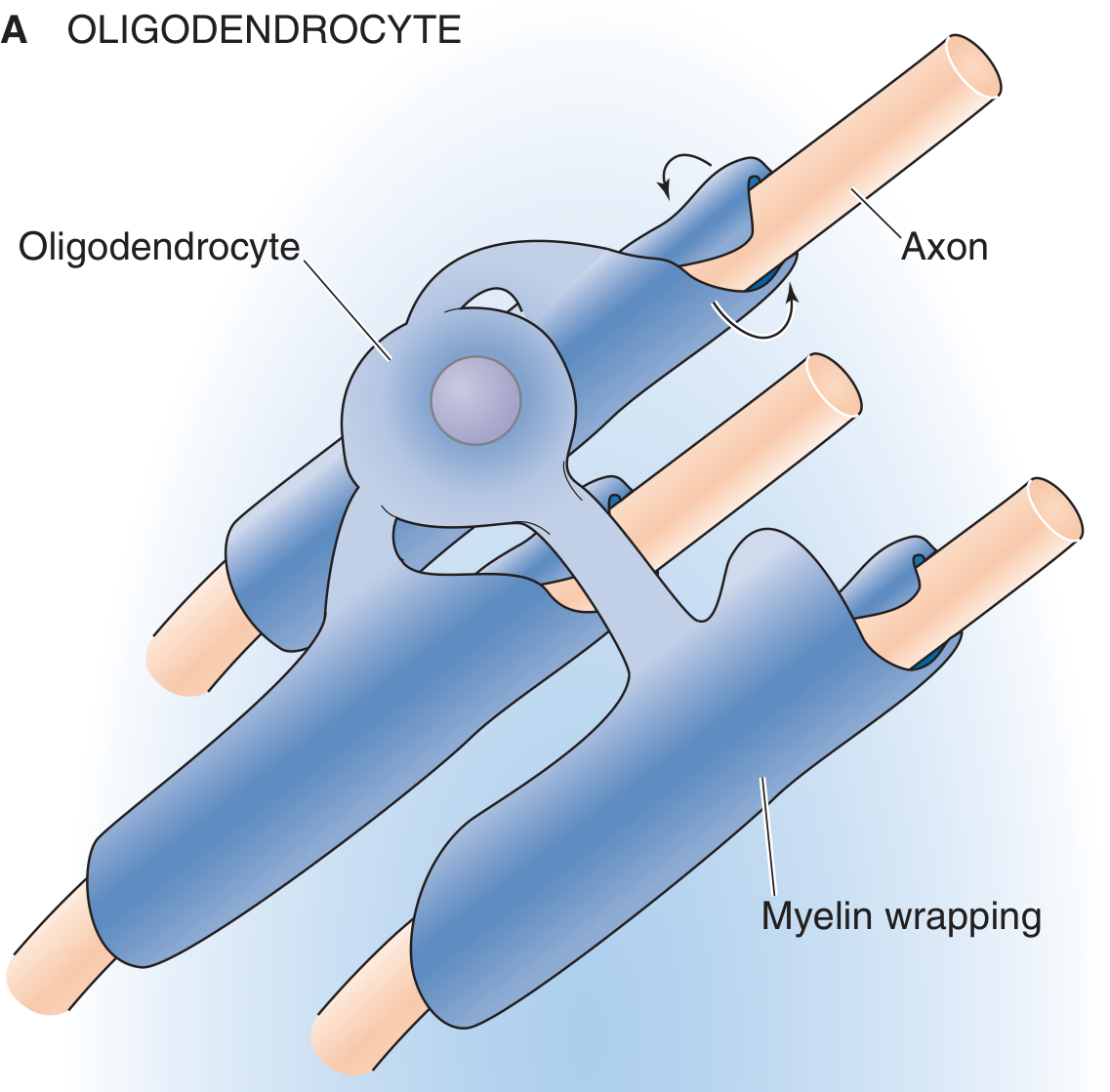
How Oligodendrocytes Extend Processes to Myelinate Multiple Axons
Each oligodendrocyte extends multiple tongue-like cytoplasmic processes that radiate outward from the cell body and make contact with nearby axons. Each individual process then wraps itself spirally around a portion (one internodal segment) of a single axon, forming a myelin sheath.
This is the key distinction from Schwann cells:
| Feature | Oligodendrocyte (CNS) | Schwann Cell (PNS) |
|---|---|---|
| Axons myelinated | Up to 15-30 different axons | Only 1 axon per cell |
| Myelin segments per cell | Multiple (one per process) | One internodal segment |
| External basal lamina | Absent | Present |
| Unmyelinated axons | Often bare (no glial wrapping) | Embedded in Schwann cell cytoplasm |
The Myelination Mechanism: How Wrapping Occurs
Because one oligodendrocyte myelinates several axons simultaneously, it cannot embed the axon in its cytoplasm the way a Schwann cell does (the mesaxon wrapping method used in the PNS). Instead, the mechanism is:
- A tongue-like process extends from the oligodendrocyte body and contacts a nearby axon
- The leading edge of the process spirals around the axon repeatedly, staying in close proximity to it
- After many wraps are completed, cytoplasm is squeezed out from between the membrane layers - a process called compaction
- This creates layer upon layer of tightly compressed, lipid-rich plasma membranes - which is what myelin actually is
- Each myelin sheath can be up to 250 μm wide, and it wraps many times along the long axis of one axon segment
- The myelin sheaths remain continuous with the parent oligodendrocyte, which nourishes them
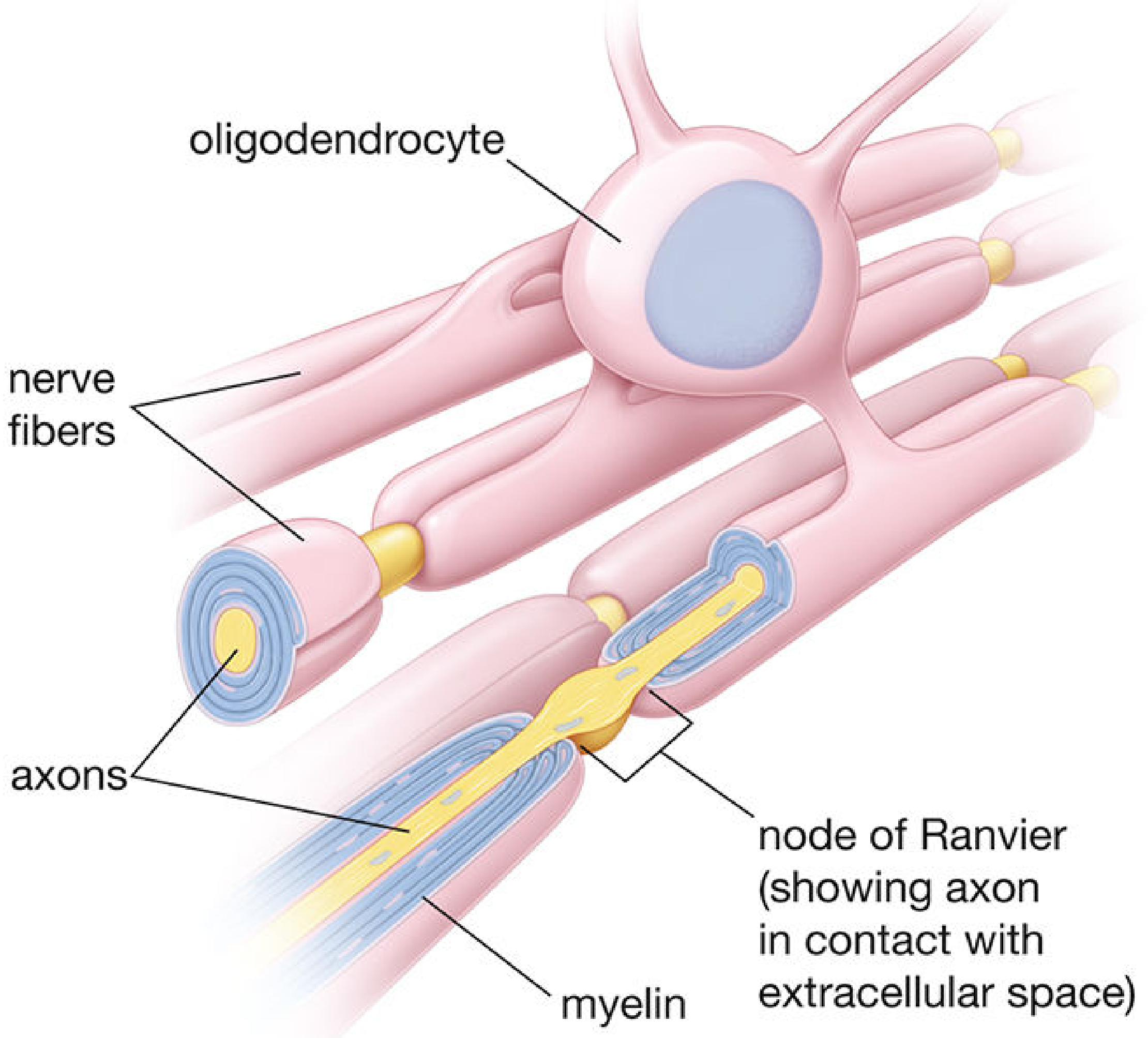
The Node of Ranvier
The small exposed stretch of axon between adjacent myelin sheaths from two neighboring oligodendrocytes is called the node of Ranvier. Nodes in the CNS are actually larger than those in the PNS. This larger exposed axolemma makes saltatory conduction (the jumping of action potentials from node to node) even more efficient in the CNS.
Myelin Composition: CNS vs. PNS Proteins
Oligodendrocytes and Schwann cells express different sets of myelin-specific proteins:
| Protein | CNS (% of total myelin protein) | PNS |
|---|---|---|
| Proteolipid protein (PLP) | ~50% | <0.01% |
| Myelin basic protein (MBP) | ~30% | <18% |
| Myelin-associated glycoprotein (MAG) | <1% | ~0.1% |
| Cyclic nucleotide phosphodiesterase (CNP) | <4% | present |
| Myelin oligodendrocyte glycoprotein (MOG) | present | absent |
| P0 / PMP22 | absent | major proteins |
Deficiencies in CNS-specific myelin proteins (MOG, PLP) are implicated in autoimmune demyelinating diseases. MOG antibodies are the target in MOG antibody-associated disease (MOGAD).
Key Structural Differences Between CNS and PNS Myelin
- CNS myelin has fewer Schmidt-Lanterman clefts because astrocytes (not the myelin-forming cell itself) provide metabolic support
- Oligodendrocytes have no external basal lamina, so adjacent myelin sheaths can directly contact each other and may share an intraperiod line
- Since cytoplasm is largely absent from the outermost myelin layer, CNS myelin appears more compact ultrastructurally
Why Does This Matter Clinically?
In diseases like multiple sclerosis (MS), the oligodendrocyte is the primary target. Its destruction leads to demyelination of multiple CNS axon segments simultaneously - since each oligodendrocyte services up to 30 internodal segments across multiple axons, loss of one cell can cause widespread conduction failure. The plaques of MS represent focal areas of oligodendrocyte destruction and myelin loss.
Sources:
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, pp. 969-971
- Medical Physiology (Boron & Boulpaep), pp. 444-445
The extra dural space in brain is potentially space not a reak space
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a precise, well-sourced answer. Here it is:
The Extradural (Epidural) Space in the Brain: Potential vs. Real
Your statement is CORRECT - with an important nuance
The cranial extradural (epidural) space is indeed a potential space, not a real space under normal conditions. The textbooks confirm this exactly.
Why It Is a Potential Space in the Brain
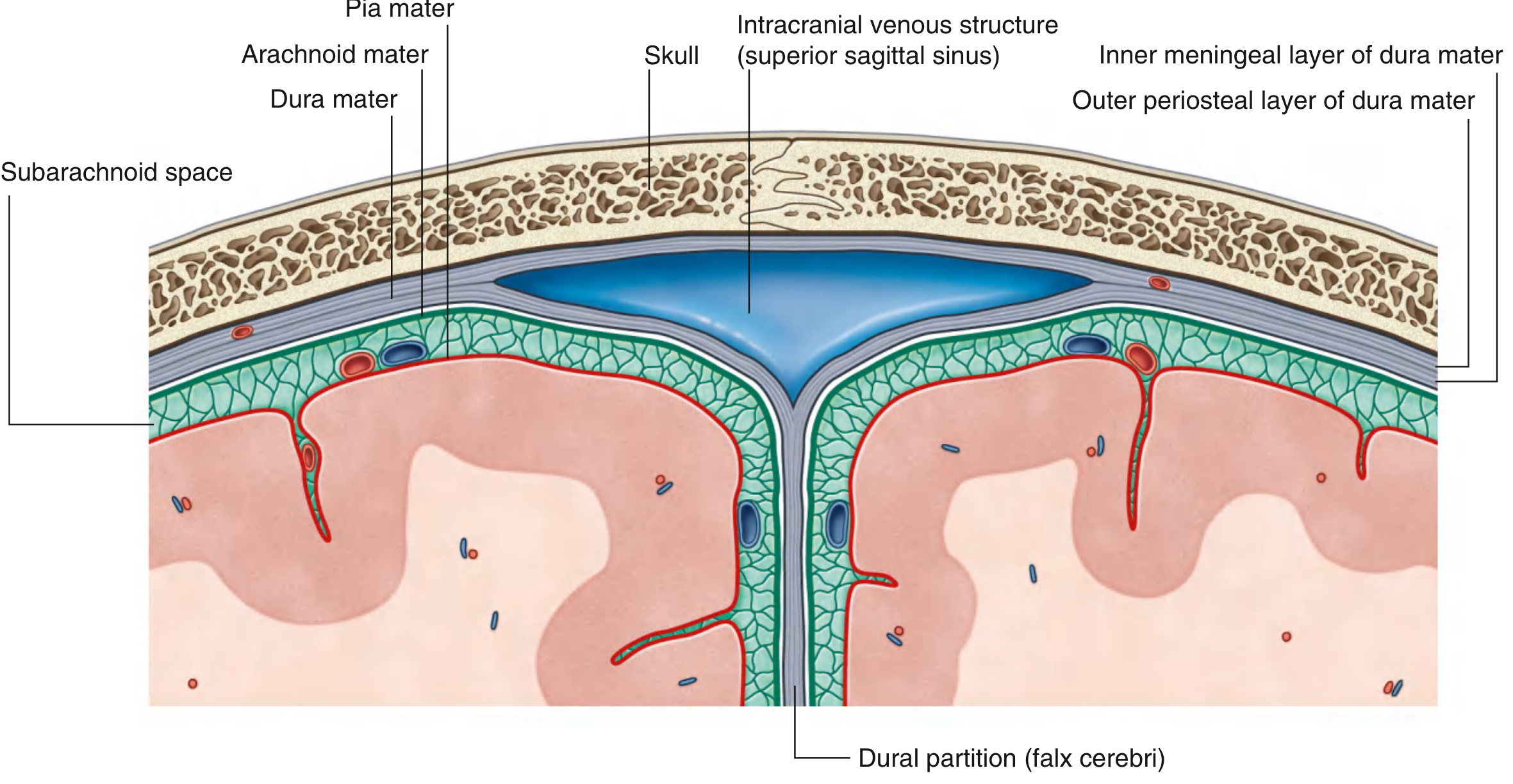
The cranial dura mater has two layers:
- Outer periosteal layer - tightly adherent/fused to the inner surface of the skull bones
- Inner meningeal layer - lies against the underlying arachnoid mater
Because the outer periosteal layer is adherent to the skull, the extradural space between the skull and this outer dural layer does not normally exist as an open gap. It only becomes a real space when pathological forces - most commonly arterial hemorrhage - strip the dura away from the bone.
As Gray's Anatomy for Students states directly:
"Two potential spaces exist as the epidural (extradural) space, superficial to the periosteal layer, and subdural space deep to the meningeal dural layer. These spaces can become filled with blood during vascular trauma."
And from Shambaugh's Surgery of the Ear:
"The epidural (extradural) space is a potential space between the dura mater and the bone of the intracranial cavity."
Contrast With the Spinal Epidural Space
This is where many students get confused - the two epidural spaces are anatomically very different:
| Feature | Cranial Epidural Space | Spinal Epidural Space |
|---|---|---|
| Nature | Potential space only | Real space (exists normally) |
| Why? | Dura is fused/adherent to skull periosteum | Dura is separated from vertebral canal by fat, veins, and loose connective tissue |
| Normal contents | None | Fat, epidural venous plexus, lymphatics |
| Clinical access | Not routinely accessible | Used for epidural anaesthesia/analgesia |
Gray's Anatomy for Students explicitly notes this contrast:
"[The spinal cord] is separated from the bony vertebral canal by the epidural/extradural space. In addition, unlike in the cranial cavity, the underlying arachnoid mater is not tightly adherent to the dura mater..."
When the Cranial Potential Space Becomes Real: Epidural Hematoma
The cranial epidural space only becomes a real, blood-filled space in pathology - specifically, epidural (extradural) hematoma, most commonly caused by:
- Rupture of the middle meningeal artery (a branch of the maxillary artery that runs in grooves on the inner skull surface)
- Typically from temporal bone fractures following blunt head trauma
- Arterial pressure strips the dura away from the skull, creating a biconvex (lens-shaped) hematoma on CT
The clinical hallmark is the "lucid interval" - brief loss of consciousness, followed by recovery, then rapid neurological deterioration as the hematoma expands under arterial pressure.
Summary Table: All Meningeal Spaces
| Space | Location | Type | Normal Contents |
|---|---|---|---|
| Cranial epidural | Between skull and outer dural periosteum | Potential | None |
| Subdural | Between inner dura and arachnoid | Potential | Thin film of fluid |
| Subarachnoid | Between arachnoid and pia mater | Real | CSF, blood vessels |
| Spinal epidural | Between vertebral canal and spinal dura | Real | Fat, veins |
Sources:
- Gray's Anatomy for Students, Meninges section, p. 1305
- Gray's Anatomy for Students, Spinal Meninges section, p. 1325
- Shambaugh's Surgery of the Ear, Epidural Abscess section
Epidural hemorrhage
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content, CT imaging, and a gross pathology image. Here is the complete answer:
Epidural Hemorrhage (Extradural Hematoma - EDH)
Definition
An epidural (extradural) hematoma is a collection of blood in the potential space between the inner surface of the skull and the outer periosteal layer of the dura mater. As discussed in the previous topic, this space does not normally exist - blood must first strip the dura away from the bone under sufficient pressure to create it.
Etiology and Source of Bleeding
Primary Cause - Arterial (most common)
The classic and most dangerous cause is rupture/laceration of the middle meningeal artery (MMA), a branch of the maxillary artery that runs in grooves along the inner surface of the temporal bone. It is torn by a fracture of the squamous temporal bone - most often at the pterion, the thinnest part of the skull, where the frontal, parietal, temporal, and sphenoid bones converge.
Because bleeding is arterial, it is under high pressure, rapidly expanding, and capable of stripping the dura far from the bone. This is why EDH can be rapidly fatal.
Other Arterial Sources
- Anterior meningeal artery - frontotemporal hematomas
- Posterior meningeal artery - parietooccipital hematomas
Venous Causes (less common)
Bleeding from diploic veins, middle meningeal veins, or dural sinuses can also cause EDH, but venous pressure is insufficient to rapidly strip dura from bone - so these bleed more slowly, behave more like subdural hematomas, and are often self-limited.
"The inability of the venous system to generate sufficient pressure to strip dura from bone accounts for the infrequency of epidural hematomas following venous injury." - DiMaio's Forensic Pathology
Special Case in Children
EDH without skull fracture can occur in children due to their very elastic bones - the dura can be avulsed without fracture. Bleeding in these cases is usually minor.
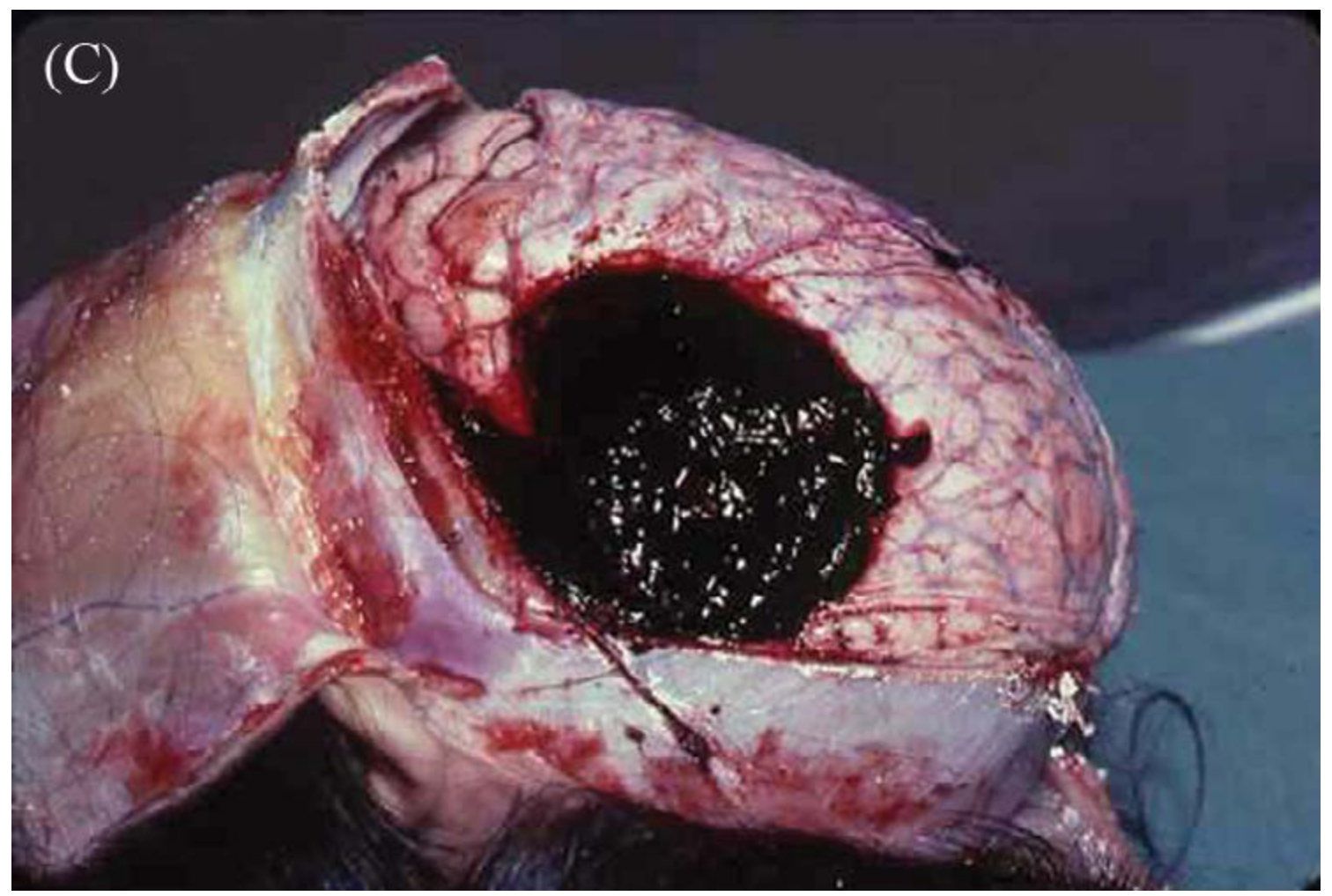
Why EDH Is Almost Always Unilateral
The dura is tightly fused to the skull at the cranial sutures. This firm attachment prevents blood from crossing suture lines. As a result:
- EDHs are virtually always unilateral
- They have a characteristic lens-shaped (biconvex/lenticular) morphology - convex on both surfaces, bounded by sutures
- They do not cross suture lines (unlike subdural hematomas, which cross freely)
CT and Imaging Appearance
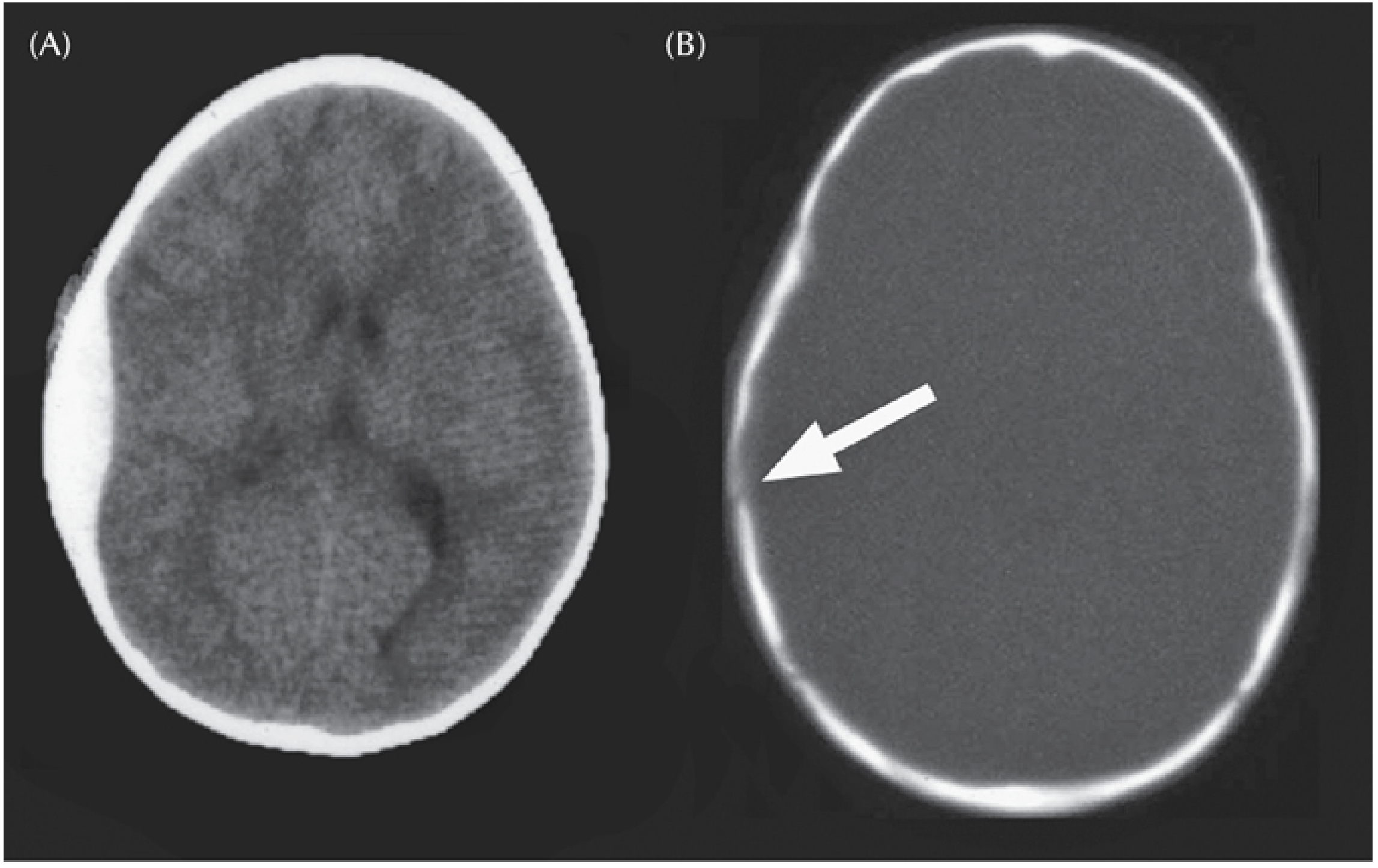
On CT:
- Hyperdense (bright white) biconvex/lens-shaped collection between skull and brain
- Does not cross suture lines
- Midline shift if large
- The dura itself may appear as a thin linear structure pushed toward the brain
On MRI: Signal characteristics evolve like other hematomas - the pattern of deoxy-hemoglobin → met-hemoglobin → hemosiderin follows the same timeline as other intracranial bleeds.
Gross Pathology
Classic Clinical Presentation - The "Lucid Interval"
The classic teaching sequence is:
Head trauma → Brief loss of consciousness → LUCID INTERVAL → Rapid deterioration → Coma → Death (if untreated)
However, this "classic" picture occurs in only 15-20% of patients. More commonly:
- Many patients never lose consciousness initially
- Most EDHs today are detected on CT scans done for even mild concussion in the emergency department
- Only ~30% ultimately require surgical intervention
Why the lucid interval occurs:
- The initial blow may briefly stun the brain (transient concussion)
- As the dura is slowly stripped by arterial blood, the brain compensates initially
- As the hematoma expands over 4-8 hours, ICP rises
- Compression of the temporal lobe leads to uncal herniation
- The uncus herniates over the tentorial edge, compressing CN III (oculomotor nerve)
Neurological signs of expanding EDH:
| Sign | Mechanism |
|---|---|
| Headache (often attributed to trauma) | Stretching of pain-sensitive meninges and vessels at base of middle fossa |
| Ipsilateral pupil dilation (early) | CN III compression by uncal herniation |
| Complete ophthalmoparesis (late) | Progressive CN III palsy |
| Contralateral motor weakness | Compression of ipsilateral cerebral peduncle |
| Decreasing consciousness → coma | Rising ICP, bilateral hemisphere dysfunction |
| Battle's sign | Ecchymosis behind the ear - indicates basal skull fracture |
| Raccoon eyes | Periorbital ecchymosis - also indicates basal skull fracture |
| Blood behind tympanic membrane | Temporal bone fracture |
"Patients who 'talk and die'" - the clinical phrase describing the lucid interval, emphasizing that seemingly alert patients can rapidly deteriorate.
Comparison: EDH vs. SDH vs. SAH
| Feature | EDH | SDH | SAH |
|---|---|---|---|
| Location | Between skull and dura | Between dura and arachnoid | Between arachnoid and pia |
| Usual source | Arterial (MMA) | Venous (bridging veins) | Arterial (Berry aneurysm) |
| CT shape | Biconvex (lens) | Crescent-shaped | Fills cisterns/sulci |
| Crosses sutures? | No | Yes | N/A |
| Classic symptom | Lucid interval | Variable | Thunderclap headache |
| Age group | Young adults/children | Elderly (chronic) | Adults 40-60 |
Treatment
Emergent surgical decompression is the treatment for significant EDH:
- Temporal craniotomy - evacuates the hematoma and allows coagulation of the torn MMA
- Must be performed before herniation syndrome develops for best outcomes
- If performed promptly, outcomes can be excellent because the brain parenchyma itself is often uninjured (the damage is compressive, not intrinsic)
"If performed prior to a herniation syndrome, patient outcomes can be excellent." - Mulholland & Greenfield's Surgery
Conservative management may be appropriate for small hematomas (<30 mL, <15 mm thickness, <5 mm midline shift) in neurologically intact patients, with close monitoring and repeat CT.
Sources:
- Neuroanatomy through Clinical Cases, 3rd Ed., pp. 173-174
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma, pp. 246-247
- DiMaio's Forensic Pathology, 3rd Ed., pp. 141-142
- Mulholland & Greenfield's Surgery, 7th Ed., p. 1135
- Bradley and Daroff's Neurology in Clinical Practice, p. 739
This is a shared conversation. Sign in to Orris to start your own chat.