Discuss role of growth factors in inflammation and repair.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"growth factors" AND "wound healing" AND inflammation
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a thorough, well-illustrated answer. Here it is:
Role of Growth Factors in Inflammation and Repair
Growth factors are soluble peptide mediators that bind to specific cell-surface receptors (most carrying intrinsic tyrosine kinase activity) and drive the cellular events of inflammation, regeneration, and scar formation. They act in autocrine, paracrine, or endocrine fashions and are produced at injury sites by macrophages, platelets, epithelial cells, fibroblasts, and endothelial cells.
Overview: Tissue Repair and the Proliferative Capacity of Tissues
Before growth factors can drive repair, the tissue must have the ability to respond. Tissues are classified into three groups based on this capacity:
- Labile tissues (skin epithelium, GI mucosa, bone marrow): continuously renewing; readily regenerate after injury if stem cells are preserved.
- Stable tissues (liver, kidney, fibroblasts, endothelium): quiescent at rest but can re-enter the cell cycle in response to growth factors after injury.
- Permanent tissues (neurons, cardiac muscle): terminally differentiated; cannot regenerate; repair defaults to scar formation.
Cell proliferation in all these tissues is driven by signals from growth factors and the extracellular matrix (ECM). Most growth factors are produced by cells near the injury site - primarily macrophages - but epithelial and stromal cells also contribute. Several factors are stored in ECM-bound reservoirs and released only by proteolysis at wound sites.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 35-36
Key Growth Factors: Sources and Functions
The table below summarizes the major growth factors involved in regeneration and repair (Table 1.1, Robbins):
| Growth Factor | Principal Sources | Key Functions |
|---|---|---|
| EGF (Epidermal Growth Factor) | Activated macrophages, salivary glands, keratinocytes | Mitogenic for many cell types; stimulates epithelial cell migration; promotes granulation tissue formation |
| TGF-α (Transforming GF-alpha) | Activated macrophages, keratinocytes | Stimulates proliferation of hepatocytes and many epithelial cells |
| HGF (Hepatocyte GF / scatter factor) | Fibroblasts, stromal cells, endothelial cells | Enhances proliferation of hepatocytes and epithelial cells; increases cell motility |
| VEGF (Vascular Endothelial GF) | Mesenchymal cells | Stimulates endothelial proliferation and migration; increases vascular permeability; major driver of angiogenesis |
| PDGF (Platelet-Derived GF) | Platelets, macrophages, endothelium, smooth muscle, keratinocytes | Chemotactic for neutrophils, macrophages, fibroblasts, and smooth muscle cells; stimulates fibroblast and endothelial proliferation; promotes ECM synthesis |
| FGFs (Fibroblast GFs, incl. FGF-1, FGF-2) | Macrophages, mast cells, endothelial cells | Chemotactic and mitogenic for fibroblasts; stimulates angiogenesis and ECM protein synthesis |
| TGF-β (Transforming GF-beta) | Platelets, T cells, macrophages, endothelium, fibroblasts | Chemotactic for leukocytes and fibroblasts; stimulates ECM protein synthesis; suppresses acute inflammation; major driver of fibrosis |
| KGF / FGF-7 (Keratinocyte GF) | Fibroblasts | Stimulates keratinocyte migration, proliferation, and differentiation |
Phase-by-Phase Role in Inflammation and Repair
1. Hemostasis and Initiation of Inflammation
The first event after tissue injury is platelet activation and clot formation. Activated platelets release PDGF and TGF-β from their alpha-granules. These are among the earliest growth factors at the wound site:
- PDGF is chemotactic for neutrophils, monocytes, and fibroblasts - recruiting the initial inflammatory infiltrate to the wound bed.
- TGF-β from platelets also begins recruiting leukocytes and sets the stage for fibroblast migration later.
The hemostatic plug and fibrin clot serve as the provisional matrix scaffold on which subsequent repair is built.
2. Inflammatory Phase (0-48 hours)
Neutrophils arrive first (within 6-24 hours), followed by monocytes that mature into macrophages. At this stage, growth factors serve two main purposes: amplifying inflammation and beginning to transition toward repair.
- Macrophages are the central orchestrators. M1 (classically activated) macrophages dominate early, clearing debris and microbes. They produce EGF, TGF-α, PDGF, and FGFs that begin signaling to resident fibroblasts and epithelial cells.
- PDGF continues to recruit and activate macrophages and fibroblasts from the surrounding tissue.
- As debris is cleared, macrophages gradually polarize toward the M2 (alternatively activated) phenotype - the critical transition that dampens inflammation and initiates repair. M2 macrophages produce growth factors (including VEGF, TGF-β, and PDGF) that drive angiogenesis and fibroblast activity.
3. Proliferative Phase: Epithelial Repair, Angiogenesis, and Granulation Tissue (Days 2-10)
This phase involves three overlapping processes driven by growth factors:
A. Re-epithelialization
- EGF and KGF (FGF-7) stimulate keratinocyte migration across the wound surface and proliferation of basal epithelial cells at the wound margins.
- FGF-2 further promotes epithelial cell migration.
- HGF (scatter factor) enhances motility and proliferation of epithelial cells across the wound.
B. Angiogenesis
New vessel formation is essential to deliver oxygen and nutrients to the regenerating tissue. Growth factors drive angiogenesis via the following steps:
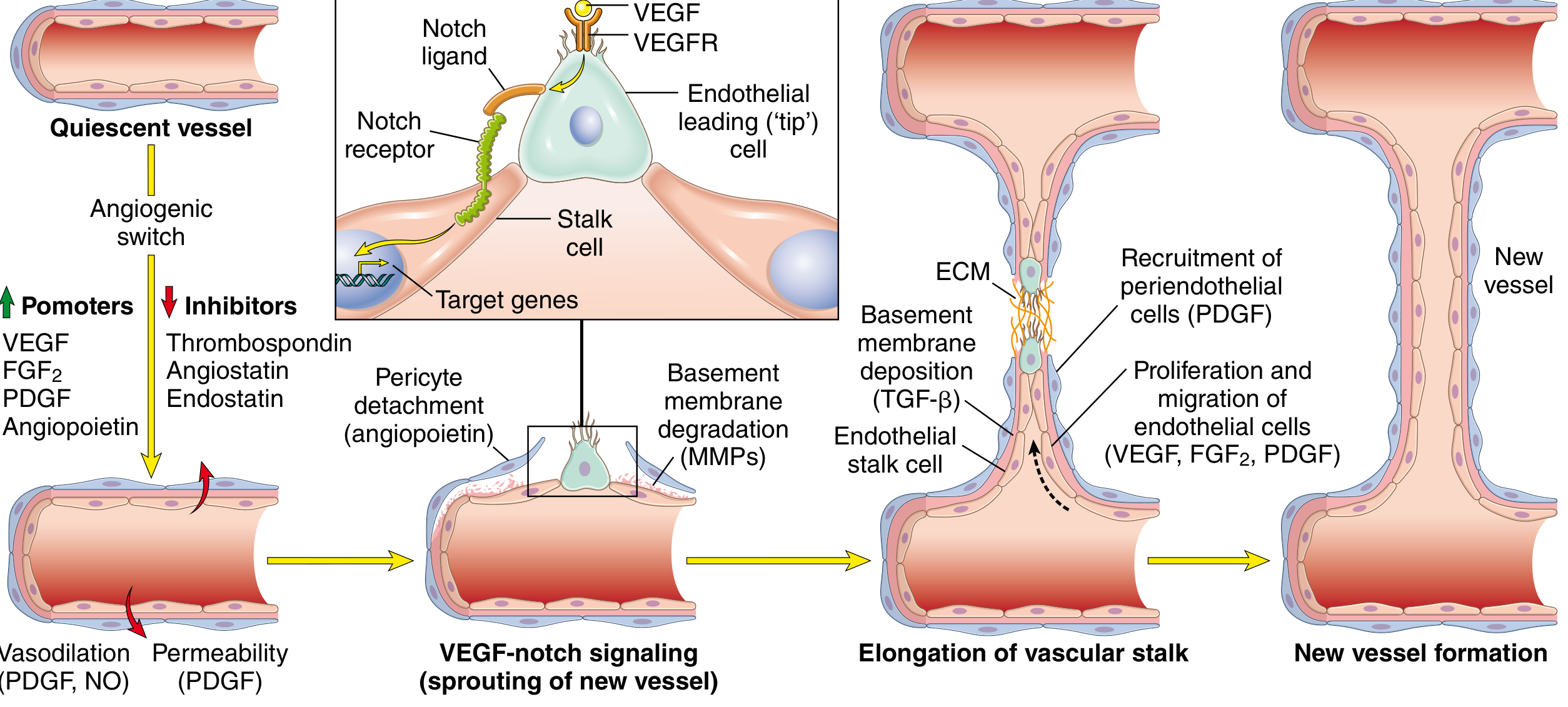
Fig. Steps in angiogenesis by vessel sprouting, showing the roles of VEGF, FGF-2, PDGF, TGF-β, and angiopoietins. (Robbins, Cotran & Kumar)
- VEGF-A (produced by mesenchymal and inflammatory cells, strongly induced by hypoxia via HIF-1 transcription factor) is the master switch. It stimulates vasodilation (via NO production), increases vascular permeability, and drives endothelial cell migration and proliferation ("angiogenic switch"). VEGFR-2 on endothelial cells is the primary signaling receptor.
- FGF-2 (bFGF) stimulates endothelial proliferation, promotes macrophage and fibroblast migration to the damaged area, and also stimulates epithelial cell migration over wounds.
- Angiopoietins 1 and 2 (Ang1, Ang2) regulate angiogenesis and structural maturation of new vessels.
- PDGF stabilizes newly formed vessels by recruiting pericytes and smooth muscle cells to the vessel wall.
- TGF-β suppresses further endothelial proliferation/migration once vessels are established and promotes basement membrane deposition, consolidating the mature vessel.
- Notch signaling (activated by VEGF) regulates vessel branching patterns to ensure appropriate spacing of new capillaries.
C. Granulation Tissue and Fibroblast Activity
Granulation tissue forms by the combination of proliferating fibroblasts, new vessels, and a loose ECM infiltrated by macrophages:
- PDGF, FGF-2, and TGF-β are the principal orchestrators. These are produced mainly by M2 macrophages, mast cells, and lymphocytes in the granulation tissue.
- PDGF induces fibroblast and smooth muscle cell proliferation and migration into the wound.
- FGF-2 is chemotactic and mitogenic for fibroblasts and stimulates ECM protein synthesis.
4. Connective Tissue Deposition and Remodeling
As granulation tissue matures, the emphasis shifts from proliferation to matrix synthesis and remodeling:
- TGF-β is the single most important cytokine at this stage. It:
- Stimulates fibroblast migration and proliferation
- Strongly upregulates synthesis of collagen and fibronectin
- Decreases ECM degradation by inhibiting matrix metalloproteinases (MMPs) and increasing tissue inhibitors of metalloproteinases (TIMPs)
- Is an antiinflammatory cytokine, limiting and terminating the inflammatory response by inhibiting lymphocyte proliferation and leukocyte activity
- Is produced by M2 macrophages, platelets, T cells, and fibroblasts in the granulation tissue
TGF-β levels are regulated primarily at the post-transcriptional level - by activation of latent TGF-β, rate of secretion, and ECM-bound molecules (notably integrins and fibrillin microfibrils) that modulate its activity.
Some fibroblasts acquire contractile features and are called myofibroblasts - they contribute to wound contraction. This is stimulated by TGF-β and PDGF.
The outcome of ECM deposition depends on the balance between:
- Fibrogenic signals (TGF-β)
- MMPs (activated by plasmin at wound sites)
- TIMPs (produced by mesenchymal cells to limit MMP activity)
5. Remodeling
Collagen in the initial scar undergoes continuous MMP-mediated remodeling and cross-linking, increasing tensile strength over weeks to months. Growth factors that previously stimulated fibroblasts diminish. Vascular regression converts the highly vascular granulation tissue into a pale, largely avascular scar.
Steps in Repair: Skin Wound Healing
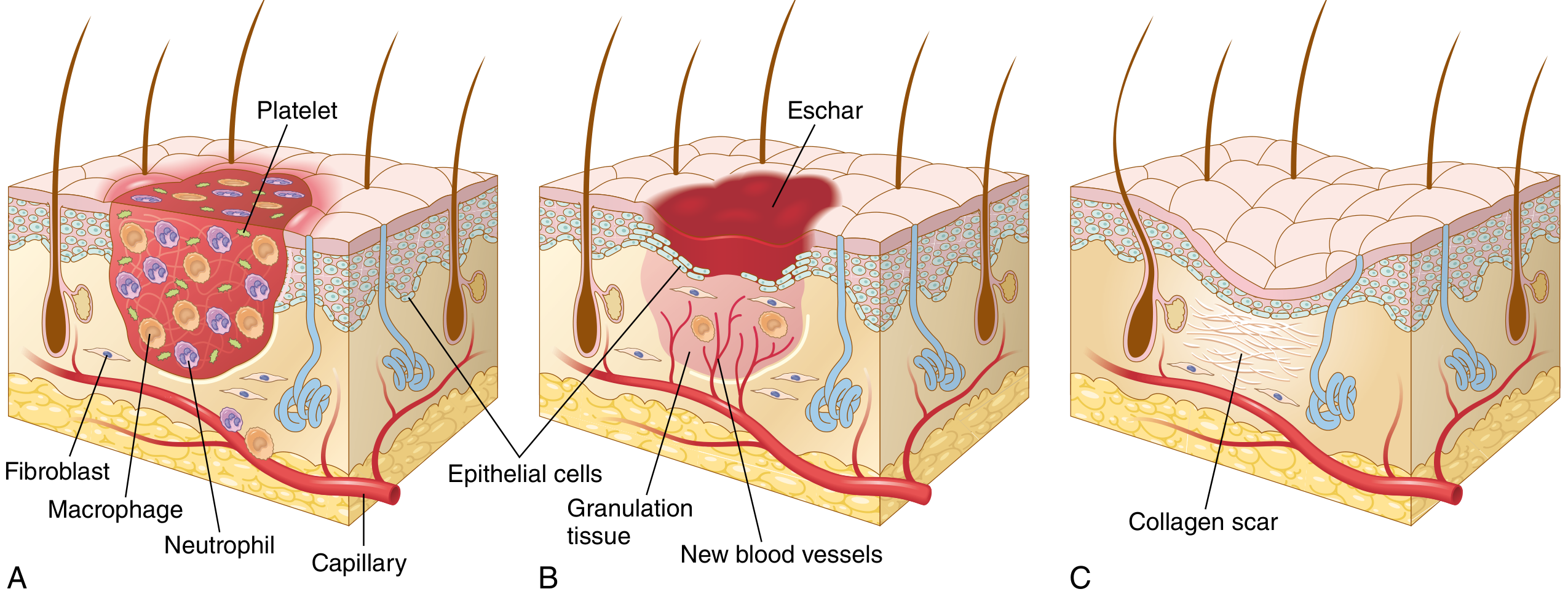
Fig. Steps in repair by scar formation - wound healing in skin. (A) Inflammation. (B) Proliferation of epithelial cells, formation of granulation tissue by vessel growth and proliferating fibroblasts. (C) Remodeling to produce the fibrous scar. (Robbins, Cotran & Kumar)
Role of the ECM in Growth Factor Signaling
The ECM is not merely a scaffold - it functions as a dynamic reservoir for growth factors and modulates their activity:
-
The ECM binds and concentrates growth factors such as FGFs (via heparan sulfate proteoglycans) and TGF-β (via fibrillin microfibrils), keeping them in an inactive state until proteolytic release at wound sites.
-
Integrin receptors on cells bind ECM proteins and trigger signaling cascades that interact with (and amplify) growth factor receptor signals.
-
ECM disruption prevents effective regeneration even when growth factors are present - intact basement membrane is required for organized tissue renewal.
-
Robbins, Cotran & Kumar, p. 36-37
Special Role in Liver Regeneration
The liver is the classic model for growth factor-driven tissue regeneration. After partial hepatectomy or injury:
-
Cytokines (TNF, IL-6) and growth factors (HGF, TGF-α, EGF) produced in response to loss of liver mass and inflammation trigger hepatocyte proliferation.
-
HGF acts on the c-Met receptor on hepatocytes and is the primary mitogenic signal.
-
TGF-α (produced by macrophages) stimulates hepatocyte proliferation.
-
When differentiated hepatocytes cannot regenerate (e.g., in severe cirrhosis), hepatic progenitor cells in the Canal of Hering expand and differentiate.
-
Robbins, Cotran & Kumar, p. 107-108
Pathologic Consequences: Fibrosis
When tissue injury is persistent (chronic inflammation), TGF-β and PDGF drive continuous fibroblast activation and collagen deposition beyond what is needed for repair, leading to fibrosis of:
- Lung (idiopathic pulmonary fibrosis)
- Liver (cirrhosis)
- Kidney (glomerulosclerosis, tubulointerstitial fibrosis)
- Dermis (keloids, hypertrophic scars)
TGF-β is the central mediator in all of these - its levels, duration of action, and sensitivity of the target tissue determine whether the outcome is physiologic scar formation or pathologic fibrosis.
Summary
| Phase | Dominant Growth Factors | Net Effect |
|---|---|---|
| Hemostasis/early inflammation | PDGF, TGF-β (from platelets) | Leukocyte and fibroblast recruitment |
| Inflammatory | EGF, TGF-α, PDGF (from macrophages) | Amplify inflammation; begin cell recruitment |
| Re-epithelialization | EGF, KGF/FGF-7, HGF, FGF-2 | Keratinocyte migration and proliferation |
| Angiogenesis | VEGF, FGF-2, PDGF, Angiopoietins, TGF-β | New vessel formation and stabilization |
| Granulation tissue | PDGF, FGF-2, TGF-β | Fibroblast proliferation, ECM synthesis |
| Remodeling/scar maturation | TGF-β (dominant) | Collagen cross-linking, MMP/TIMP balance, scar contraction |
Key principle: Macrophages - particularly M2-polarized macrophages - are the master orchestrators of repair, producing or inducing the growth factors that coordinate all phases from inflammation through scar maturation.
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Table 1.1, pp. 35-37, 107-114
- Robbins & Kumar Basic Pathology, pp. 2093-2112
- Dermatology, 5th ed. - "Growth Factors and Their Receptors," p. 4074
- Cellular and Molecular Immunology - "Role of Macrophages in Tissue Repair," p. 2647
Recent literature note: A 2025 systematic review (PMID 40076553) on cell-free regenerative medicine highlights secretome-derived growth factors (including VEGF, FGF, PDGF) as therapeutic targets in wound healing, consistent with the mechanisms above. A 2026 review (PMID 41297226) evaluates FGF-21 specifically in thermal injury repair - no major contradictions with established mechanisms were identified.
role of growth factors and cytokines involved in regeneration and wound healing.
Finding Sources
Finding Sources
Searching PubMed
"cytokines" AND "wound healing" AND "regeneration"
Reading File
Reading File
Reading File
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.