Gall bladder in detail about its anatomy , pathophysiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the detailed answer.
The Gallbladder: Detailed Anatomy and Pathophysiology
1. Overview
The gallbladder is a pear-shaped, distensible sac that serves as a storage reservoir for bile. It concentrates bile and delivers it in a controlled, high-concentration bolus to the duodenum to assist with fat digestion. In adults, it measures 7-10 cm in length, 3 cm in width, and holds approximately 30-50 mL of bile.
- Yamada's Textbook of Gastroenterology, 7e
- Sleisenger and Fordtran's GI and Liver Disease
2. Gross Anatomy
Position and Relations
The gallbladder lies in a fossa on the inferior (visceral) surface of the right lobe of the liver, at the anatomic boundary between the right and quadrate lobes. Its anterior surface faces the anterior abdominal wall, typically projecting to the level of the 9th costal cartilage at the right lateral border of the rectus abdominis muscle. Posteriorly it rests on:
- The transverse colon (behind the fundus)
- The superior part of the duodenum (behind the body)
- Gerota's fascia of the right kidney (posteriorly)
This intimate relationship means a perforated or inflamed gallbladder can readily fistulize into the colon or duodenum.
Four Anatomical Parts
| Part | Description |
|---|---|
| Fundus | Rounded, blind end; projects 0.5-1 cm beyond the liver margin; covered by peritoneum. Occasionally has a kink = Phrygian cap deformity (no pathological significance) |
| Body | Largest part; intimately attached to the liver above - the reason gallbladder carcinoma spreads directly into liver early |
| Infundibulum | Transitional region between body and neck; may have a shallow diverticulum on its inferior surface |
| Neck | Short (5-7 mm) tapering portion leading into the cystic duct; lies in the free edge of the hepatoduodenal ligament |
Hartmann's Pouch
A bulging of the inferior infundibulum near the neck. Gallstones can become impacted here, obstructing the cystic duct and triggering acute cholecystitis. Extensive inflammation can cause secondary compression of the adjacent common hepatic duct - this is Mirizzi syndrome.
Spiral Valve of Heister
The mucous membrane of the gallbladder neck forms spiral mucosal folds that constitute the spiral valve of Heister in the cystic duct. This structure regulates flow into and out of the gallbladder.
- Gray's Anatomy for Students
- Sleisenger and Fordtran's
- Yamada's Textbook of Gastroenterology
3. Arterial Supply
The gallbladder is supplied by the cystic artery, which arises most commonly (in ~95% of cases) from the right hepatic artery inside the Triangle of Calot.
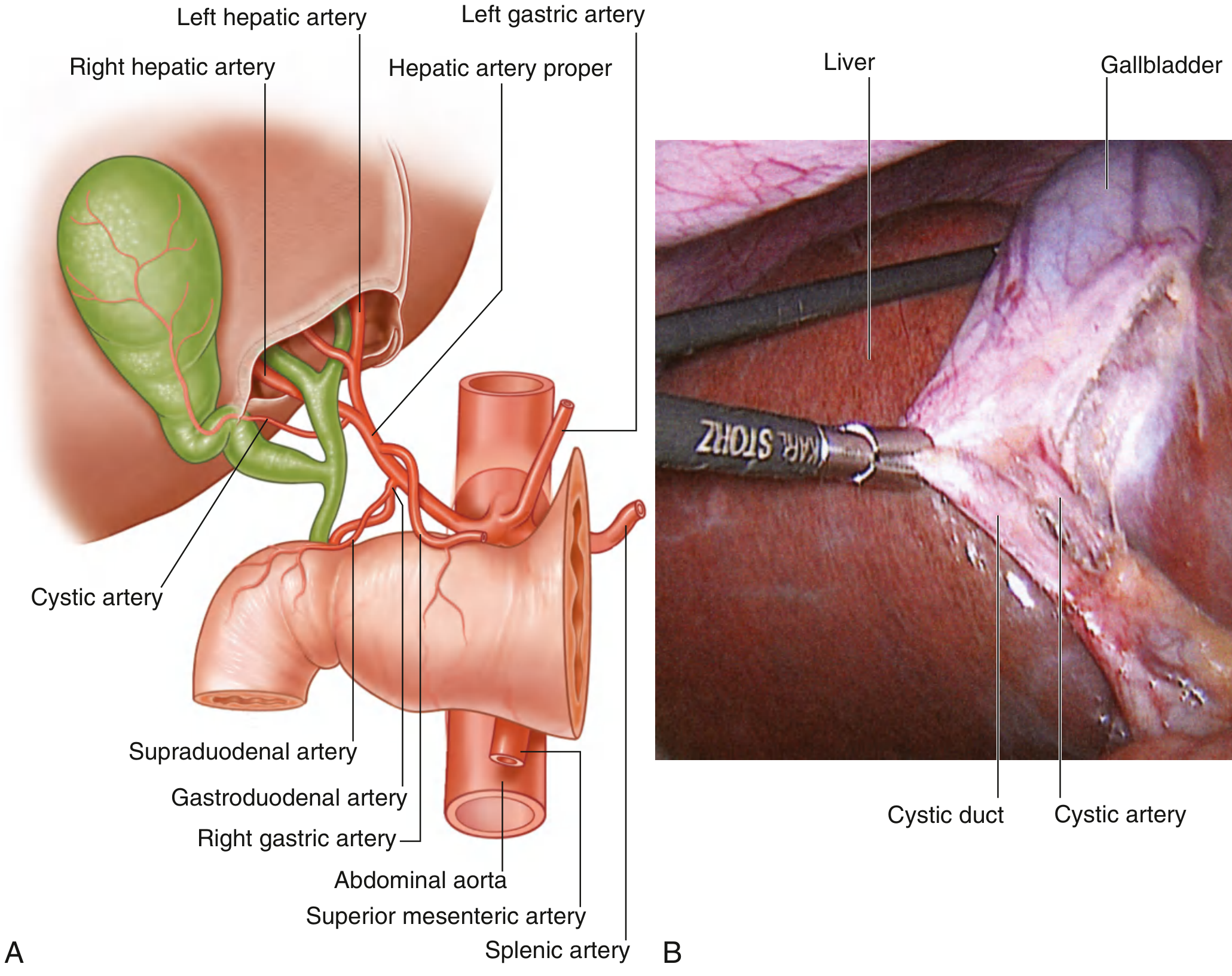
Arterial Supply to the Gallbladder - Gray's Anatomy for Students
Near the neck of the gallbladder, the cystic artery divides into:
- A superficial (peritoneal) branch - supplies the serosal surface
- A deep branch - supplies the layers against the liver
Important: Because the cystic artery is an end artery, the gallbladder is particularly vulnerable to ischemic necrosis with prolonged inflammation or interruption of hepatic arterial flow - this is the mechanism of gangrenous cholecystitis.
Variations are common: the cystic artery may arise from the left hepatic artery, common hepatic artery, gastroduodenal artery, or the superior mesenteric artery. Double/accessory cystic arteries occur in up to 20% of people.
Relations of the gallbladder - Yamada's Textbook of Gastroenterology
4. Venous Drainage
The cystic vein follows the course of the cystic artery initially, then deviates and drains directly into the hepatic sinusoids via the cystic plate / intrahepatic parenchyma to the middle hepatic vein, or occasionally directly into the portal vein. Small veins in the connective tissue between the gallbladder and liver also drain directly into hepatic sinusoids - this is why isolated cystic vein ligation is less predictable surgically.
5. Lymphatic Drainage
Lymphatics from the gallbladder drain through the node of Calot (near the cystic duct), then into:
- Pericholedochal nodes → Portal vein nodes → Superior retropancreatic nodes → Peri-aortic nodes (the major cholecystic-retropancreatic pathway)
- Less commonly, via the cholecystic-celiac pathway along the common hepatic artery to the celiac trunk nodes
This knowledge is critical in staging gallbladder carcinoma: involvement of peri-aortic, pericaval, celiac, or superior mesenteric artery nodes constitutes distant metastasis (M1) per AJCC 8th edition.
6. Innervation
| Type | Source | Function |
|---|---|---|
| Sympathetic | T9 segment → celiac plexus; also right phrenic nerve | Visceral pain - referred to right subcostal, epigastric, and right scapular regions |
| Parasympathetic | Hepatic branch of anterior vagus nerve | Contributes to gallbladder motility regulation |
Visceral pain from the gallbladder travels via sympathetic fibers and is classically referred to the right shoulder/scapula (through the right phrenic nerve) and the epigastrium - which explains the pain pattern in biliary colic.
7. Histology and Microstructure
The gallbladder wall has five layers:
- Epithelium - Simple columnar epithelium with abundant apical microvilli; numerous folds greatly increase the surface area for bile concentration. Tight junctions between lateral membranes separate the lumen from intercellular spaces.
- Lamina propria - Loose connective tissue with elastic fibers, blood vessels, and lymphatics
- Muscularis - Interlocking circular, longitudinal, and oblique smooth muscle fibers (no distinct layers unlike the gut)
- Perimuscular connective tissue - Loose collagen and elastic fibers with larger vessels; contains Rokitansky-Aschoff sinuses - invaginations of surface epithelium that can extend through the muscularis (important in adenomyomatosis and a source of confusion on imaging)
- Serosa - Covers the free surface; absent where the gallbladder is attached to the liver (replaced by adventitia)
Tubuloalveolar glands are found at the neck and infundibulum and produce mucus.
Numerous mitochondria in epithelial cells drive the active transport of NaCl (followed by water) out of the lumen - concentrating bile up to 10-fold during storage.
- Yamada's Textbook of Gastroenterology
8. Physiology
The gallbladder receives, concentrates, and stores bile from the liver:
- Fasting state: The sphincter of Oddi is closed, intraluminal pressure rises, and relaxed gallbladder fills passively.
- Fed state (especially after fat ingestion): Duodenal I-cells release cholecystokinin (CCK), which causes:
- Gallbladder smooth muscle contraction
- Relaxation of the sphincter of Oddi
- Coordinated ejection of concentrated bile into the duodenum
Bile functions to emulsify dietary fats, enabling pancreatic lipase to hydrolyze triglycerides into absorbable fatty acids. Bile acids are then reabsorbed in the terminal ileum and recycled via the enterohepatic circulation.
9. Pathophysiology
A. Cholelithiasis (Gallstone Disease)
Gallstones affect 10-20% of adults in Western countries. There are two main types:
Cholesterol Stones (80% in Western countries)
- Form when bile is supersaturated with cholesterol, exceeding the solubilizing capacity of bile salts and lecithins
- Promoted by:
- Gallbladder hypomotility/stasis (promotes crystal nucleation)
- Mucus hypersecretion (traps crystals, promotes aggregation)
- Estrogen (increases hepatic cholesterol secretion) - explains higher risk in women, with OCP use, and pregnancy
- Obesity, rapid weight loss, metabolic syndrome
- Appear pale yellow to gray-white, ovoid, often faceted (multiple stones); mostly radiolucent (20% may be radiopaque from calcium carbonate)
Pigment Stones (20%)
- Black pigment stones: Form in sterile bile from high unconjugated bilirubin (chronic hemolysis: sickle cell, hereditary spherocytosis; cirrhosis; Crohn disease). Small, numerous, brittle. 50-75% radiopaque.
- Brown pigment stones: Form in infected bile ducts from bacterial phospholipase activity releasing fatty acid salts. Soft, greasy, soaplike. Radiolucent.

Multiple cholesterol gallstones in a gallbladder with chronic cholecystitis wall changes - Robbins & Kumar Basic Pathology
Risk Factors Summary (the "5 F's" + more):
- Fat (obesity), Female, Fertile (pregnancy/OCP), Forty (advancing age), Family history
- Also: rapid weight loss, gallbladder stasis, spinal cord injury, ileal disease (Crohn), total parenteral nutrition
Clinical Features:
- 70-80% remain asymptomatic for decades
- Symptomatic: biliary colic (severe, constant or spasmodic RUQ/epigastric pain, often post-fatty meal as gallbladder contracts against an obstructing stone)
- Complications: empyema, perforation, fistula, cholangitis, obstructive jaundice, pancreatitis
B. Acute Calculous Cholecystitis
Caused by sustained obstruction of the cystic duct by a gallstone, triggering:
- Increased intraluminal pressure
- Bile stasis and mucosal injury from concentrated bile salts
- Secondary bacterial infection (E. coli, Klebsiella, Enterococci)
- Inflammatory cascade: edema, leukocyte infiltration, vascular congestion
Morphology: Enlarged, tense, red-to-violaceous gallbladder; fibrinopurulent exudate on serosa; turbid/purulent bile. Progression: empyema (pus-filled), gangrenous cholecystitis (green-black necrotic wall, from end-artery ischemia).
Clinical presentation: Severe, steady RUQ pain radiating to right shoulder, fever, nausea, leukocytosis, Murphy's sign positive. 25% of patients require surgical intervention.
Complications:
- Bacterial superinfection → cholangitis or sepsis
- Gallbladder perforation → bile peritonitis
- Fistula formation (cholecystoduodenal fistula → gallstone ileus)
- Emphysematous cholecystitis (gas-forming organisms, associated with diabetes)
C. Acute Acalculous Cholecystitis
5-12% of all acute cholecystitis cases. Caused by gallbladder stasis and ischemia in critically ill patients:
- Major surgery, severe trauma, severe burns, sepsis
- Mortality is high due to the underlying conditions
D. Chronic Cholecystitis
Almost always associated with gallstones, but supersaturated bile (rather than stones per se) drives the inflammation. Develops insidiously without prior acute attacks in most cases.
Morphology:
- Variable gallbladder size (contracted, normal, or enlarged)
- Marked subepithelial and subserosal fibrosis
- Lymphocytic infiltration in the wall
- Prominent Rokitansky-Aschoff sinuses
Microorganisms (E. coli, enterococci) cultured in ~1/3 of cases.
E. Gallbladder Carcinoma
A rare but aggressive malignancy, most common primary gallbladder neoplasm. Strongly associated with gallstones (found in 60-90% of cases), chronic inflammation, and gallbladder wall changes.
Growth patterns:
- Infiltrating (more common): Diffuse wall thickening and induration
- Exophytic: Irregular mass growing into the lumen while invading the wall
Histology:
- ~95% adenocarcinoma
- ~5% squamous cell or adenosquamous carcinoma
Clinical features: Symptoms are insidious and mimic cholelithiasis (RUQ pain, jaundice, anorexia, nausea). Preoperative diagnosis in fewer than 20% of patients. Only ~10% are diagnosed early enough for curative resection. Prognosis is poor.
Spread pattern:
-
Direct invasion into the liver (body of gallbladder is fused to liver)
-
Via lymphatics to Calot's node → pericholedochal nodes → para-aortic nodes
-
T-stage determines surgical management:
- T1a: simple cholecystectomy, ~100% 5-year survival
- T1b and beyond: extended resection with liver bed clearance
- T2+: extended cholecystectomy with hepatic segment IVB/V resection + lymphadenectomy
-
Robbins & Kumar Basic Pathology
-
Current Surgical Therapy 14e
F. Other Gallbladder Pathology
| Condition | Key Features |
|---|---|
| Porcelain gallbladder | Calcification of gallbladder wall, associated with chronic cholecystitis. Historical association with carcinoma (now debated) |
| Gallbladder polyps | Cholesterol polyps most common (pseudopolyps); true adenomas rare. Polyps >10 mm warrant cholecystectomy due to malignancy risk |
| Adenomyomatosis | Hyperplastic change with Rokitansky-Aschoff sinus overgrowth; can mimic cancer on imaging |
| Cholesterolosis | "Strawberry gallbladder" - cholesterol deposits in the mucosa |
| Primary sclerosing cholangitis | Can involve intrahepatic and extrahepatic biliary tree including gallbladder |
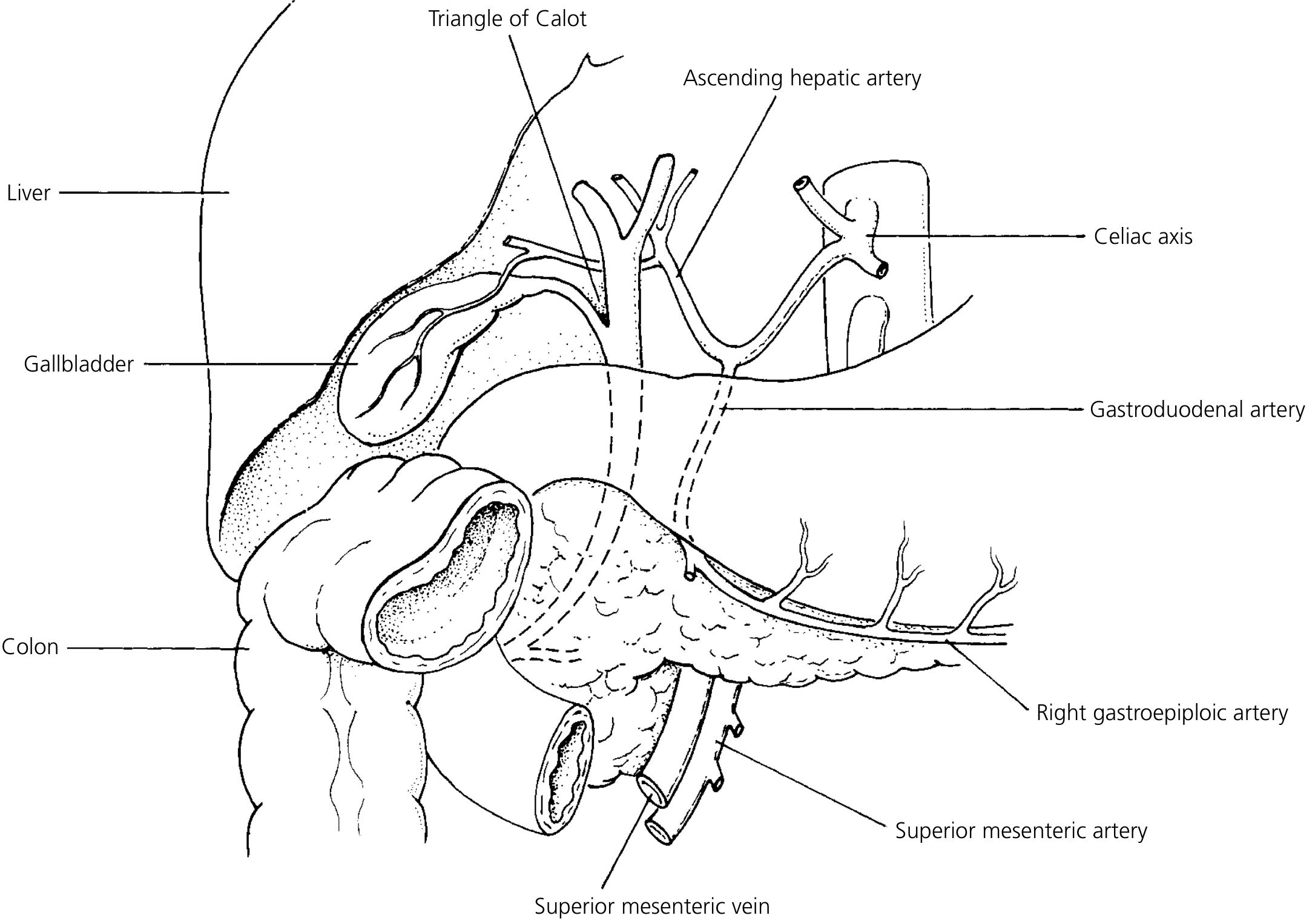
10. Triangle of Calot - Surgical Significance
The Triangle of Calot (hepatocystic triangle) is bounded by:
- Superiorly: inferior surface of the liver
- Medially: common hepatic duct
- Laterally: cystic duct
The cystic artery runs within this triangle before reaching the gallbladder. Correctly identifying and dissecting this triangle is essential in laparoscopic cholecystectomy to avoid inadvertent bile duct injury, which remains the most serious complication of the procedure.
Sources: Gray's Anatomy for Students | Yamada's Textbook of Gastroenterology, 7e | Robbins & Kumar Basic Pathology | Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Current Surgical Therapy 14e
This is a shared conversation. Sign in to Orris to start your own chat.