Explain Bp
Reading File
Finding Sources
Searching the Web
blood pressure physiology regulation determinants
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Explain ECg cases to p10 woth diagram and show the poonts where it changes
Asking for Preferences
Reading File
Finding Sources
Searching Images
ECG waveform anatomy P wave QRS complex T wave intervals labeled diagram
Loading Image
Loading Image
Finding Sources
Finding Sources
Searching Images
normal sinus rhythm ECG strip labeled with P wave PR interval QRS ST T wave
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Now I have everything I need to give a comprehensive, well-illustrated explanation. Let me put it all together.
📈 ECG Basics — Waveform Anatomy (P1 to P10)
The Master Diagram
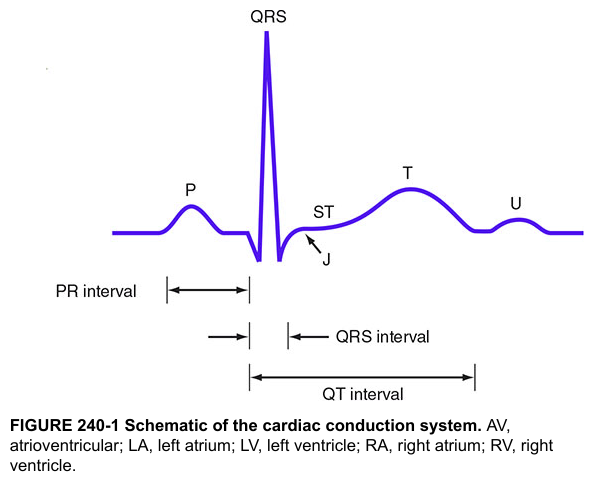
Here are two authoritative labeled ECG diagrams showing every key component:
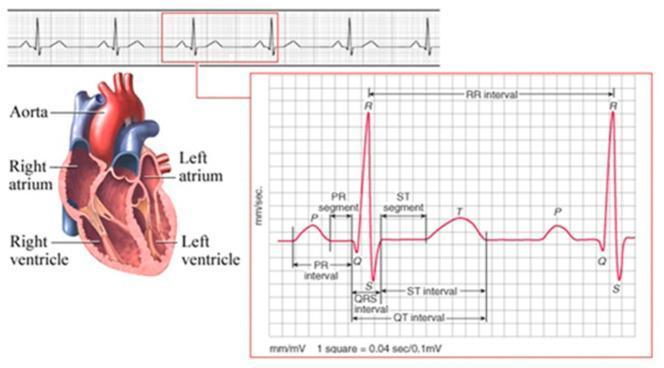
Understanding the Grid
Before reading any waveform, understand the paper:
| Dimension | Value |
|---|---|
| 1 small box (horizontal) | 0.04 seconds |
| 1 large box (horizontal) | 0.20 seconds |
| 1 small box (vertical) | 0.1 mV |
| Standard paper speed | 25 mm/sec |
P1 — The P Wave (Atrial Depolarization)
What it is: The first small, rounded upward hump before the QRS.
Represents: Electrical depolarization spreading from the SA node across both atria.
"Depolarization of the atria begins in the sinus node and spreads in all directions over the atria... This record of atrial depolarization is known as the atrial P wave." — Guyton & Hall Textbook of Medical Physiology
| Feature | Normal Value |
|---|---|
| Duration | < 0.12 sec (3 small boxes) |
| Amplitude | < 2.5 mm |
| Polarity | Upright in leads I, II, aVF |
Where it changes: Absent P wave → atrial fibrillation or severe hyperkalemia. Inverted P wave → ectopic atrial rhythm (impulse coming from below, not from SA node).
P2 — The PR Segment
What it is: The flat line from the end of the P wave to the start of the QRS.
Represents: Time the impulse is held at the AV node (physiological delay to allow ventricular filling).
"The P wave is generated by atrial depolarization, the QRS by ventricular muscle depolarization, and the T wave by ventricular repolarization. Thus, the PR interval is a measure of conduction time from atrium to ventricle." — Katzung's Basic & Clinical Pharmacology
P3 — The PR Interval
What it is: From the start of the P wave to the start of the QRS.
Represents: Total atrial → AV node → His-Purkinje conduction time.
| Feature | Normal Value |
|---|---|
| Duration | 0.12 – 0.20 sec (3–5 small boxes) |
Where it changes:
- Long PR (>0.20 s) → 1st degree AV block (slow AV conduction)
- Short PR (<0.12 s) → Pre-excitation (WPW syndrome) or accelerated AV conduction
- Lengthening PR then dropped beat → 2nd degree (Mobitz I) block
P4 — The Q Wave
What it is: The first downward deflection of the QRS complex.
Represents: Initial septal depolarization (left → right through the interventricular septum).
| Feature | Normal (Septal) | Pathological |
|---|---|---|
| Duration | < 0.04 sec (1 small box) | ≥ 0.04 sec |
| Depth | < 25% of R wave height | ≥ 25% of R wave height |
Where it changes: A pathological Q wave (deep, wide) = marker of prior myocardial infarction (dead myocardium produces no electrical force).
P5 — The R Wave
What it is: The tall, sharp upward spike — the dominant feature of the QRS.
Represents: Depolarization of the bulk of ventricular muscle (mainly left ventricle).
Normal R-wave progression (V1 → V6):
- V1: Small R, large S
- V3–V4: R and S roughly equal (transition zone)
- V5–V6: Tall R, small S
Where it changes: Loss of R-wave progression (poor R-wave progression = anterior MI or LBBB).
P6 — The S Wave
What it is: The downward deflection after the R wave.
Represents: Terminal depolarization of the basal portions of the ventricles.
Where it changes: Broad, slurred S wave in leads I, aVL, V5–V6 → Right Bundle Branch Block (RBBB). RSR' (M-shaped) pattern in V1 is the hallmark.
P7 — The QRS Complex (Combined)
What it is: Q + R + S together as one unit.
Represents: Complete ventricular depolarization.
| Feature | Normal Value |
|---|---|
| Duration | < 0.12 sec (3 small boxes) |
"The total duration of the QRS complex is similar to that of the P wave. This fact may seem surprising because the ventricles are so much larger than the atria; however, the ventricles depolarize just as quickly because conduction velocity in the His-Purkinje system is much faster than in the atrial conducting system." — Costanzo Physiology
Where it changes:
- Wide QRS (>0.12 s) → Bundle branch block, ventricular rhythm, hyperkalemia, or pre-excitation
- Low voltage QRS → Pericardial effusion, obesity, hypothyroidism
P8 — The ST Segment
What it is: The flat line from the end of the QRS (J point) to the start of the T wave.
Represents: The plateau phase of the ventricular action potential — all ventricular cells are depolarized and no net current flows → isoelectric line.
| Feature | Normal Value |
|---|---|
| Position | Isoelectric (at baseline) |
| Deviation | < 1 mm elevation or depression |
Where it changes (most clinically critical):
| Change | Significance |
|---|---|
| ST elevation ≥ 1 mm (≥2 leads) | STEMI (acute transmural MI) |
| ST depression | Subendocardial ischemia, NSTEMI |
| Diffuse ST elevation (saddle-shaped) | Pericarditis |
| ST elevation in V1–V4 (concave up) | Benign early repolarization |
P9 — The T Wave (Ventricular Repolarization)
What it is: A rounded, broader hump after the ST segment.
Represents: Ventricular repolarization (recovery of electrical charge).
| Feature | Normal Value |
|---|---|
| Polarity | Same direction as QRS (concordant) |
| Amplitude | < 5 mm limb leads; < 10 mm precordial |
"The T wave represents repolarization of the ventricles." — Costanzo Physiology
Where it changes:
- Hyperacute T waves (tall, peaked) → Earliest sign of STEMI; also severe hyperkalemia
- T wave inversion → Ischemia, RBBB, LVH (strain pattern), PE (V1–V4)
- Flat T waves → Hypokalemia, digoxin effect, ischemia
P10 — The QT Interval
What it is: From the start of the QRS to the end of the T wave.
Represents: Total duration of ventricular depolarization + repolarization (entire electrical systole).
| Feature | Normal Value |
|---|---|
| Duration | 0.35 – 0.45 sec (rate-dependent) |
| Corrected QTc | < 440 ms men; < 460 ms women |
"The QT interval is an index of the length of the overall ventricular action potential; duration depends on heart rate because the action potential shortens with increased heart rate." — Medical Physiology (Boron & Boulpaep)
Where it changes:
- Prolonged QT → Risk of Torsades de Pointes (polymorphic VT) → caused by drugs (quinidine, haloperidol, macrolides), hypokalemia, hypomagnesemia, congenital long QT syndrome
- Short QT → Hypercalcemia, digoxin toxicity
Summary Table — All 10 Points at a Glance
| Point | Component | Represents | Normal Duration/Value | Key Change |
|---|---|---|---|---|
| P1 | P wave | Atrial depolarization | < 0.12 s | Absent = AF / hyperkalemia |
| P2 | PR segment | AV node delay | Flat, isoelectric | Depression = atrial ischemia |
| P3 | PR interval | Atrio-ventricular conduction | 0.12–0.20 s | Long = heart block; Short = WPW |
| P4 | Q wave | Septal depolarization | < 0.04 s, < 25% R | Wide/deep = old MI |
| P5 | R wave | Ventricular depolarization (bulk) | Progresses V1→V6 | Poor progression = anterior MI |
| P6 | S wave | Terminal ventricular depolarization | Small in lateral leads | Wide/slurred = RBBB |
| P7 | QRS complex | Total ventricular depolarization | < 0.12 s | Wide = BBB, VT, hyperkalemia |
| P8 | ST segment | Ventricular plateau | Isoelectric | Elevation = STEMI; Depression = ischemia |
| P9 | T wave | Ventricular repolarization | Concordant, < 10 mm | Peaked = hyperkalemia; Inverted = ischemia |
| P10 | QT interval | Total ventricular electrical cycle | 0.35–0.45 s (QTc < 440 ms) | Prolonged = Torsades de Pointes risk |
Sources: Guyton & Hall Textbook of Medical Physiology | Costanzo Physiology 7th Ed | Medical Physiology (Boron & Boulpaep) | Katzung's Basic & Clinical Pharmacology | Harrison's Principles of Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.