Explain myopia. Uh, with its simple clinical and pathological myopias and causes. And fundus examination. And briefly explain all the above things. Of myopia. And what... Lent should be used to treat it. Okay. Where the retinas are formed. Everything.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
I have excellent content from the textbooks. Now I have everything needed to write a comprehensive answer on myopia. Let me compose the full response.
Myopia (Short-sightedness / Near-sightedness)
What Is Myopia?
Myopia is a refractive error in which parallel rays of light from a distant object are focused in front of the retina (instead of on it) when the eye is at rest. The result is blurry distance vision but clear near vision. It is caused by a mismatch between the optical power of the eye and its axial length.
Types of Myopia
1. Simple (Physiological) Myopia
- The most common form. The eye is anatomically normal but falls at the far end of the normal distribution of refractive errors.
- Typically develops in school-age children (hence also called "school myopia"), stabilizes in the early 20s.
- Usually < -6.00 diopters (D); axial length is only mildly increased.
- No structural ocular damage or pathological changes on fundus.
- Strong association with near-work (prolonged reading, screens) and reduced time outdoors in sunlight.
2. Pathological (Degenerative / High) Myopia
- Defined as > -6.00 D, with axial length typically > 26 mm.
- Characterized by progressive anteroposterior elongation of the scleral envelope beyond what is needed for emmetropia.
- Not simply a refractive variant - there is structural damage due to mechanical stretching of the retina, choroid, and sclera.
- A significant cause of legal blindness; maculopathy is the most common cause of visual loss.
- Affects >2% of Western populations and up to ~10% in East Asians.
Causes / Etiology
Axial myopia (most common): The eyeball is too long - the most frequent mechanism.
Refractive myopia: The refracting power of the eye is too strong (e.g., a steep cornea or dense lens).
Contributing / risk factors:
-
Genetic: Strong hereditary component; autosomal dominant patterns seen.
-
Environmental: Long-term intensive near visual activity (reading, computers, screens).
-
Systemic associations of high myopia:
- Down syndrome
- Marfan syndrome
- Stickler syndrome
- Ehlers-Danlos syndrome
- Prematurity (ROP-related)
- Noonan syndrome
- Pierre-Robin syndrome
-
Medications causing transient myopia: miotics, sulfa drugs, tetracycline.
-
Nuclear sclerosis of the lens (lens-induced myopia - increases refractive index).
(Wills Eye Manual; Kanski's Clinical Ophthalmology 10th ed.)
Where Is the Image Formed?
In myopia, the image of a distant object falls in front of the retina - within the vitreous cavity - because the axial length is too long or the eye's optical power is too strong. For close objects, the focal point moves back toward the retina, which is why myopes see near objects clearly without glasses.
Fundus Examination Findings
Simple Myopia
Fundus is essentially normal. No structural pathology is expected.
Pathological / High Myopia - Key Fundus Signs
Critical findings (Wills Eye Manual):
- Myopic crescent: A crescent-shaped area of white sclera or exposed choroidal vessels adjacent to the optic disc, separated from normal-appearing fundus by a hyperpigmented line.
- Tilted/oblique optic disc: With or without vertical elongation.
- Macular pigmentary abnormalities.
- Fuchs spot: A raised, circular, pigmented lesion at the macula, developing after a subretinal hemorrhage has been absorbed.
- Refractive correction typically > -6.00 D, axial length ≥ 26 mm.
Other findings (Kanski's + Wills):
- Tessellated (tigroid) fundus: Pale, tiger-stripe appearance due to attenuation of the RPE with visibility of large underlying choroidal vessels.
- Focal chorioretinal atrophy: Patchy visibility of choroidal vessels, sometimes sclera.
- Lacquer cracks: Fine, irregular yellow lines criss-crossing the posterior pole - ruptures in the RPE-Bruch membrane-choriocapillaris complex (~5% of high myopia eyes). Can lead to macular neovascularization (MNV).
- Subretinal "coin" hemorrhages: May develop from lacquer cracks without MNV.
- Posterior staphyloma: Focal posterior scleral ectasia (macular or peripapillary), present in ~1/3 of pathological myopia eyes.
- Lattice degeneration (peripheral).
- Peripapillary atrophy: Common temporal crescent of absent RPE.
- Choroidal neovascularization (MNV/CNV): Occurs in ~10% of highly myopic eyes.
- Rhegmatogenous retinal detachment (RRD): Much more common in high myopia.
- Temporal optic disc pallor.
- Visual field defects (arcuate scotoma, generalized constriction).
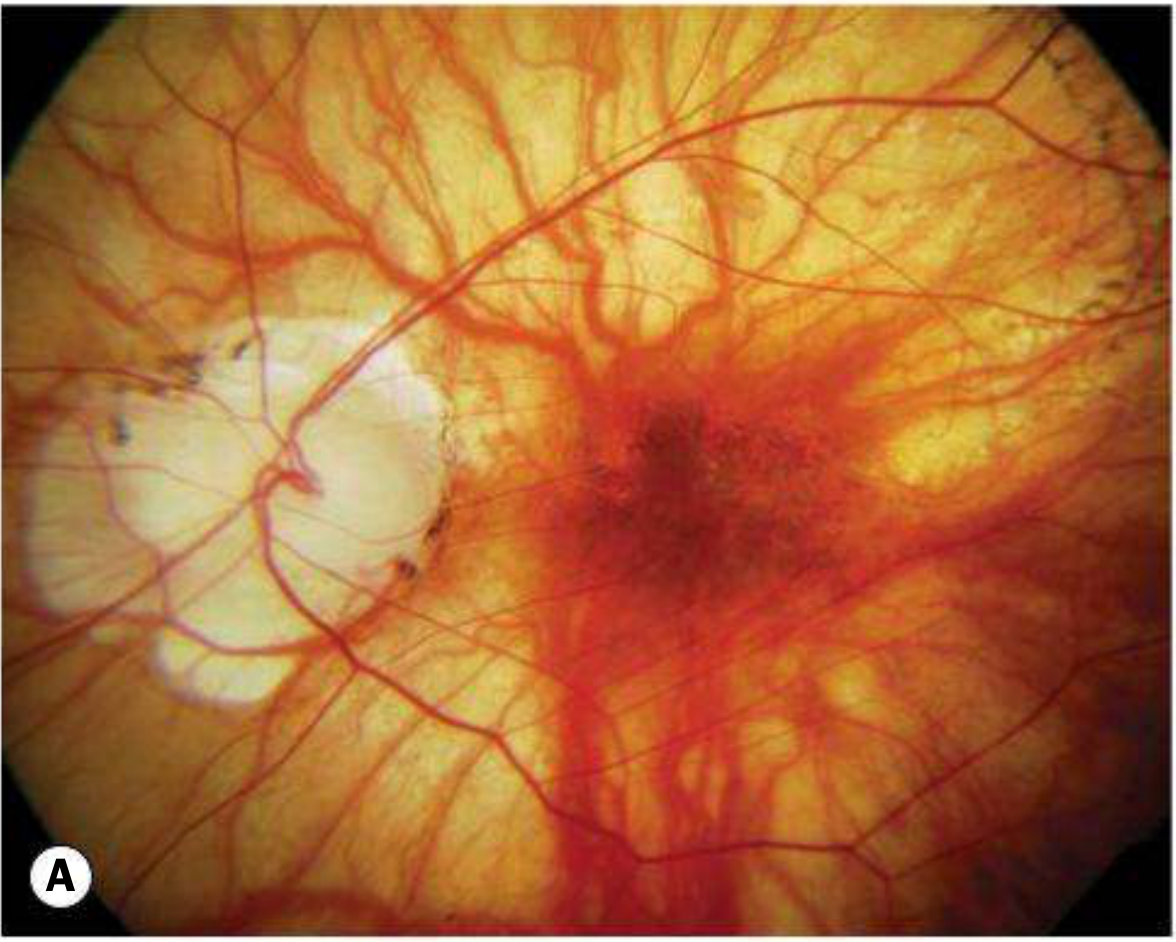
Fundus image - High myopia with macular hemorrhage (Wills Eye Manual):

Fundus image - Tessellated fundus with large peripapillary crescent in pathological myopia (Kanski's):
Workup
- Retinoscopy to estimate the refractive error (axial myopia).
- Dilated fundus examination with indirect ophthalmoscopy + scleral depression to search for retinal breaks or detachment.
- Slit-lamp biomicroscopy with 60 D or 90 D lens or fundus contact lens for posterior pole detail.
- OCT: For macular pathology, staphyloma, subretinal fluid, MNV.
- A-scan biometry for axial length measurement.
Treatment - What Lens Is Used?
Lens Correction (Optical)
Myopia is corrected with a concave (diverging) lens - i.e., a minus (-) powered lens. This diverges the incoming light rays before they enter the eye, so the focal point moves back onto the retina.
- Glasses or contact lenses with minus (-) diopter power are prescribed.
- Example: A patient with -3.00 D myopia gets -3.00 D concave lens.
Surgical Options (Kanski's)
| Method | Indication |
|---|---|
| Surface ablation (PRK/LASEK) | Low-to-moderate myopia |
| LASIK | Moderate-to-high myopia (depends on corneal thickness) |
| SMILE (small-incision lenticule extraction) | Myopia and myopic astigmatism |
| Phakic posterior chamber implant (ICL) | Very high myopia; lens inserted behind iris, in front of crystalline lens; power range -3 D to -20.5 D |
| Iris-clip (lobster-claw) implant | Anterior chamber phakic IOL for very high myopia |
| Clear lens exchange | Very high myopia; risk of RD post-op |
Myopia Progression Control
- Low-dose atropine 0.01% at bedtime significantly slows progression in children (ages 5-15) whose myopia increases >1 D/year.
- Multifocal soft contact lenses (+2.50 D add, centre-distance) in children 7-11 years with < 5 D myopia (BLINK trial showed dose-dependent slowing).
- Spend time outdoors in sunlight - reduces progression rate in children.
Summary Table
| Feature | Simple Myopia | Pathological Myopia |
|---|---|---|
| Degree | < -6 D | > -6 D |
| Axial length | Mildly increased | > 26 mm |
| Fundus | Normal | Multiple degenerative changes |
| Progression | Stops in 20s | Progressive (lifelong) |
| Risk of RD, CNV | Low | Significantly raised |
| Treatment | Concave lens | Concave lens + surgical options |
| Progression control | Atropine 0.01%, multifocals | Monitor, anti-VEGF for CNV |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed.; The Wills Eye Manual, 8th ed.
I sincerely apologize. I forgot to mention that the myopia which I am telling you to explain for the BSc Allied Health Science, Kailajini Arena University of Health Science. So, it was an humble request. If you please explain the above, uh, myopia, uh, functions, deficiency, causes, examinations for the BSc Allied Health Science.
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I have all the material needed. Here are your complete, exam-ready BSc Allied Health Science notes on Myopia.
MYOPIA
BSc Allied Health Science - Complete Study Notes
Kailajini Arena University of Health Science
1. DEFINITION
Myopia (also called short-sightedness or near-sightedness) is a refractive error of the eye in which parallel light rays coming from a distant object are focused in front of the retina instead of directly on it, when the eye is at rest (not accommodating).
- The person sees near objects clearly but distant objects appear blurry.
- It is written with a minus (-) sign in prescriptions (e.g., -2.00 D, -5.00 D).
2. NORMAL EYE vs. MYOPIC EYE - How the Image is Formed
| Feature | Normal Eye (Emmetropia) | Myopic Eye |
|---|---|---|
| Focal point | Exactly on the retina | In front of the retina |
| Axial length | ~24 mm | Longer (>24 mm, up to 26+ mm in high myopia) |
| Vision | Clear at all distances | Clear near, blurry far |
Simple rule to remember: The eyeball is "too long" (or the lens/cornea is "too curved"), so light rays converge too early - before reaching the retina.
3. TYPES OF MYOPIA
A. Simple (Physiological / School) Myopia
- Most common type.
- The eye is structurally normal - it just falls at the "long" end of the normal distribution.
- Typically starts in school-going children (age 7-14 years) and stabilizes in the early 20s.
- Refractive error is usually less than -6.00 diopters (D).
- No structural damage to the retina or other ocular structures.
- Caused mainly by genetics + near-work (reading, screens).
B. Pathological (Degenerative / High) Myopia
- Refractive error is greater than -6.00 D.
- Axial length is > 26 mm (eye is abnormally long).
- The eye continuously elongates, even into adulthood - it does not stop progressing.
- The stretching of the eye wall causes damage to the retina, choroid, and other structures.
- A significant cause of legal blindness worldwide.
- More common in East Asian populations (up to 10%) than in Western populations (2%).
4. CAUSES OF MYOPIA
A. Causes by Mechanism
| Mechanism | Explanation |
|---|---|
| Axial myopia | Eyeball is too long (most common mechanism) |
| Refractive myopia | Cornea or lens is too curved/powerful, bends light too strongly |
| Index myopia | Increased refractive index of the lens (e.g., nuclear cataract, diabetes) |
B. Risk Factors and Contributing Causes
Genetic / Hereditary:
- Strong family history increases risk significantly.
- If both parents are myopic, the child has a much higher risk.
Environmental:
- Prolonged near-work (reading, writing, using computers/phones/tablets).
- Reduced time outdoors in natural sunlight (sunlight triggers dopamine release in the retina, which normally slows eye growth).
Systemic Diseases associated with High Myopia:
- Down syndrome
- Marfan syndrome
- Stickler syndrome
- Ehlers-Danlos syndrome
- Prematurity (Retinopathy of Prematurity)
- Noonan syndrome
- Pierre-Robin syndrome
Medications (drug-induced transient myopia):
- Miotic eye drops
- Sulfa drugs
- Tetracycline
(Kanski's Clinical Ophthalmology 10th ed.)
5. CLINICAL FEATURES (Symptoms)
These are what the patient complains of:
| Symptom | Explanation |
|---|---|
| Blurred distant vision | Cannot see the board, television, or distant faces clearly |
| Clear near vision | Can read a book or see close objects without difficulty |
| Squinting/narrowing eyes | Patient squints to see far (acts as a pinhole, improving focus temporarily) |
| Eye strain / headache | Due to effort to focus on distant objects |
| Floaters | In high myopia, due to vitreous degeneration |
| Flashes of light | In high myopia, may indicate retinal traction or detachment |
| Gradual progression in childhood | Increasing need for stronger glasses year by year |
6. PATHOLOGICAL CHANGES IN HIGH MYOPIA
In high/pathological myopia, the eye undergoes progressive stretching, causing the following structural damage:
| Structure | Pathological Change |
|---|---|
| Sclera | Thinning and elongation; posterior staphyloma (outpouching of the back of the eye) |
| Retina | Thinning, lattice degeneration, atrophic holes, retinal detachment |
| Choroid | Atrophy, choroidal neovascularization (new abnormal blood vessels) |
| RPE (Retinal Pigment Epithelium) | Atrophy - causes tessellated appearance |
| Bruch's Membrane | Ruptures - seen as "lacquer cracks" |
| Lens | Posterior subcapsular cataract; nuclear sclerosis worsens myopia |
| Optic disc | Tilted, abnormally shaped; peripapillary atrophy |
7. FUNDUS EXAMINATION FINDINGS
The fundus is the back of the eye (retina, optic disc, macula, blood vessels) seen using an ophthalmoscope.
Simple Myopia:
Fundus appears completely normal. No structural changes.
Pathological / High Myopia - Fundus Signs:
Critical (Most Important) Signs:
- Myopic Crescent - A crescent-shaped pale area of white sclera or visible choroidal vessels next to the optic disc. The crescent is separated from the normal fundus by a dark (hyperpigmented) line.
- Tilted / Oblique Optic Disc - The optic disc appears tilted or slanted, not round and straight.
- Fuchs Spot - A raised, dark, pigmented spot at the macula. Forms after a subretinal bleed absorbs. Indicates severe macular damage.
- Macular pigmentary changes - Irregular pigmentation at the macula.
Other Important Signs:
- Tessellated (Tigroid) Fundus - The fundus has a pale, tiger-stripe appearance because the RPE is thin and the large choroidal vessels beneath are visible.
- Lacquer Cracks - Fine, irregular yellow lines criss-crossing the posterior pole. These are ruptures in Bruch's membrane. Found in about 5% of high myopia eyes. Can lead to bleeding and choroidal neovascularization (CNV/MNV).
- Subretinal Coin Hemorrhage - Small round bleed under the retina from a lacquer crack.
- Posterior Staphyloma - An ectasia (outpouching) of the back of the eye at the macula or around the optic disc.
- Chorioretinal Atrophy - Patchy loss of RPE and choroid; sclera may be visible underneath.
- Lattice Degeneration - Peripheral retinal thinning with a criss-cross pattern; risk of retinal tear.
- Retinal Detachment - Much more common in high myopia.
- Temporal optic disc pallor - The temporal side of the disc looks pale.
Fundus Image 1 - High Myopia with Macular Hemorrhage (Wills Eye Manual):
Note the large dark macular hemorrhage (Fuchs spot precursor) and the pale peripapillary crescent to the right, with a relatively flat/pale optic disc.
Fundus Image 2 - Tessellated Fundus with Large Peripapillary Crescent (Kanski's):
Note the large white peripapillary crescent (left side) indicating peripapillary atrophy, and the overall pale-yellow tessellated appearance of the fundus due to RPE thinning.
8. EXAMINATION / INVESTIGATIONS
As an Allied Health Science student, you should know these steps:
| Investigation | What It Does |
|---|---|
| Visual acuity testing (Snellen chart) | Measures how blurry the distance vision is |
| Retinoscopy | Objective measurement of refractive error; detects axial myopia |
| Subjective refraction | Patient confirms the best correcting lens |
| Slit-lamp examination | Examines the front of the eye (cornea, lens, anterior chamber) |
| Dilated fundus examination | Indirect ophthalmoscopy + scleral depression to check for retinal breaks or detachment |
| OCT (Optical Coherence Tomography) | High-resolution imaging of the macula and retinal layers |
| A-scan biometry | Measures axial length of the eyeball |
| Visual field testing | Checks for peripheral vision loss |
9. LENS USED FOR TREATMENT
Myopia is corrected with a CONCAVE (DIVERGING) lens - i.e., a MINUS (-) lens.
Why a Concave Lens?
In myopia, the eye's focusing power is too strong. A concave lens diverges (spreads out) the light rays before they enter the eye. This effectively moves the focal point backward - from in front of the retina, back onto the retina where it belongs.
Distant object → Light rays → Concave (-) lens diverges them →
Eye converges them → Image falls ON the retina → Clear vision ✓
Types of Corrections:
1. Spectacles (Glasses)
- Concave lenses (minus power, e.g., -1.00 D to -20.00 D).
- Simplest, safest, and most affordable.
2. Contact Lenses
- Soft or rigid gas-permeable concave contact lenses.
- Worn directly on the cornea.
3. Surgical Corrections (for permanent treatment):
| Surgery | Used For |
|---|---|
| PRK / Surface ablation | Low to moderate myopia |
| LASIK (Laser-Assisted In-Situ Keratomileusis) | Moderate to high myopia; reshapes the cornea with laser |
| SMILE (Small Incision Lenticule Extraction) | Myopia and myopic astigmatism |
| ICL (Implantable Collamer Lens / Phakic IOL) | Very high myopia (-3D to -20.5D); lens inserted behind iris in front of natural lens |
| Clear Lens Exchange | Very high myopia; the natural lens is replaced |
(Kanski's Clinical Ophthalmology 10th ed.)
10. MANAGEMENT / SLOWING PROGRESSION
| Method | Details |
|---|---|
| Low-dose Atropine 0.01% eye drops | Given at bedtime; significantly slows myopia progression in children aged 5-15 years with progression > 1 D/year |
| Multifocal contact lenses | +2.50 D add, centre-distance soft lens for children 7-11 years with < 5D myopia (BLINK trial) |
| Spend time outdoors | Sunlight stimulates retinal dopamine, which normally inhibits excessive eye growth |
| Anti-VEGF injections | For choroidal neovascularization (CNV) in pathological myopia |
| Safety eyewear | Polycarbonate goggles during sport - high myopia eyes are at risk of choroidal rupture |
11. COMPLICATIONS OF HIGH MYOPIA
| Complication | Notes |
|---|---|
| Retinal detachment | Much more common; watch for sudden floaters + flashes |
| Macular degeneration | Myopic maculopathy - leading cause of blindness in high myopia |
| Choroidal neovascularization | Abnormal vessels grow under retina; causes sudden central vision loss |
| Glaucoma | Increased risk; visual field loss may mimic glaucoma |
| Cataract | Posterior subcapsular or nuclear type |
| Amblyopia (lazy eye) | If myopia is unequal between the two eyes and uncorrected in childhood |
QUICK REVISION TABLE - Exam Memory Aid
| Point | Key Fact |
|---|---|
| Definition | Light focuses in front of the retina |
| Simple myopia | < -6 D, no structural damage, stops in 20s |
| Pathological myopia | > -6 D, axial length > 26 mm, progressive, causes blindness |
| Main cause | Axial elongation of the eyeball |
| Lens used | Concave (minus, diverging) lens |
| Fundus in simple | Normal |
| Fundus in high myopia | Myopic crescent, tessellated fundus, lacquer cracks, Fuchs spot, staphyloma |
| Most common cause of blindness in high myopia | Maculopathy |
| Progression control in children | Atropine 0.01% + outdoor time |
| Retinal image position | In front of the retina (in the vitreous) |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition | The Wills Eye Manual, 8th Edition
This is a shared conversation. Sign in to Orris to start your own chat.