Prepare comprehensive MD Medicine notes on Junctional Rhythm The notes should be structured with clear headings, tables, ECG diagrams, algorithms, and clinical pearls. Add ecg ( more and more example if needed use google ecg not only books) Cover the following topics in detail: 1. Definition * Definition of junctional rhythm * Anatomy and physiology of the AV junction * Normal pacemaker hierarchy * Escape rhythm vs accelerated rhythm 2. Electrophysiology * Automaticity of AV junction * Escape mechanism * Enhanced automaticity * Re-entry mechanism * Influence of sympathetic and parasympathetic tone 3. Classification Add each ecg example and clinical significance. * Junctional escape rhythm (40–60 bpm) * Accelerated junctional rhythm (60–100 bpm) * Junctional tachycardia (>100 bpm) * Non-paroxysmal junctional tachycardia * Congenital junctional ectopic tachycardia * Postoperative junctional ectopic tachycardia 4. Etiology Categorize causes into: * Physiological * Increased vagal tone * Sick sinus syndrome * Sinus arrest * SA exit block * AV block * Inferior wall MI * Myocarditis * Cardiac surgery * Digoxin toxicity * Beta-blockers * Calcium channel blockers * Amiodarone * Electrolyte disturbances * Hypoxia * Hyperkalemia * Sleep apnea * Congenital heart disease * Idiopathic Present causes in an easy-to-remember table. 5. ECG Diagnosis (Very Detailed) Explain stepwise ECG interpretation. Include labeled ECG diagrams for: * Normal junctional escape rhythm * Accelerated junctional rhythm * Junctional tachycardia * Retrograde P waves * Inverted P before QRS * Hidden P wave * P wave after QRS * Simultaneous P wave within QRS Explain: * Heart rate * Rhythm regularity * QRS duration * PR interval * RP interval * Retrograde atrial activation * AV dissociation * Capture beats * Fusion beats Draw multiple ECG strips showing every pattern. 6. ECG Differential Diagnosis Compare junctional rhythm with: * Sinus bradycardia * Sinus arrest * SA exit block * Low atrial rhythm * AVNRT * AVRT * Atrial tachycardia * Ventricular escape rhythm * Idioventricular rhythm * Complete heart block * Accelerated idioventricular rhythm Provide comparison tables. 7. Clinical Features * Symptoms * Signs * Hemodynamic effects * Cannon A waves * Syncope * Presyncope * Palpitations * Heart failure * Cardiogenic shock 8. Diagnostic Evaluation History Physical examination Laboratory investigations: * CBC * Electrolytes * Calcium * Magnesium * Thyroid profile * Troponin * Digoxin level * ABG Cardiac investigations: * Serial ECG * Holter * Event recorder * Telemetry * Echocardiography * Exercise testing * Electrophysiology study * Cardiac MRI * Coronary angiography (when indicated) 9. Approach to Junctional Rhythm Create a flowchart: Patient → ECG → Stable/Unstable → Identify reversible cause → Treatment → Need for pacing → Follow-up 10. Acute Management According to ACC/AHA/ESC guidelines. Differentiate: * Stable patient * Unstable patient Include: * Oxygen * IV access * Monitoring * Atropine * Dopamine * Epinephrine * Isoproterenol * Temporary pacing * Transcutaneous pacing * Transvenous pacing Explain indications and contraindications. 11. Long-Term Treatment * Treat underlying cause * Medication adjustment * Permanent pacemaker indications * Catheter ablation * Follow-up strategy 12. Drug-Induced Junctional Rhythm Explain mechanisms and management of: * Digoxin * Beta-blockers * Calcium channel blockers * Amiodarone * Ivabradine * Adenosine 13. Junctional Rhythm in Special Situations * Inferior wall MI * Digoxin toxicity * Cardiac surgery * Congenital heart disease * Athletes * Pregnancy * Pediatric patients * ICU patients * Electrolyte abnormalities 14. Complications * Syncope * Heart failure * Hypotension * AV dyssynchrony * Reduced cardiac output * Progression to complete heart block 15. Prognosis * Benign vs pathological junctional rhythm * Prognostic factors
junctional rhythm ECG examples labeled strips retrograde P wave accelerated junctional
"junctional rhythm" AND management
accelerated junctional rhythm ECG strip 12 lead digoxin toxicity junctional tachycardia site:litfl.com OR site:ecgwaves.com OR site:ecglibrary.com
junctional ectopic tachycardia postoperative congenital ECG pediatric pacemaker hierarchy cardiac conduction system
junctional rhythm ECG AV dissociation complete heart block vs junctional escape comparison digoxin toxicity ECG
~/junctional-rhythm-notes/Junctional_Rhythm_MD_Notes.md
# JUNCTIONAL RHYTHM
## Comprehensive MD Medicine Notes
> **Prepared for MD Medicine Examination**
> Sources: Tintinalli's Emergency Medicine, Harrison's Principles of Internal Medicine (22E), Rosen's Emergency Medicine, Harriet Lane Handbook, Frameworks for Internal Medicine, LITFL ECG Library, StatPearls
---
# TABLE OF CONTENTS
1. [Definition and Anatomy](#1-definition-and-anatomy)
2. [Electrophysiology](#2-electrophysiology)
3. [Classification](#3-classification)
4. [Etiology](#4-etiology)
5. [ECG Diagnosis](#5-ecg-diagnosis)
6. [ECG Differential Diagnosis](#6-ecg-differential-diagnosis)
7. [Clinical Features](#7-clinical-features)
8. [Diagnostic Evaluation](#8-diagnostic-evaluation)
9. [Approach Algorithm](#9-approach-algorithm)
10. [Acute Management](#10-acute-management)
11. [Long-Term Treatment](#11-long-term-treatment)
12. [Drug-Induced Junctional Rhythm](#12-drug-induced-junctional-rhythm)
13. [Special Situations](#13-special-situations)
14. [Complications](#14-complications)
15. [Prognosis](#15-prognosis)
---
# 1. DEFINITION AND ANATOMY
## 1.1 Definition
**Junctional rhythm** is a cardiac rhythm arising from the **atrioventricular (AV) junction** (AV node and/or proximal His bundle) rather than the sinoatrial (SA) node. It occurs when the SA node rate falls below the intrinsic rate of the AV junction, or when SA node impulses are blocked from reaching the AV node.
- Junctional rhythms are classified by rate: escape (40-60 bpm), accelerated (60-100 bpm), and tachycardia (>100 bpm)
- Diagnosis is based on ECG: absent or abnormal P waves with narrow QRS complexes and regular rhythm
> *- Tintinalli's Emergency Medicine, p. 147*
---
## 1.2 Anatomy and Physiology of the AV Junction
```
┌─────────────────────────┐
│ RIGHT ATRIUM │
│ │
│ [SA NODE] ─────────────┼──> Left Atrium
│ (60-100 bpm) │
│ │ │
│ ▼ │
│ INTERNODAL TRACTS │
│ (Anterior, Middle, │
│ Posterior) │
│ │ │
└─────────┼────────────────┘
╔═════════╪════════════════╗
║ AV JUNCTION ║
║ ┌──────▼──────────┐ ║
║ │ AV NODE │ ║ ← COMPACT NODE
║ │ (40-60 bpm) │ ║ (Koch's Triangle)
║ └──────┬──────────┘ ║
║ │ ║
║ ┌──────▼──────────┐ ║
║ │ BUNDLE OF HIS │ ║
║ │ (40-60 bpm) │ ║
╚══════════════════════════╝
│
┌─────────┼─────────────────┐
│ LEFT BUNDLE RIGHT BUNDLE │
│ BRANCH BRANCH │
│ │ │ │
│ PURKINJE FIBERS │
│ (Ventricles: 20-40 bpm) │
└────────────────────────────┘
```
### Key Anatomical Points:
- The **AV node** sits in the floor of the right atrium, at the apex of **Koch's Triangle** (bounded by: tendon of Todaro, tricuspid annulus, and coronary sinus ostium)
- Blood supply: **Right coronary artery (RCA)** in ~90% of people (dominant right circulation); hence inferior MI commonly causes junctional rhythm
- The **compact AV node** measures ~1 x 3 x 5 mm
- Autonomic innervation: rich supply from both sympathetic and parasympathetic systems
- The **His bundle** emerges from the AV node, runs along the membranous septum, and divides at the crest of the muscular septum
---
## 1.3 Normal Pacemaker Hierarchy
| Pacemaker Site | Intrinsic Rate | Notes |
|----------------|---------------|-------|
| SA Node | 60-100 bpm | Dominant pacemaker; sympathetic/vagal modulation |
| AV Node / His Bundle (AV Junction) | 40-60 bpm | Secondary pacemaker; "escape" at this rate |
| Bundle Branches | 25-40 bpm | Rarely seen |
| Purkinje Fibers / Ventricular Myocardium | 20-40 bpm | Last resort; wide QRS |
> **Pearl:** The higher pacemaker suppresses lower ones by **overdrive suppression** - each depolarization from above resets the lower site's clock. When the higher pacemaker fails, the lower site "escapes."
---
## 1.4 Escape Rhythm vs. Accelerated Rhythm
| Feature | Escape Rhythm | Accelerated Rhythm |
|---------|--------------|-------------------|
| Mechanism | SA node failure / block allowing AV junction to emerge | Enhanced automaticity of AV junction overriding SA node |
| Rate | 40-60 bpm | 60-100 bpm |
| Context | Protective response (avoids asystole) | Pathological usurpation of pacemaker |
| Treatment | Treat underlying cause; pacing if symptomatic | Treat underlying cause (e.g., digoxin toxicity) |
| Danger | If suppressed → asystole | Usually benign; investigate cause |
---
# 2. ELECTROPHYSIOLOGY
## 2.1 Automaticity of the AV Junction
- **Phase 4 spontaneous depolarization** (pacemaker potential) occurs in AV nodal and His bundle cells
- This is driven by the "funny current" (I_f) through HCN channels, plus slow inward Ca²⁺ and reduced K⁺ outward currents
- Normally suppressed by faster SA node impulses (overdrive suppression)
- AV junction automaticity is **slower** (40-60 bpm) than SA node (60-100 bpm), hence acts as backup
---
## 2.2 Escape Mechanism
```
Normal: SA node fires at 75 bpm → depolarizes AV junction before it spontaneously fires
→ AV junction clock continuously reset → suppressed
SA node failure or block:
SA node rate drops below 40-60 bpm → AV junction fires spontaneously
OR (escape beat → escape rhythm)
SA impulse blocked at AV node → "Rescue" of cardiac output
```
- The escape interval represents the time from last sinus beat to first junctional beat
- Multiple junctional escape beats = junctional escape rhythm
---
## 2.3 Enhanced Automaticity (Accelerated Junctional Rhythm / Junctional Tachycardia)
- Abnormal increase in Phase 4 slope → AV junction fires faster than SA node
- Causes: **Digoxin toxicity** (most classic), catecholamine excess, ischemia, fever, post-cardiac surgery
- The enhanced junctional pacemaker "usurps" the SA node
- Results in: Accelerated junctional rhythm (60-100 bpm) or Junctional tachycardia (>100 bpm)
---
## 2.4 Re-entry Mechanism
- **AVNRT (AV Nodal Reentry Tachycardia)** uses dual AV nodal pathways:
- Fast pathway (anterior, short RP) and Slow pathway (posterior, long RP)
- Most common SVT (~60% of all SVT)
- This is distinct from "true" junctional automatic tachycardia
- Re-entrant junctional rhythms are typically paroxysmal and abrupt in onset/termination
---
## 2.5 Influence of Autonomic Tone
| Autonomic Effect | SA Node | AV Junction | Net Result |
|-----------------|---------|-------------|------------|
| **Increased vagal tone** (sleep, athletes, vasovagal) | ↓↓ firing | ↓ firing but less suppressed | Junctional escape emerges |
| **Sympathetic stimulation** | ↑↑ firing | ↑ firing | SA node dominates; junctional suppressed |
| **Beta-blocker** | ↓ SA rate | Minimal effect on junction | Junctional escape may emerge |
| **Digoxin toxicity** | ↓ SA rate + SA block | ↑↑↑ enhanced automaticity | Accelerated junctional rhythm |
| **Atropine** | ↑ SA rate | Relative suppression of junctional | Restores sinus rhythm |
---
# 3. CLASSIFICATION
## 3.1 Overview Table
| Type | Rate | Mechanism | Clinical Significance |
|------|------|-----------|----------------------|
| Junctional Bradycardia | < 40 bpm | Severe SA suppression | Hemodynamically compromising; urgent pacing |
| **Junctional Escape Rhythm** | **40-60 bpm** | SA node failure / block | Protective; treat underlying cause |
| **Accelerated Junctional Rhythm (AJR)** | **60-100 bpm** | Enhanced AV junction automaticity | Often digoxin toxicity; investigate |
| **Junctional Tachycardia** | **> 100 bpm** | Enhanced automaticity / re-entry | May be hemodynamically significant |
| Non-paroxysmal Junctional Tachycardia | 70-130 bpm | Enhanced automaticity | Classic in digoxin toxicity; gradual onset |
| Congenital JET | 150-300 bpm | Congenital automaticity defect | Rare; life-threatening in neonates |
| Postoperative JET (POJET) | 170-260 bpm | Surgical trauma to His bundle | Most common early arrhythmia after congenital heart surgery |
---
## 3.2 Junctional Escape Rhythm (40-60 bpm)
**ECG Example 1 - Junctional Escape Rhythm with Hidden P Waves:**

**ECG Example 2 - Three P wave patterns in junctional rhythm:**
**ECG Example 3 - Junctional escape following a sinus pause (labeled):**

**ECG Features:**
- Rate: 40-60 bpm (regular)
- P waves: absent, hidden within QRS, or inverted/retrograde (in inferior leads II, III, aVF)
- QRS: narrow (< 120 ms) unless aberrant conduction
- PR interval: < 120 ms (if P wave before QRS) or negative RP relationship
**Clinical Significance:**
- Protective rhythm preventing asystole
- Seen with: sinus bradycardia, SA block, vasovagal episodes, sleep, trained athletes
- Treatment only if symptomatic (rate < 40 or hemodynamic compromise)
---
## 3.3 Accelerated Junctional Rhythm (60-100 bpm)
**ECG Example 4 - Accelerated Junctional Rhythm (12-lead):**
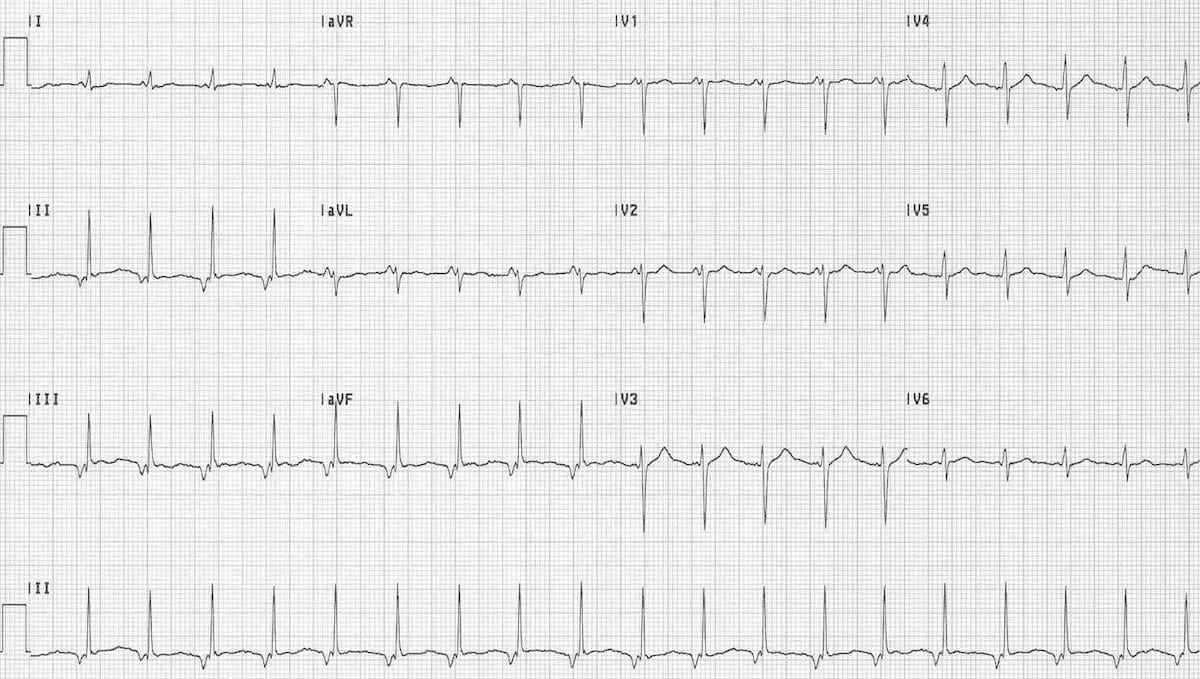
**ECG Example 5 - AJR rhythm strip, inverted P before QRS:**

**ECG Example 6 - Junctional rhythm with labeled inverted P wave:**

**ECG Features:**
- Rate: 60-100 bpm (regular)
- P waves: inverted in II, III, aVF; may be immediately before, within, or after QRS
- QRS: narrow
- AV dissociation may be present
**Clinical Significance:**
- Most commonly: **digoxin toxicity** (classic presentation)
- Also: inferior MI, myocarditis, cardiac surgery, electrolyte disturbance
- Usually hemodynamically well-tolerated
- Must investigate and treat underlying cause
---
## 3.4 Junctional Tachycardia (> 100 bpm)
**ECG Features:**
- Rate: > 100 bpm (typically 100-180 bpm)
- P waves: inverted/retrograde or dissociated
- QRS: narrow (unless aberrancy)
- Onset: may be gradual (automatic) or abrupt (re-entrant)
- Irregular rate variability: suggests automatic mechanism (vs. fixed rate in re-entry)
**ECG from Harrison's (Narrow-complex tachycardia diagnostic algorithm):**
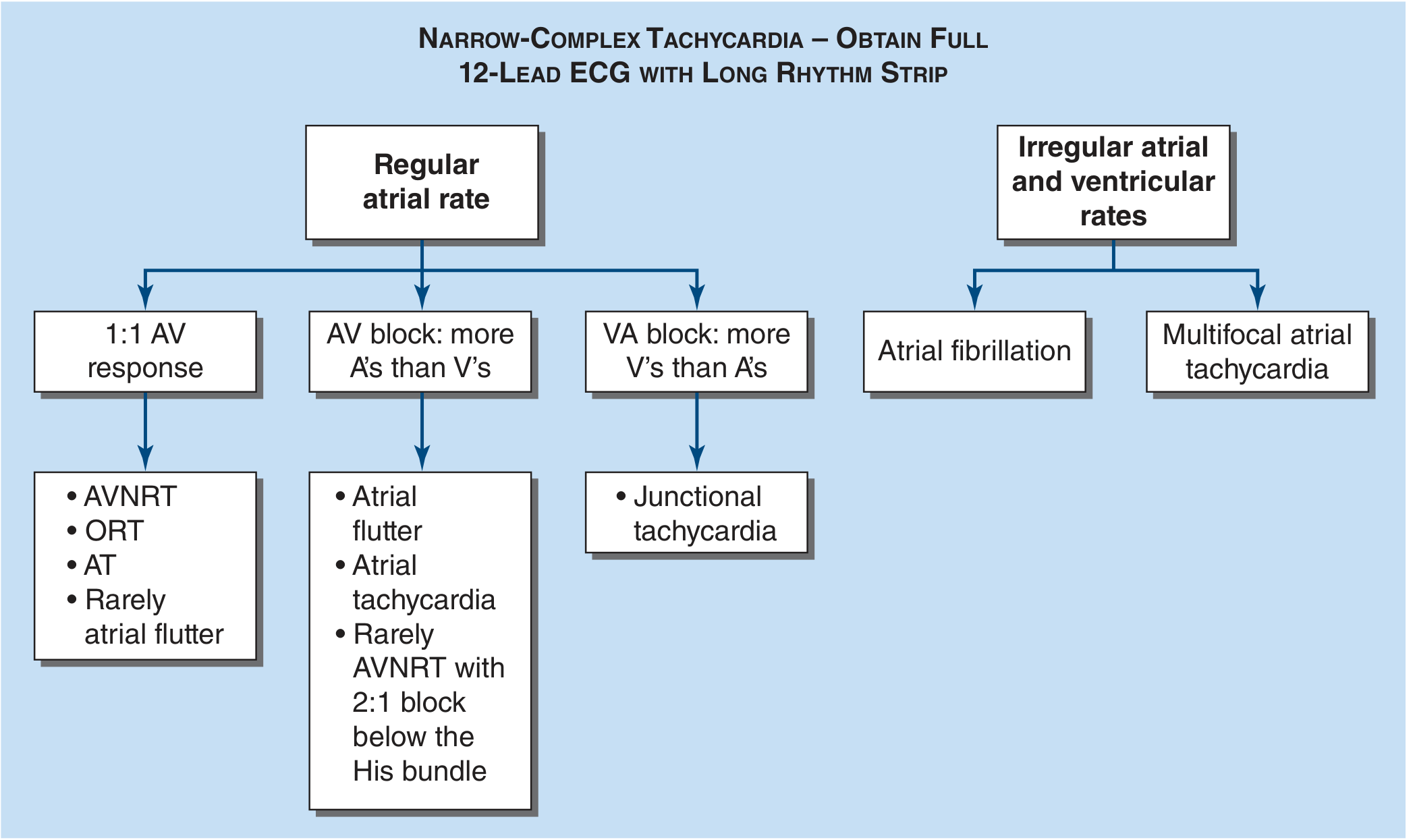
> Note: In junctional tachycardia, more V's than A's (VA block pattern) distinguishes it from AVNRT/ORT. - *Harrison's 22E, p. 1976*
---
## 3.5 Non-Paroxysmal Junctional Tachycardia (NPJT)
- Rate: 70-130 bpm
- **Gradual** onset and termination (vs. abrupt in re-entry)
- Classic hallmark of **digoxin toxicity** and inferior MI
- Also called "accelerated junctional tachycardia" when between 100-130 bpm
- May show AV dissociation with independent atrial rate
---
## 3.6 Congenital Junctional Ectopic Tachycardia (JET)
- Rare, autosomal dominant mutations (HCN4 channels)
- Presents in infancy/early childhood
- Rate: 150-300 bpm
- Often incessant; leads to **tachycardia-induced cardiomyopathy**
- ECG: narrow QRS, retrograde P waves, AV dissociation common
- Management: amiodarone, propafenone, catheter ablation in resistant cases
---
## 3.7 Postoperative JET (POJET)
**ECG Example - Postoperative JET after congenital heart surgery:**

- **Most common arrhythmia** in the first 24-72 hours after congenital heart surgery in children
- Incidence: 2-8% overall; up to 14% after tetralogy of Fallot repair or VSD closure
- Mechanism: thermal or mechanical injury to the His bundle or AV nodal region
- Rate: 170-260 bpm; AV dissociation present (V rate > A rate)
- Hemodynamically destabilizing: loss of AV synchrony + fast rate
- Management: surface cooling (reduce fever/temperature), magnesium, amiodarone, pacing above the junctional rate
---
# 4. ETIOLOGY
## 4.1 Comprehensive Cause Table
| Category | Specific Cause | Mechanism | Notes |
|----------|---------------|-----------|-------|
| **PHYSIOLOGICAL** | Athletes, sleep, vagal tone | Enhanced vagal tone suppresses SA node | Benign; escape rhythm |
| **DRUGS** | Digoxin toxicity | Enhanced AV junction automaticity + SA suppression | NPJT; most classic cause |
| | Beta-blockers | SA node suppression | Junctional escape |
| | Calcium channel blockers (diltiazem, verapamil) | SA/AV node depression | Escape rhythm |
| | Amiodarone | SA/AV node suppression | Escape rhythm |
| | Ivabradine | I_f channel blockade (SA > AV) | Junctional escape |
| | Adenosine | Transient AV block | Brief junctional escape |
| **CARDIAC** | Inferior wall MI | RCA ischemia → SA and AV node dysfunction | NPJT or escape; associated with 3rd degree block |
| | Sick sinus syndrome (SSS) | Degeneration of SA node | Junctional escape; bradycardia-tachycardia syndrome |
| | Sinus arrest | Complete failure of SA node to fire | Junctional escape rescues rhythm |
| | SA exit block | SA fires but impulse blocked from leaving | Junctional escape |
| | Complete AV block | P waves dissociated from QRS | Junctional escape rhythm (narrow QRS) |
| | 2nd degree AV block | Intermittent SA-to-AV block | Intermittent junctional escape |
| | Myocarditis | Inflammatory damage to conduction system | Any type of junctional rhythm |
| | Cardiac surgery | Mechanical/thermal injury to His-AV junction | POJET (especially congenital surgery) |
| | Congenital heart disease | Structural abnormalities near AV node | Congenital JET |
| **METABOLIC / ELECTROLYTES** | Hyperkalemia | Depressed SA automaticity | Junctional escape |
| | Hypokalemia | Enhanced automaticity | Accelerated junctional |
| | Hypomagnesemia | Enhanced automaticity | Accelerated junctional |
| | Hypocalcemia | Conduction disturbance | Various bradyarrhythmias |
| | Hypothyroidism | Slowed SA node | Junctional escape |
| | Hypothermia | Global conduction slowing | Osborn waves + junctional rhythm |
| **RESPIRATORY / SYSTEMIC** | Hypoxia | SA node ischemia | Junctional escape or tachycardia |
| | Sleep apnea | Hypoxia + vagal surges | Nocturnal junctional rhythm |
| | Sepsis/ICU | Autonomic dysregulation | Variable |
| **IDIOPATHIC** | No identifiable cause | Unknown | Diagnosis of exclusion |
---
## 4.2 Memory Aid - Causes of Junctional Rhythm
```
Mnemonic: "DIME-CHASM"
D - Digoxin toxicity (classic)
I - Inferior MI (RCA territory)
M - Myocarditis
E - Electrolytes (K+, Mg2+, Ca2+)
C - Cardiac surgery (POJET)
H - Hypoxia / Hypothermia
A - Athletes / Autonomic (vagal) tone
S - Sick sinus syndrome / Sinus arrest
M - Medications (beta-blockers, CCB, amiodarone)
```
---
# 5. ECG DIAGNOSIS
## 5.1 Stepwise ECG Interpretation
```
STEP-BY-STEP APPROACH TO JUNCTIONAL RHYTHM ON ECG
═══════════════════════════════════════════════════
Step 1: CALCULATE THE RATE
Count R-R intervals
Rate = 300 ÷ large squares between R-R
OR Rate = 1500 ÷ small squares between R-R
< 40: Junctional bradycardia (severe)
40-60: Junctional escape rhythm
60-100: Accelerated junctional rhythm
> 100: Junctional tachycardia
Step 2: ASSESS RHYTHM REGULARITY
Regular R-R intervals (usually)
Slight irregularity → suggests automatic mechanism
Abrupt onset/termination → suggests re-entrant mechanism
Step 3: ASSESS QRS DURATION
Narrow QRS (< 120 ms) = supraventricular origin
Wide QRS (≥ 120 ms) = aberrant conduction OR ventricular origin
KEY: Junctional rhythm should have NARROW QRS
Step 4: LOOK FOR P WAVES
Search CAREFULLY in all leads (especially lead II, V1, aVR)
Four P wave scenarios in junctional rhythm:
A. NO P waves visible
- P wave buried within QRS
- Most common pattern
B. INVERTED P WAVE BEFORE QRS (short PR < 120 ms)
- Retrograde P wave (inverted in II, III, aVF; upright in aVR)
- Retrograde conduction faster than antegrade
- RP interval: very short (< 80 ms)
C. P WAVE WITHIN QRS (simultaneous)
- Atria and ventricles depolarize simultaneously
- P wave buried/obscured
D. INVERTED P WAVE AFTER QRS (short RP)
- Retrograde P wave follows QRS (in ST segment)
- Antegrade conduction faster than retrograde
- RP interval: 80-200 ms
Step 5: ASSESS AV RELATIONSHIP
Retrograde P (inverted in II/III/aVF) = typical junctional
Independent P waves (dissociated) = AV dissociation
P rate < QRS rate in AV dissociation
Step 6: LOOK FOR AV DISSOCIATION FEATURES
Capture beats: sinus P wave conducts, produces narrow QRS
Fusion beats: simultaneous junctional + sinus activation
Variable PR intervals in dissociation
Step 7: CONFIRM WITH 12-LEAD ECG
Lead II: Best for P wave morphology
Lead V1: P wave visible in biphasic pattern
aVR: Upright retrograde P wave (normally inverted)
aVF: Inverted retrograde P wave
```
---
## 5.2 ECG Gallery
### ECG 1 - Junctional Escape Rhythm (Hidden P Waves)

```
Analysis:
- Rate: 46 bpm (top strip)
- Rhythm: Regular
- P waves: Hidden within QRS complex (no visible P waves)
- QRS: Narrow (< 120 ms)
- Note: Loss of atrial kick → cannon A waves possible
```
### ECG 2 - Three Patterns of Retrograde P Waves

```
Pattern A (Top): Hidden P - atrial and ventricular depolarization simultaneous
Pattern B (Middle): Inverted P before QRS - retrograde faster than antegrade
Pattern C (Bottom): P wave after QRS - antegrade faster than retrograde
```
### ECG 3 - Junctional Escape Beat (After Sinus Pause - Labeled)

```
Analysis:
- Sinus rhythm initially → sinus pause (no P wave)
- After pause: junctional escape beat fires
- Inverted P wave visible AFTER QRS (retrograde P)
- The beat "rescues" from asystole
```
### ECG 4 - Accelerated Junctional Rhythm (12-Lead)

```
Analysis:
- Rate: ~78 bpm (accelerated junctional)
- QRS: Narrow in all leads
- P waves: Not clearly discernible preceding QRS
- Retrograde P may be buried in QRS or T wave
- Look for inverted P in II, III, aVF
```
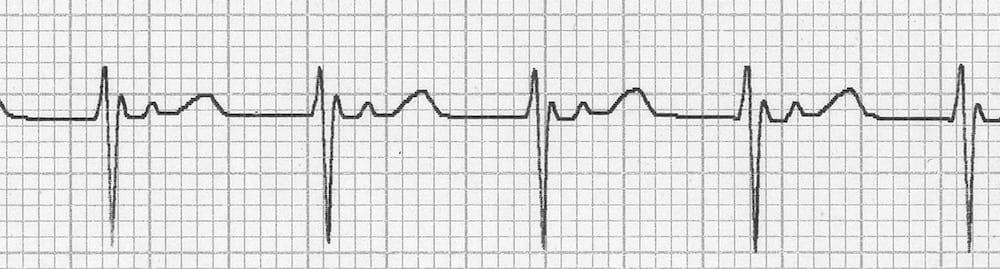
### ECG 5 - AJR Rhythm Strip (Inverted P before QRS)

```
Analysis (LITFL):
- Rate: ~85 bpm
- Rhythm: Regular
- P wave: Inverted (retrograde) immediately before QRS
- PR interval: Very short (< 120 ms)
- QRS: Narrow
- Diagnosis: Accelerated Junctional Rhythm with retrograde P waves before QRS
```
### ECG 6 - Labeled Inverted P Wave (Before QRS)

```
Teaching Points:
- Retrograde P (red) = inverted in lead II
- P wave BEFORE QRS: retrograde conduction to atria completes before ventricular
activation = short PR interval (often < 120 ms)
- Distinguish from: low atrial rhythm (where P is upright but non-sinus)
```
---
## 5.3 P Wave Patterns - Detailed Explanation
```
RETROGRADE ATRIAL ACTIVATION DIAGRAM
════════════════════════════════════
Normal Sinus: SA → Atria → AV node → His → Ventricles
P wave UPRIGHT in II, III, aVF
PR interval: 120-200 ms
Junctional: AV node/His → [Ventricles (antegrade) + Atria (retrograde)]
Case A: Equal speeds
Ventricles ────────────────────> QRS
Atria ──────────────────────> P
(hidden within QRS)
Case B: Retrograde faster
Atria depolarize BEFORE ventricles
P (inverted) ─────> QRS
Short PR < 120 ms
Case C: Antegrade faster
QRS ─────────────────> P (inverted, after QRS)
RP interval < 200 ms
P visible in ST segment
Case D: Total retrograde block
No retrograde atrial activation at all
AV dissociation: SA fires at own rate
P waves "march through" independently
```
---
## 5.4 AV Dissociation
- **Definition:** Independent firing of atria (by SA node) and ventricles (by junctional pacemaker)
- P waves and QRS are unrelated; P waves march through at their own rate
- May be **complete** or **incomplete**
- Look for: P waves at different positions relative to QRS in consecutive beats
- **Capture beats:** When a sinus P wave reaches AV node at the right moment, it conducts and produces a QRS (narrow, normal PR) - proves AV dissociation
- **Fusion beats:** Simultaneous activation from both sinus and junctional pacemakers - QRS morphology is intermediate
---
## 5.5 Summary ECG Features Table
| Feature | Junctional Escape (40-60) | Accelerated Junctional (60-100) | Junctional Tachy (>100) |
|---------|--------------------------|--------------------------------|------------------------|
| Rate | 40-60 bpm | 60-100 bpm | >100 bpm |
| Rhythm | Regular | Regular | Regular (slight variability if automatic) |
| P waves | Absent/retrograde/hidden | Absent/retrograde | Absent/retrograde/dissociated |
| PR interval | Short (<120ms) or no P | Short (<120ms) or no P | Short or N/A |
| QRS | Narrow (<120ms) | Narrow (<120ms) | Narrow (<120ms) |
| RP interval | Very short | Very short | Short |
| AV dissociation | Possible | Possible | Common |
> Sources: Tintinalli's Emergency Medicine Table 18-6; LITFL ECG Library
---
# 6. ECG DIFFERENTIAL DIAGNOSIS
## 6.1 Bradycardia Differential
| Feature | Junctional Escape | Sinus Bradycardia | Sinus Arrest | SA Exit Block | Ventricular Escape | Complete Heart Block |
|---------|------------------|-------------------|-------------|--------------|-------------------|---------------------|
| Rate | 40-60 | < 60 | Variable | Variable | 20-40 | Varies |
| P waves | Absent/retrograde/inverted | Upright, precede each QRS | Absent during arrest | May be absent (grouped) | Absent | Present but dissociated |
| PR interval | Short/absent | Normal (120-200ms) | N/A | Normal when present | N/A | No relationship |
| QRS | **Narrow** | Narrow | Narrow (if junctional escape) | Narrow | **Wide** | Narrow (junctional escape) or wide (ventricular) |
| Rhythm | Regular | Regular | Irregular (pauses) | Irregular (pauses) | Regular | Regular (but P and QRS independent) |
| Key clue | Inverted P / no P + narrow QRS | Upright P before every QRS | Long pause without P wave | Pauses are multiples of PP interval | Wide QRS, very slow | P rate > QRS rate; no conduction |
---
## 6.2 Tachycardia Differential
| Feature | Junctional Tachy (automatic) | AVNRT | AVRT (ORT) | Atrial Tachycardia | Sinus Tachycardia |
|---------|------------------------------|-------|-----------|-------------------|------------------|
| Rate | 100-180 | 150-250 | 150-250 | 150-250 | 100-150 |
| Onset/termination | Gradual (warm up) | Abrupt | Abrupt | Gradual or abrupt | Gradual |
| P wave | Retrograde/dissociated | Retrograde, in QRS (typical) | Retrograde, after QRS | Ectopic P before QRS | Upright, before QRS |
| RP relationship | Short RP or long RP (variable) | Very short RP | Short RP (>70ms, RP<PR) | Long RP | Long RP |
| Response to adenosine | May slow/terminate | Terminates | Terminates | May unmask/slow | Transient slowing |
| AV dissociation | Common | Rare | Absent | May occur | No |
| Rate variability | Yes (automatic) | No | No | May vary | Varies with physiology |
| Delta wave on resting ECG | No | No | Yes (if WPW) | No | No |
---
## 6.3 Comparison: Junctional vs. Idioventricular Escape
| Feature | Junctional Escape Rhythm | Idioventricular Rhythm (IVR) |
|---------|--------------------------|------------------------------|
| Origin | AV node / His bundle | Ventricle (Purkinje) |
| Rate | 40-60 bpm | 20-40 bpm |
| QRS | **Narrow** (< 120 ms) | **Wide** (> 120 ms) |
| QRS morphology | Normal | Bizarre, LBBB/RBBB pattern |
| P waves | Absent/retrograde | Usually absent or dissociated |
| Clinical context | SA node failure | Complete heart block, late rescue |
| Treatment urgency | Moderate | HIGH - pacing usually needed |
> Source: Tintinalli's Emergency Medicine, Table 18-7
---
## 6.4 Accelerated Idioventricular Rhythm (AIVR) vs. Accelerated Junctional Rhythm (AJR)
| Feature | AIVR | AJR |
|---------|------|-----|
| Rate | 50-110 bpm | 60-100 bpm |
| QRS | **Wide** (> 120 ms) | **Narrow** (< 120 ms) |
| Context | Post-MI reperfusion, digoxin | Digoxin, inferior MI, post-surgery |
| AV dissociation | Common | Common |
| Capture beats | Present | Present |
| Hemodynamics | Usually tolerated | Usually tolerated |
---
# 7. CLINICAL FEATURES
## 7.1 Symptoms
| Symptom | Mechanism | Frequency |
|---------|-----------|-----------|
| **Asymptomatic** | Adequate CO at escape rates | Most junctional escape rhythms |
| Fatigue / Weakness | Reduced cardiac output | Common |
| Palpitations | Awareness of arrhythmia | Accelerated/tachycardia forms |
| Lightheadedness / Presyncope | Reduced cerebral perfusion | Slower rates |
| **Syncope** | Severe bradycardia or initial sinus arrest pause | Less common |
| Dyspnea | Reduced CO → pulmonary congestion | Advanced cases |
| Neck pulsations | Cannon A waves | AV dissociation |
| Chest discomfort | Underlying ischemia or reduced CO | When associated with MI |
---
## 7.2 Signs
### Cannon A Waves (Important Clinical Sign)
```
MECHANISM OF CANNON A WAVES IN AV DISSOCIATION:
Normal:
Atria contract (A wave) ──────────> [tricuspid open] ──> blood flows to RV
AV Dissociation:
Atria contract AGAINST CLOSED tricuspid valve
(closed because RV has already started contracting)
↓
Blood reflected back to jugular veins
↓
VISIBLE CANNON A WAVE in JVP
(occurs intermittently when P wave falls just before/during QRS)
```
- **Regular cannon A waves:** every beat is dissociated (complete AV dissociation in junctional tachycardia)
- **Intermittent cannon A waves:** incomplete AV dissociation; varies beat to beat
- Differentiate from: tricuspid regurgitation (causes systolic V waves, not A waves)
---
## 7.3 Hemodynamic Consequences
| Hemodynamic Effect | Mechanism | Consequence |
|-------------------|-----------|-------------|
| Loss of atrial contribution | No synchronized atrial contraction | ↓ CO by 15-25% |
| Reduced diastolic filling | Fast rate (tachycardia) → short diastole | ↓ SV |
| Hypotension | Reduced CO | Dizziness, presyncope, shock |
| Heart failure | Prolonged junctional tachycardia | Tachycardia-induced cardiomyopathy |
| Cardiogenic shock | Severe bradycardia or tachycardia in compromised heart | Emergency pacing needed |
| AV dyssynchrony | Loss of atrial kick | Especially significant in poor LV function |
---
## 7.4 Clinical Pearls
> **Pearl 1:** In a patient with AV dissociation, ask them to lie flat and watch the jugular vein - intermittent large pulsations (cannon A waves) clinch the diagnosis.
> **Pearl 2:** A junctional rhythm in the setting of suspected digoxin toxicity should stop all digoxin immediately and measure serum digoxin level.
> **Pearl 3:** After inferior STEMI, a junctional escape rhythm is a "benign" protective rhythm - treat with PCI/thrombolysis and monitor; do not immediately pace unless hemodynamically compromised.
> **Pearl 4:** POJET after congenital heart surgery: ventricular rate > atrial rate is the hallmark (unlike complete heart block where atrial rate > ventricular rate).
---
# 8. DIAGNOSTIC EVALUATION
## 8.1 History
Key questions to ask:
- Drug history: **digoxin, beta-blockers, CCB, amiodarone, ivabradine** (ask specifically)
- Recent cardiac surgery or catheterization
- Symptoms of inferior MI: inferior chest pain, diaphoresis, nausea
- Exercise tolerance (athletes may have benign junctional escape)
- Sleep history (sleep apnea symptoms)
- Family history of conduction disease or sudden death
---
## 8.2 Physical Examination
| Finding | Significance |
|---------|--------------|
| Heart rate, rhythm | Bradycardia or tachycardia |
| Blood pressure | Hemodynamic compromise? |
| JVP: cannon A waves | AV dissociation |
| JVP: elevated | Right heart failure |
| Lungs: crepitations | Left heart failure |
| Signs of inferior MI | RCA territory ischemia |
| Yellow xanthopsia | Digoxin toxicity |
| Cool extremities | Reduced CO |
---
## 8.3 Laboratory Investigations
| Test | Indication | What to Look For |
|------|-----------|-----------------|
| **CBC** | Routine | Anemia (contributing hypoxia), infection (myocarditis) |
| **Serum electrolytes (Na, K, Cl, HCO3)** | All patients | Hyper/hypokalemia; hyponatremia |
| **Serum calcium** | All patients | Hypocalcemia → conduction disturbance |
| **Serum magnesium** | All patients | Hypomagnesemia → enhanced automaticity |
| **Thyroid function (TSH, T3, T4)** | Bradycardia workup | Hypothyroidism → SA suppression |
| **Cardiac troponin (hs-cTnI/T)** | Suspected MI or myocarditis | Elevation confirms injury |
| **Serum digoxin level** | Digoxin use or toxicity suspected | Therapeutic: 0.5-0.9 ng/mL; toxic: > 2 ng/mL |
| **ABG** | Respiratory symptoms or ICU | Hypoxia, acidosis affecting automaticity |
| **Drug screen** | Unknown cause | Other toxidromes |
| **BNP/NT-proBNP** | Heart failure symptoms | Elevated in decompensation |
| **Lactate** | Hemodynamic compromise | Tissue hypoperfusion |
---
## 8.4 Cardiac Investigations
| Investigation | Indication | Findings |
|--------------|-----------|---------|
| **12-lead ECG** | All patients (first test) | Rate, rhythm, P wave morphology, QRS, intervals |
| **Serial ECG** | Dynamic changes, MI monitoring | ST changes, evolving block |
| **Rhythm monitor / Telemetry** | Inpatients, post-surgery | Continuous monitoring; capture intermittent rhythms |
| **24-hour Holter** | Outpatients, symptoms | Correlation of symptoms with rhythm |
| **Event recorder / Loop recorder** | Infrequent palpitations/syncope | Long-term symptom-rhythm correlation |
| **Echocardiography** | All patients with junctional rhythm | Structural disease, LV function, pericardial effusion |
| **Exercise stress test** | Chronotropic response evaluation | Appropriate rate response; exclude ischemia |
| **Electrophysiology study (EPS)** | Recurrent tachycardia, pre-ablation | Map reentrant circuit; ablation target |
| **Cardiac MRI** | Myocarditis, cardiomyopathy suspected | Fibrosis, inflammation |
| **Coronary angiography** | Suspected ischemic cause | Coronary anatomy; PCI if indicated |
| **Pharmacological provocation** | Carotid sinus hypersensitivity | Atropine test (expected: ↑ rate by >25%) |
---
# 9. APPROACH ALGORITHM
```
CLINICAL APPROACH TO JUNCTIONAL RHYTHM
════════════════════════════════════════
PATIENT WITH SUSPECTED JUNCTIONAL RHYTHM
│
▼
┌─────────────────┐
│ 12-LEAD ECG │
└────────┬────────┘
│
┌───────────────────┼──────────────────┐
▼ ▼ ▼
Narrow QRS + Wide QRS + Narrow QRS +
absent/retrograde P slow rate tachycardia >100
│ │ │
JUNCTIONAL RHYTHM Consider: JUNCTIONAL TACHY
│ Ventricular escape │
│ Complete heart block │
│ │
└────────────────────┬───────────────────┘
│
┌──────────▼──────────┐
│ HEMODYNAMICALLY │
│ STABLE OR UNSTABLE?│
└──────┬──────────────┘
│
┌────────────────┤
▼ ▼
STABLE UNSTABLE
(BP OK, (Hypotension,
no symptoms) syncope, CHF,
│ AMS, angina)
│ │
▼ ▼
IDENTIFY CAUSE EMERGENCY:
│ • O2, IV access
┌──────┴──────┐ • Atropine 0.5 mg IV
▼ ▼ • Dopamine/Epinephrine
ESCAPE ACCEL. • Transcutaneous pacing
RHYTHM JUNCTIONAL • Transvenous pacing
│ │ │
▼ ▼ ▼
Investigate: Investigate: STABILIZE FIRST
• Drugs • Digoxin THEN investigate
• SSS • Inferior MI
• AV block • Post-surgery
• Vagal tone • Electrolytes
│
▼
REVERSIBLE CAUSE FOUND?
│ │
YES NO
│ │
TREAT CAUSE PERMANENT
(stop drug, PACEMAKER
treat MI, consideration
correct electrolyte)
│
▼
REASSESS ECG + SYMPTOMS
│
┌────┴─────┐
▼ ▼
Resolved Persists
│
▼
Consider pacemaker
or EP referral
```
---
# 10. ACUTE MANAGEMENT
## 10.1 Initial Stabilization (All Patients)
```
ABC APPROACH:
━━━━━━━━━━━━
A - Airway: Ensure patent; intubate if compromised
B - Breathing: O2 via nasal cannula or mask; target SpO2 > 94%
C - Circulation:
• Large bore IV access (18G or larger)
• Continuous cardiac monitoring (telemetry)
• 12-lead ECG stat
• BP monitoring (continuous if unstable)
• Labs: electrolytes, digoxin level, troponin, ABG
```
---
## 10.2 Stable Patient
| Situation | Action |
|-----------|--------|
| Asymptomatic junctional escape rhythm | Monitor; no acute treatment needed |
| Digoxin-induced (any rate) | Stop digoxin; monitor levels; digoxin-immune Fab if toxic |
| Beta-blocker/CCB induced | Stop offending drug; supportive care |
| Inferior MI | IV access, monitoring; atropine if symptomatic bradycardia; proceed to reperfusion |
| Electrolyte cause | Correct electrolyte (IV potassium, magnesium) |
| Vagal (athlete, sleep) | Reassurance; no treatment |
| Post-cardiac surgery (slow JR) | Monitor; temporary pacing if rate < 40 or symptomatic |
| POJET | Cooling, magnesium, amiodarone; atrial overdrive pacing |
---
## 10.3 Unstable Patient - Emergency Algorithm (ACC/AHA/ACLS Based)
```
UNSTABLE JUNCTIONAL BRADYCARDIA PROTOCOL
══════════════════════════════════════════
Signs of instability:
✓ Hypotension (SBP < 90)
✓ Altered mental status
✓ Signs of heart failure
✓ Chest pain (ischemia)
✓ Syncope/near-syncope
FIRST LINE:
┌────────────────────────────────────────────────┐
│ ATROPINE 0.5 mg IV BOLUS │
│ • Repeat every 3-5 minutes │
│ • Maximum total dose: 3 mg (0.04 mg/kg) │
│ • Mechanism: Blocks muscarinic receptors → │
│ increases SA rate, enhances AV conduction │
│ • Note: Less effective for infranodal block │
│ • Note: NOT effective for digoxin-induced JR │
│ (may paradoxically worsen) │
└────────────────────────────────────────────────┘
│
▼ (if no response)
SECOND LINE (PHARMACOLOGICAL):
┌────────────────────────────────────────────────┐
│ Options (while preparing for pacing): │
│ │
│ DOPAMINE: 2-10 mcg/kg/min IV infusion │
│ • Beta-1 + dopaminergic effects at low doses │
│ • Alpha + beta at higher doses │
│ • Use if hypotension persists │
│ │
│ EPINEPHRINE: 2-10 mcg/min IV infusion │
│ • Alpha + beta agonist │
│ • Use in severe shock │
│ • Increases automaticity and heart rate │
│ │
│ ISOPROTERENOL: 2-10 mcg/min IV infusion │
│ • Pure beta-1 + beta-2 agonist │
│ • Increases heart rate effectively │
│ • Use in complete heart block while awaiting │
│ pacemaker; rarely used in isolation │
└────────────────────────────────────────────────┘
│
▼ (if pharmacological fails or severe instability)
THIRD LINE - PACING:
```
---
## 10.4 Pacing Options
| Type | Access | Speed | Indication | Notes |
|------|--------|-------|-----------|-------|
| **Transcutaneous pacing (TCP)** | Skin electrodes | Immediate (< 2 min) | Emergent; first-line while preparing TV pacing | Painful; unreliable; use as bridge |
| **Transvenous pacing (TVP)** | Femoral/subclavian/internal jugular vein | 15-30 min | Definitive temporary pacing | Reliable; needs fluoroscopy/ultrasound guidance |
| **Transesophageal pacing** | Esophagus | Rapid | Atrial pacing in POJET | Limited to atrial pacing |
| **Permanent pacemaker (PPM)** | Subcutaneous + transvenous | Weeks later | Persistent symptomatic bradycardia | Definitive treatment |
### Pacing Rate and Thresholds:
- Temporary pacing threshold: typically 5-10 mA (set at 2x threshold)
- Rate: usually set at 60-80 bpm
- In POJET: atrial overdrive pacing at rate > junctional rate to restore AV synchrony
---
## 10.5 Digoxin Toxicity Specific Management
```
DIGOXIN TOXICITY WITH JUNCTIONAL RHYTHM:
═════════════════════════════════════════
1. STOP digoxin immediately
2. Continuous cardiac monitoring
3. Correct hypokalemia (K+ acts synergistically with digoxin toxicity)
4. Correct hypomagnesemia
5. DO NOT use calcium (may worsen)
6. Atropine: use cautiously (may increase junctional rate unpredictably)
7. Lidocaine or phenytoin: for ventricular arrhythmias from digoxin
8. DIGOXIN-IMMUNE FAB (Digibind/DigiFab):
- Indication: life-threatening arrhythmia, K+ > 5.0, ingestion > 10 mg
- Dose: based on serum level and body weight
- Reversal within 20-30 minutes
9. Cardioversion: AVOID (may precipitate refractory VF)
```
---
# 11. LONG-TERM TREATMENT
## 11.1 Treat Underlying Cause
| Cause | Long-Term Treatment |
|-------|-------------------|
| Digoxin toxicity | Discontinue digoxin; use alternative drugs |
| Beta-blocker excess | Dose reduction or discontinuation |
| Sick sinus syndrome | Permanent pacemaker |
| Inferior MI with persistent block | Permanent pacemaker if block persists > 2 weeks |
| Myocarditis | Treat underlying infection/inflammation; usually resolves |
| Electrolyte disturbance | Correct and maintain normal levels |
| Congenital JET | Antiarrhythmics (amiodarone, flecainide); catheter ablation |
| POJET | Usually self-limiting by day 3-5; manage acutely |
---
## 11.2 Permanent Pacemaker Indications in Junctional Rhythm
**Class I Indications (ACC/AHA Guidelines):**
- Symptomatic bradycardia due to **sinus node dysfunction** (junctional escape with symptoms)
- **Complete AV block** with junctional escape rhythm and symptoms
- **Third-degree AV block** with rate < 40 bpm or asystole > 3 seconds
- Bradycardia due to required drug therapy with no alternatives
- Post-inferior MI: persistent complete AV block (> 2 weeks)
**Class IIa Indications:**
- Asymptomatic bradycardia with HR < 40 during waking hours
- Sinus node dysfunction with HR < 40 and symptoms attributable to bradycardia
---
## 11.3 Catheter Ablation
- Indicated for: **congenital JET** refractory to medical therapy; **AVNRT** (if re-entrant mechanism confirmed on EPS)
- Target: Slow pathway ablation for AVNRT (success rate > 95%)
- Risk: AV block (1-3% with slow pathway ablation)
- For automatic JET: ablation near His bundle carries risk of complete AV block → requires simultaneous pacemaker
---
## 11.4 Follow-Up
- Asymptomatic benign junctional rhythm: annual ECG review; Holter if symptoms develop
- Post-MI: monitor for 24-48 hours; permanent pacing if block persists
- Post-cardiac surgery: ICU monitoring; discharge when stable sinus rhythm restored
- Pacemaker patients: device clinic at 1, 3, 6, and 12 months, then annually
---
# 12. DRUG-INDUCED JUNCTIONAL RHYTHM
## 12.1 Summary Table
| Drug | Mechanism | Type of Junctional Rhythm | Management |
|------|-----------|--------------------------|------------|
| **Digoxin** | Vagotonic (inhibits Na/K-ATPase) + enhanced AV junction automaticity | NPJT (70-130 bpm); AV dissociation | Stop digoxin; correct K+/Mg2+; Fab fragments if severe |
| **Beta-blockers** | Block beta-1 receptors → ↓ SA node rate and conduction | Junctional escape (40-60 bpm) | Reduce/stop drug; glucagon for reversal; atropine; temporary pacing |
| **Calcium channel blockers** (diltiazem, verapamil) | Block L-type Ca²⁺ channels → ↓ SA and AV node conduction | Junctional escape | Stop drug; calcium gluconate/chloride IV; atropine; temporary pacing |
| **Amiodarone** | Complex: blocks Na, K, Ca channels + beta-blocking + thyroid effects | Junctional bradycardia / escape | Reduce dose; temporary pacing if symptomatic |
| **Ivabradine** | Blocks HCN4 (I_f) channels in SA node > AV junction | Junctional escape (SA slows more) | Reduce dose; stop if symptomatic |
| **Adenosine** | A1 receptor → transient AV block (IKAdo ↑) | Brief junctional escape (15-30 sec) | Transient; no treatment needed; reassure |
---
## 12.2 Key Pearls on Drug-Induced JR
> **Digoxin:** The only drug that characteristically causes *accelerated* junctional rhythm (enhanced automaticity). All others cause junctional *escape* (suppressed SA node).
> **Beta-blocker overdose:** Give glucagon 5-10 mg IV bolus (bypasses beta receptor), high-dose insulin-glucose therapy (HIET) in severe cases.
> **CCB overdose:** Give calcium chloride 1g IV (10mL of 10%) or calcium gluconate 3g IV. Add glucagon and HIET for severe cases.
> **Amiodarone:** Long half-life (~50 days) means effects persist long after stopping; may require temporary pacing for weeks.
---
# 13. SPECIAL SITUATIONS
## 13.1 Inferior Wall Myocardial Infarction
- **RCA** supplies SA node (55%) and AV node (90%) in dominant right circulation
- Inferior MI (ST elevation in II, III, aVF) → SA and/or AV node ischemia
- Junctional rhythm in inferior MI may represent:
1. Sinus arrest or severe bradycardia with junctional escape
2. High-degree AV block with junctional escape
3. NPJT (enhanced automaticity from ischemia)
- **Management priorities:**
1. Immediate reperfusion (PCI/thrombolysis)
2. Atropine for symptomatic bradycardia (0.5-1 mg IV)
3. Temporary pacing if atropine fails
4. Most cases resolve after reperfusion
5. Permanent pacemaker rarely needed (unlike anterior MI)
> *"The junctional escape rhythm in this case is most likely the result of an inferior myocardial infarction in the distribution of the right coronary artery."* - Frameworks for Internal Medicine
---
## 13.2 Digoxin Toxicity
- Classic presentation: nausea/vomiting + visual disturbances (yellow-green) + bradycardia + **NPJT**
- Digoxin level > 2 ng/mL is toxic (symptoms may occur at lower levels if K+ low)
- ECG: NPJT with AV dissociation; bidirectional VT (severe toxicity)
- Complete digoxin toxicity picture: "PAT with block" (multifocal atrial tachycardia with AV block) or NPJT
- Hyperkalemia (K+ > 5) = severe toxicity → immediate Fab fragments
---
## 13.3 Cardiac Surgery
- POJET: Most common arrhythmia after pediatric congenital heart surgery
- Also occurs after adult cardiac surgery (CABG, valve repair)
- Adult post-surgical JR: usually junctional escape from surgical trauma; transient
- Management: temporary epicardial pacing wires placed intraoperatively; rate support with dopamine
---
## 13.4 Congenital Heart Disease
- ASD repair, VSD repair, tetralogy of Fallot repair → proximity to AV node/His bundle
- Late conduction disease may develop years post-repair
- Long-term monitoring with periodic Holter/EPS recommended
---
## 13.5 Athletes
- **Highly trained athletes:** Enhanced vagal tone → marked sinus bradycardia → junctional escape
- Typically rate 40-55 bpm; asymptomatic; disappears with exercise
- No treatment needed; important **not to misdiagnose** as pathological
- Pre-participation screening: obtain 12-lead ECG; detraining test if uncertain
---
## 13.6 Pregnancy
- Physiological increase in heart rate during pregnancy; junctional rhythm uncommon
- Maternal junctional tachycardia: treat with beta-blockers (metoprolol - relatively safe) or flecainide
- Avoid amiodarone (teratogenic, neonatal hypothyroidism)
- Temporary pacing if hemodynamic compromise before delivery
---
## 13.7 Pediatric Patients
| Age Group | Common Junctional Rhythm | Notes |
|-----------|--------------------------|-------|
| Neonates | Congenital JET | Presents at < 6 months; incessant; tachycardia-cardiomyopathy |
| Infants post-CHD surgery | POJET | 170-260 bpm; within 72h of surgery |
| Older children | Junctional escape, AVNRT | Vagal tone, structural disease |
| Adolescents | AVNRT, AJR | Often benign; may need EPS |
- Harriet Lane Handbook: Nodal escape/junctional rhythm is common after atrial surgery; often requires no treatment; if rate slow enough, may require pacemaker.
---
## 13.8 ICU Patients
- Common causes: hypoxia, electrolyte disturbances, catecholamine infusions, post-cardiac surgery
- Monitor continuously; address metabolic causes
- If caused by sedative/analgesic overdose → reduce doses
- Temporary pacing readily available in ICU
---
## 13.9 Electrolyte Abnormalities
| Electrolyte Disturbance | Effect on AV Junction | ECG Findings |
|------------------------|----------------------|-------------|
| **Hyperkalemia** | Depresses SA node > AV junction → junctional escape | Peaked T waves, wide QRS, absent P waves (severe) |
| **Hypokalemia** | Enhances automaticity | Flat T waves, U waves, increased ectopy |
| **Hypomagnesemia** | Enhances automaticity; interacts with digoxin toxicity | Varies |
| **Hypocalcemia** | Prolonged QT, conduction disturbance | Long QT, Chvostek/Trousseau signs |
---
# 14. COMPLICATIONS
| Complication | Mechanism | Management |
|-------------|-----------|------------|
| **Syncope** | Inadequate cerebral perfusion at slow rates | Emergency pacing |
| **Pre-syncope / Falls** | Cerebral hypoperfusion | Treat underlying rhythm |
| **Heart failure** | Loss of atrial kick + rate issues → ↓ CO | Rate control/restoration + diuretics |
| **Hypotension** | ↓ CO due to bradycardia or tachycardia | Pharmacological support + pacing |
| **AV dyssynchrony** | Loss of coordinated AV contraction | Restore AV synchrony (DDD pacing) |
| **Tachycardia-induced cardiomyopathy** | Prolonged junctional tachycardia | Rate control + treat cause |
| **Cardiogenic shock** | Severe compromise of CO | ICU; inotropes; pacing |
| **Progression to complete AV block** | Worsening conduction disease | Permanent pacemaker |
| **Asystole** | Failure of all escape mechanisms | CPR; emergent pacing |
| **Ventricular tachycardia/fibrillation** | In context of digoxin toxicity | Fab fragments; lidocaine |
---
# 15. PROGNOSIS
## 15.1 Benign vs. Pathological Junctional Rhythm
| Feature | Benign | Pathological |
|---------|--------|-------------|
| Clinical context | Athletes, sleep, vagal | Post-MI, post-surgery, digoxin toxicity |
| Rate | 40-60 bpm; normal exercise response | Persistent bradycardia or tachycardia |
| Symptoms | Asymptomatic | Symptomatic (syncope, CHF, hypotension) |
| Structural heart disease | No | Often yes |
| Reversibility | Yes (resolves with activity/treatment) | Variable |
| Treatment needed | No | Often yes |
| Prognosis | Excellent | Depends on underlying cause |
---
## 15.2 Prognostic Factors
| Factor | Better Prognosis | Worse Prognosis |
|--------|-----------------|-----------------|
| Underlying cause | Reversible (drugs, vagal, inferior MI) | Irreversible (SSS, advanced CHD) |
| Heart rate | 40-60 (junctional escape) | < 40 (junctional bradycardia) |
| LV function | Preserved EF | Reduced EF (< 35%) |
| Structural heart disease | Absent | Present |
| Response to atropine | Good | Poor (suggests infranodal block) |
| Response to reperfusion (MI) | Resolves | Persists despite reperfusion |
| Duration | Transient | Persistent |
| Age | Younger | Older with comorbidities |
---
## 15.3 Specific Prognostic Points
- **Inferior MI with junctional/AV block:** Usually transient (resolves 2-7 days post-reperfusion); permanent pacemaker needed in < 5% of cases. Good prognosis with revascularization.
- **POJET:** Mortality if untreated can be significant; with modern management (cooling, amiodarone, pacing) mortality < 5%. Usually resolves by day 3-5 post-operatively.
- **Congenital JET:** Higher mortality in infancy without treatment; catheter ablation achieves cure in ~70-80% but carries risk of AV block.
- **Digoxin-induced NPJT:** Excellent prognosis once digoxin discontinued and electrolytes corrected.
- **Sick sinus syndrome with junctional escape:** Progressive; permanent pacemaker greatly improves symptoms and quality of life. Minimal effect on survival unless associated with VT.
---
# QUICK REFERENCE SUMMARY CARD
```
╔══════════════════════════════════════════════════════════════════════════╗
║ JUNCTIONAL RHYTHM - QUICK REFERENCE ║
╠══════════════════════════════════════════════════════════════════════════╣
║ TYPE RATE ECG HALLMARK KEY CAUSE ║
║ ─────────────────────────────────────────────────────────────────────── ║
║ Junctional escape 40-60 No P / retrograde P SSS, AV block, ║
║ Narrow QRS vagal, drugs ║
║ Accelerated JR 60-100 Retrograde P or Digoxin toxicity, ║
║ AV dissociation inferior MI, post-op ║
║ Junctional tachy >100 P < V (AV block) Digoxin, post-surgery ║
║ Narrow, regular ║
║ POJET 170-260 V rate > A rate Congenital heart Sx ║
║ Congenital JET 150-300 Incessant, narrow Congenital, neonatal ║
╠══════════════════════════════════════════════════════════════════════════╣
║ STABLE → Find cause → Treat cause ║
║ UNSTABLE → O2 + IV + Monitor → Atropine 0.5mg IV → Dopamine/Epi → ║
║ Transcutaneous → Transvenous Pacing ║
╠══════════════════════════════════════════════════════════════════════════╣
║ KEY DIFFERENTIALS: ║
║ Narrow QRS slow rhythm → Junctional vs. Sinus bradycardia vs. CHB ║
║ Wide QRS slow rhythm → Idioventricular vs. Ventricular escape ║
║ Junctional tachycardia → AVNRT vs. atrial tachycardia ║
╠══════════════════════════════════════════════════════════════════════════╣
║ NEVER cardiovert digoxin-induced arrhythmias (→ refractory VF) ║
║ Atropine ineffective for infranodal block → go straight to pacing ║
║ POJET: V rate > A rate (opposite of complete heart block) ║
║ Inferior MI JR: usually resolves with reperfusion; pacing rarely needed ║
╚══════════════════════════════════════════════════════════════════════════╝
```
---
## REFERENCES
1. Tintinalli JE, et al. *Tintinalli's Emergency Medicine: A Comprehensive Study Guide*, 9th ed. McGraw-Hill. Chapter 18, p. 147 (Tables 18-6, 18-7).
2. Harrison's Principles of Internal Medicine, 22nd Edition (2025). McGraw Hill Medical. Chapter 253, p. 1976.
3. Marx JA, et al. *Rosen's Emergency Medicine: Concepts and Clinical Practice*, 9th ed. Elsevier.
4. Harriet Lane Handbook, 23rd ed. Johns Hopkins Hospital. p. 234.
5. Tanski S, et al. *Frameworks for Internal Medicine*. Wolters Kluwer. Chapter 1.
6. LITFL ECG Library. Burns E, Buttner R. Accelerated Junctional Rhythm, Junctional Escape Rhythm. https://litfl.com/accelerated-junctional-rhythm-ajr
7. StatPearls. *Junctional Rhythm*. NCBI Bookshelf NBK507715.
8. Sasikumar N, et al. "Diagnosis and management of junctional ectopic tachycardia." PMC8457265 (2021).
9. 2015 ACC/AHA/HRS Guideline for Management of Adult Patients With Supraventricular Tachycardia.
10. Page RL, et al. "2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia." *JACC* 2016;67(13):e27-e115.
---
*Notes compiled: July 14, 2026 | For MD Medicine Board Preparation*
I dont want pdf just paste things here
JUNCTIONAL RHYTHM
Comprehensive MD Medicine Notes
Sources: Tintinalli's Emergency Medicine, Harrison's Principles 22E (2025), Rosen's Emergency Medicine, Harriet Lane Handbook, Frameworks for Internal Medicine, LITFL ECG Library, StatPearls
TABLE OF CONTENTS
- Definition and Anatomy
- Electrophysiology
- Classification
- Etiology
- ECG Diagnosis
- ECG Differential Diagnosis
- Clinical Features
- Diagnostic Evaluation
- Approach Algorithm
- Acute Management
- Long-Term Treatment
- Drug-Induced Junctional Rhythm
- Special Situations
- Complications
- Prognosis
1. DEFINITION AND ANATOMY
1.1 Definition
- The SA node rate falls below the intrinsic rate of the AV junction, OR
- SA node impulses are blocked from reaching the AV node
- Escape: 40-60 bpm
- Accelerated: 60-100 bpm
- Tachycardia: >100 bpm
- Tintinalli's Emergency Medicine, p. 147
1.2 Anatomy and Physiology of the AV Junction
┌─────────────────────────────────┐
│ RIGHT ATRIUM │
│ [SA NODE] ────────────────────►│──► Left Atrium
│ (60-100 bpm) │
│ │ │
│ ▼ Internodal Tracts │
│ (Anterior, Middle, Posterior) │
└─────────┼───────────────────────┘
╔═════════╪═════════════════════╗
║ AV JUNCTION ║
║ ┌──────▼──────────────────┐ ║
║ │ AV NODE │ ║ ← Compact Node (Koch's Triangle)
║ │ (40-60 bpm) │ ║
║ └──────┬──────────────────┘ ║
║ │ ║
║ ┌──────▼──────────────────┐ ║
║ │ BUNDLE OF HIS │ ║
║ │ (40-60 bpm) │ ║
╚═════════════════════════════╝
│
┌───────┴──────────────────┐
│ LEFT BB RIGHT BB │
│ │ │ │
│ PURKINJE FIBERS │
│ (Ventricles: 20-40 bpm) │
└──────────────────────────┘
Key Anatomical Points
| Point | Detail |
|---|---|
| AV Node location | Floor of right atrium; apex of Koch's Triangle |
| Koch's Triangle borders | Tendon of Todaro + Tricuspid annulus + Coronary sinus ostium |
| AV node size | ~1 × 3 × 5 mm |
| Blood supply | Right coronary artery (RCA) in ~90% |
| Clinical implication | Inferior MI (RCA territory) → AV node ischemia → junctional rhythm |
| Autonomic supply | Rich sympathetic AND parasympathetic innervation |
1.3 Normal Pacemaker Hierarchy
| Pacemaker Site | Intrinsic Rate | Notes |
|---|---|---|
| SA Node | 60-100 bpm | Dominant pacemaker; sympathetic/vagal modulation |
| AV Node / His Bundle | 40-60 bpm | Secondary; "escape" at this rate |
| Bundle Branches | 25-40 bpm | Rarely seen |
| Purkinje / Ventricular Myocardium | 20-40 bpm | Last resort; produces wide QRS |
Pearl: Higher pacemakers suppress lower ones by overdrive suppression - each depolarization from above resets the lower site's clock. When the higher pacemaker fails, the lower site "escapes."
1.4 Escape Rhythm vs. Accelerated Rhythm
| Feature | Escape Rhythm | Accelerated Rhythm |
|---|---|---|
| Mechanism | SA failure/block → AV junction emerges | Enhanced AV junction automaticity overrides SA node |
| Rate | 40-60 bpm | 60-100 bpm |
| Context | Protective (prevents asystole) | Pathological usurpation |
| ECG appearance | P absent or retrograde | P absent, retrograde, or AV dissociation |
| Example cause | Sinus arrest, vagal tone | Digoxin toxicity, inferior MI |
| Treatment | Treat underlying cause; pace if symptomatic | Treat underlying cause |
| Danger | If suppressed → asystole | Usually hemodynamically tolerated |
2. ELECTROPHYSIOLOGY
2.1 Automaticity of the AV Junction
- Phase 4 spontaneous depolarization (pacemaker potential) occurs in AV nodal and His bundle cells
- Driven by the "funny current" (I_f) through HCN channels, plus slow inward Ca²⁺ and reduced K⁺ outward currents
- Normally suppressed by faster SA node impulses (overdrive suppression)
- AV junction automaticity is slower (40-60 bpm) than SA node → acts as backup
ACTION POTENTIAL OF AV NODAL CELL:
Phase 4: Spontaneous slow diastolic depolarization
I_f (HCN4) → Na+ enters → slope determines rate
Ca2+ (T-type) contributes to late Phase 4
Phase 0: Ca2+ dependent (slow upstroke, not Na+)
Unlike atrial/ventricular cells
Phase 3: K+ repolarization (I_K)
Autonomic modulation:
• Sympathetic (beta-1) → ↑ I_f slope → faster Phase 4 → faster rate
• Parasympathetic (muscarinic M2) → ↓ I_f, ↑ I_K → slower Phase 4 → slower rate
2.2 Escape Mechanism
NORMAL:
SA node fires at 75 bpm
→ depolarizes AV junction before it spontaneously fires
→ AV junction clock continuously reset → SUPPRESSED
SA NODE FAILURE OR BLOCK:
SA rate drops below 40-60 bpm
OR
SA impulse blocked at AV node
↓
AV junction fires spontaneously
(escape beat → sustained = escape rhythm)
↓
Rescue of cardiac output
- The escape interval = time from last sinus beat to first junctional beat
- Multiple junctional escape beats = junctional escape rhythm
- This is a PROTECTIVE mechanism - never suppress it without addressing the cause
2.3 Enhanced Automaticity
- Abnormal increase in Phase 4 slope → AV junction fires faster than SA node
- Causes: digoxin toxicity, catecholamine excess, ischemia, fever, post-cardiac surgery
- The enhanced junctional pacemaker "usurps" the SA node
- Results in: Accelerated junctional rhythm (60-100 bpm) or Junctional tachycardia (>100 bpm)
2.4 Re-entry Mechanism
- AVNRT uses dual AV nodal pathways:
- Fast pathway (anterior, short RP interval)
- Slow pathway (posterior, long RP interval)
- Most common SVT (~60% of all SVT)
- Re-entrant junctional rhythms: paroxysmal, abrupt onset/termination
- Distinct from "true" automatic junctional tachycardia
DUAL AV NODAL PATHWAYS (AVNRT):
ATRIA
│
┌─────┴──────┐
FAST│ │SLOW
PATHWAY PATHWAY
(short refractory) (long refractory)
│ │
└─────┬───────┘
│
HIS
BUNDLE
Typical AVNRT: ↓ slow → ↑ fast (short RP)
Atypical AVNRT: ↓ fast → ↑ slow (long RP)
2.5 Influence of Autonomic Tone
| Autonomic State | SA Node Effect | AV Junction Effect | Net Result |
|---|---|---|---|
| Increased vagal tone (sleep, athletes, vasovagal) | ↓↓ firing | ↓ firing (less suppressed) | Junctional escape emerges |
| Sympathetic stimulation | ↑↑ firing | ↑ firing | SA dominates; junctional suppressed |
| Beta-blocker | ↓ SA rate | Minimal effect | Junctional escape may emerge |
| Digoxin toxicity | ↓ SA rate + SA block | ↑↑↑ enhanced automaticity | Accelerated junctional rhythm |
| Atropine | ↑ SA rate | Relative suppression | Restores sinus rhythm |
| Calcium channel blockers | ↓ SA + AV node | Both slowed | Junctional escape |
3. CLASSIFICATION
3.1 Overview Table
| Type | Rate | Mechanism | Clinical Significance |
|---|---|---|---|
| Junctional Bradycardia | < 40 bpm | Severe SA suppression | Hemodynamically compromising; urgent pacing |
| Junctional Escape Rhythm | 40-60 bpm | SA node failure / block | Protective; treat underlying cause |
| Accelerated Junctional Rhythm (AJR) | 60-100 bpm | Enhanced AV junction automaticity | Often digoxin toxicity; investigate |
| Junctional Tachycardia | > 100 bpm | Enhanced automaticity / re-entry | May be hemodynamically significant |
| Non-Paroxysmal Junctional Tachycardia (NPJT) | 70-130 bpm | Enhanced automaticity | Classic in digoxin toxicity; gradual onset |
| Congenital JET | 150-300 bpm | Congenital automaticity defect | Rare; life-threatening in neonates |
| Postoperative JET (POJET) | 170-260 bpm | Surgical trauma to His bundle | Most common early arrhythmia after congenital heart surgery |
3.2 Junctional Escape Rhythm (40-60 bpm)



- Rate: 40-60 bpm (regular)
- P waves: absent, hidden within QRS, or inverted/retrograde (inverted in leads II, III, aVF; upright in aVR)
- QRS: narrow (< 120 ms) unless aberrant conduction
- PR interval: < 120 ms (if P wave before QRS)
- RP interval: very short if P after QRS
- Protective rhythm preventing asystole
- Seen with: sinus bradycardia, SA block, vasovagal, sleep, trained athletes
- Treatment only if symptomatic (rate < 40 or hemodynamic compromise)
3.3 Accelerated Junctional Rhythm (60-100 bpm)



- Rate: 60-100 bpm (regular)
- P waves: inverted in II, III, aVF; may be immediately before, within, or after QRS
- QRS: narrow
- AV dissociation may be present
- Rate slightly irregular = suggests automatic mechanism
- Most commonly: digoxin toxicity (classic presentation)
- Also: inferior MI, myocarditis, cardiac surgery, electrolyte disturbance
- Usually hemodynamically well-tolerated
- Must investigate and treat underlying cause
3.4 Junctional Tachycardia (>100 bpm)
- Rate: >100 bpm (typically 100-180 bpm)
- P waves: inverted/retrograde or dissociated from QRS
- QRS: narrow (unless aberrancy)
- Onset: gradual (automatic) or abrupt (re-entrant)
- Irregular rate variability: suggests automatic mechanism (vs. fixed rate in re-entry)

In junctional tachycardia: more V's than A's (VA block pattern) distinguishes it from AVNRT/ORT. - Harrison's 22E, p. 1976
3.5 Non-Paroxysmal Junctional Tachycardia (NPJT)
- Rate: 70-130 bpm
- Gradual ("warm-up") onset and termination (vs. abrupt in re-entry)
- Classic hallmark of digoxin toxicity AND inferior MI
- May show AV dissociation with independent atrial rate
- Also called "accelerated junctional tachycardia" in the 100-130 bpm range
3.6 Congenital Junctional Ectopic Tachycardia (Congenital JET)
- Rare; autosomal dominant mutations (HCN4 channels)
- Presents in infancy/early childhood
- Rate: 150-300 bpm; often incessant
- Leads to tachycardia-induced cardiomyopathy if untreated
- ECG: narrow QRS, retrograde P waves, AV dissociation common
- Management: amiodarone, propafenone, catheter ablation in resistant cases
- Catheter ablation achieves cure in ~70-80% but carries risk of complete AV block
3.7 Postoperative JET (POJET)

- Most common arrhythmia in first 24-72 hours after congenital heart surgery
- Incidence: 2-8% overall; up to 14% after tetralogy of Fallot or VSD closure
- Mechanism: thermal or mechanical injury to His bundle / AV nodal region
- Rate: 170-260 bpm; AV dissociation present (V rate > A rate)
- KEY ECG: Ventricular rate FASTER than atrial rate (opposite of complete heart block)
- Hemodynamically destabilizing: loss of AV synchrony + fast rate
- Management: surface cooling (fever reduction), IV magnesium, amiodarone, atrial overdrive pacing
4. ETIOLOGY
4.1 Comprehensive Cause Table
| Category | Specific Cause | Mechanism | Notes |
|---|---|---|---|
| PHYSIOLOGICAL | Athletes, sleep, vagal tone | Enhanced vagal tone suppresses SA node | Benign; escape rhythm |
| DRUGS | Digoxin toxicity | Enhanced AV junction automaticity + SA suppression | NPJT; most classic cause |
| Beta-blockers | SA node suppression (beta-1 blockade) | Junctional escape | |
| Calcium channel blockers (diltiazem, verapamil) | SA/AV node Ca2+ channel depression | Escape rhythm | |
| Amiodarone | Complex multi-channel + beta-block effects | Junctional bradycardia | |
| Ivabradine | I_f channel blockade (SA > AV effect) | Junctional escape | |
| Adenosine | Transient AV block (A1 receptor) | Brief 15-30 sec escape; self-terminating | |
| CARDIAC | Inferior wall MI | RCA ischemia → SA and AV node dysfunction | NPJT or escape; may have 3rd degree block |
| Sick sinus syndrome | Degeneration of SA node | Junctional escape; bradycardia-tachycardia syndrome | |
| Sinus arrest | Complete failure of SA node to fire | Junctional escape rescues rhythm | |
| SA exit block | SA fires but impulse blocked | Junctional escape | |
| Complete AV block | No SA impulse reaches ventricles | Junctional escape rhythm (narrow QRS) | |
| 2nd degree AV block | Intermittent block | Intermittent junctional escape | |
| Myocarditis | Inflammatory conduction damage | Any junctional rhythm | |
| Cardiac surgery | Mechanical/thermal injury to His-AV junction | POJET | |
| Congenital heart disease | Structural abnormalities near AV node | Congenital JET | |
| METABOLIC | Hyperkalemia | Depresses SA automaticity preferentially | Junctional escape; peaked T waves |
| Hypokalemia | Enhanced automaticity | Accelerated junctional | |
| Hypomagnesemia | Enhanced automaticity; worsens digoxin toxicity | Accelerated junctional | |
| Hypocalcemia | Conduction disturbance | Bradyarrhythmias | |
| Hypothyroidism | Slowed SA node | Junctional escape | |
| Hypothermia | Global conduction slowing | Osborn waves + junctional rhythm | |
| RESPIRATORY | Hypoxia | SA node ischemia | Junctional escape or tachycardia |
| Sleep apnea | Hypoxia + vagal surges | Nocturnal junctional rhythm | |
| Sepsis/ICU | Autonomic dysregulation | Variable | |
| IDIOPATHIC | No identifiable cause | Unknown | Diagnosis of exclusion |
4.2 Memory Aid
Mnemonic: "DIME-CHASM"
────────────────────────
D - Digoxin toxicity (classic - most important)
I - Inferior MI (RCA territory)
M - Myocarditis
E - Electrolytes (K+, Mg2+, Ca2+)
C - Cardiac surgery (POJET)
H - Hypoxia / Hypothermia
A - Athletes / Autonomic (vagal) tone
S - Sick sinus syndrome / Sinus arrest
M - Medications (beta-blockers, CCBs, amiodarone)
5. ECG DIAGNOSIS
5.1 Stepwise ECG Interpretation
═══════════════════════════════════════════════════════
STEP-BY-STEP ECG APPROACH TO JUNCTIONAL RHYTHM
═══════════════════════════════════════════════════════
STEP 1: CALCULATE THE RATE
────────────────────────────
• Rate = 300 ÷ large squares between R-R peaks
OR = 1500 ÷ small squares between R-R peaks
< 40 bpm → Junctional bradycardia (severe, needs urgent pacing)
40-60 → Junctional ESCAPE rhythm
60-100 → ACCELERATED junctional rhythm
> 100 → Junctional TACHYCARDIA
STEP 2: ASSESS RHYTHM REGULARITY
──────────────────────────────────
• Regular R-R intervals: typical of junctional rhythm
• Slight rate irregularity: suggests AUTOMATIC mechanism
• Abrupt paroxysmal onset/termination: suggests RE-ENTRANT mechanism
STEP 3: ASSESS QRS DURATION
──────────────────────────────
• Narrow QRS (< 120 ms) = supraventricular (junctional or above)
• Wide QRS (≥ 120 ms) = aberrant conduction OR ventricular origin
• KEY: Junctional rhythm should have NARROW QRS
STEP 4: LOOK FOR P WAVES (Most Critical Step)
────────────────────────────────────────────────
Search ALL leads carefully, especially leads II, V1, aVR
4 PATTERNS in junctional rhythm:
┌─────────────────────────────────────────────────────────┐
│ A. NO VISIBLE P WAVES │
│ → P buried within QRS (simultaneous depolarization) │
│ → Most common pattern │
│ → QRS may appear slightly widened or notched │
├─────────────────────────────────────────────────────────┤
│ B. INVERTED P WAVE BEFORE QRS │
│ → Retrograde P (inverted II/III/aVF; upright aVR) │
│ → PR interval VERY SHORT (< 120 ms) │
│ → Retrograde conduction to atria faster than │
│ antegrade to ventricles │
├─────────────────────────────────────────────────────────┤
│ C. P WAVE WITHIN QRS (simultaneous) │
│ → Notching of QRS or pseudo-R' in V1 │
│ → Atria and ventricles depolarize together │
├─────────────────────────────────────────────────────────┤
│ D. INVERTED P WAVE AFTER QRS (in ST segment) │
│ → RP interval: 80-200 ms │
│ → Antegrade conduction faster than retrograde │
└─────────────────────────────────────────────────────────┘
STEP 5: ASSESS AV RELATIONSHIP
────────────────────────────────
• Retrograde P (inverted II/III/aVF) = typical junctional
• Independent P waves "marching through" = AV dissociation
• P rate < QRS rate in junctional tachycardia with AV dissociation
STEP 6: LOOK FOR AV DISSOCIATION FEATURES
────────────────────────────────────────────
• Capture beats: sinus P conducts → produces normal narrow QRS
(PR interval normal/prolonged; QRS morphology changes to sinus)
• Fusion beats: simultaneous junctional + sinus activation
(QRS morphology intermediate between sinus and junctional)
• Variable relationship of P waves to QRS in consecutive beats
STEP 7: CONFIRM WITH 12-LEAD ECG
──────────────────────────────────
Lead II: Best lead for P wave morphology
Lead V1: Biphasic P may be visible
aVR: Upright retrograde P (normally inverted in sinus)
aVF: Inverted retrograde P (normally upright in sinus)
═══════════════════════════════════════════════════════
5.2 Retrograde P Wave Mechanism Diagram
RETROGRADE ATRIAL ACTIVATION - DIAGRAM
════════════════════════════════════════
Normal Sinus:
SA → Atria → AV node → His → Ventricles
P wave UPRIGHT in II, III, aVF
PR interval: 120-200 ms
Direction of depolarization: TOP → BOTTOM
Junctional:
AV node/His → Ventricles (antegrade) AND Atria (retrograde)
Direction of atrial depolarization: BOTTOM → TOP
→ P wave INVERTED in II, III, aVF
→ P wave UPRIGHT in aVR
TIMING VARIANTS:
Case A: Equal speeds
Atria ──────────────────► P
Ventricles ──────────────► QRS (P HIDDEN IN QRS)
Case B: Retrograde faster
Atria ───────► P (inverted)
──────────────► QRS (SHORT PR < 120ms)
Case C: Antegrade faster
Ventricles ──► QRS
──────────────► P (inverted) (P IN ST SEGMENT)
Case D: Retrograde completely blocked
SA node ────────────► P (upright, own rate)
AV junction ─────────► QRS (own rate) (AV DISSOCIATION)
5.3 ECG Gallery with Analysis
ECG 1 - Junctional Escape Rhythm (Three P Wave Patterns)
Analysis:
Top strip: Rate ~50 bpm | P hidden in QRS | No visible P wave
Middle strip: Rate ~50 bpm | Inverted P BEFORE QRS | Short PR < 120ms
Bottom strip: Rate ~50 bpm | Inverted P AFTER QRS | P in ST segment
All: Regular rhythm | Narrow QRS | Escape range (40-60 bpm)
ECG 2 - Junctional Escape (Hidden P) vs. Retrograde P (Labeled)
Analysis:
Top: 46 bpm | P waves hidden (buried in QRS) | Narrow QRS
Bottom: 50 bpm | Retrograde P visible AFTER QRS | RP short
Both: Escape range | Regular | Narrow complex
KEY: Compare T wave morphology between beats - hidden P may
distort the T wave slightly
ECG 3 - Junctional Escape Beat After Sinus Pause (Teaching ECG)
Analysis:
- Sinus rhythm initially → sinus PAUSE (no P wave for long interval)
- After pause: junctional escape beat fires
- Inverted P wave visible AFTER QRS = retrograde P
- This single beat "rescues" the rhythm from prolonged asystole
- If SA node continues to fail → sustained junctional escape RHYTHM
ECG 4 - Accelerated Junctional Rhythm (12-Lead)
Analysis (LITFL):
- Rate: ~78 bpm (accelerated junctional range: 60-100)
- Rhythm: Regular
- QRS: Narrow in all 12 leads
- P waves: Not clearly preceding QRS
- Retrograde P may be buried in QRS or T wave
- Leads II, III, aVF: check for inverted P
- Cause: enhanced AV junction automaticity
ECG 5 - AJR Rhythm Strip (Inverted P Before QRS)
Analysis (LITFL):
- Rate: ~85 bpm (accelerated junctional)
- Rhythm: Regular
- P wave: INVERTED (retrograde) immediately BEFORE QRS
- PR interval: Very short (< 120 ms) - note how different from sinus
- QRS: Narrow
- Diagnosis: Accelerated Junctional Rhythm, retrograde P before QRS
ECG 6 - Labeled Inverted P Wave (Classic Teaching ECG)
Teaching Points:
- Retrograde P (red label) = inverted in lead II
- P wave BEFORE QRS: retrograde conduction to atria completes
before ventricular activation → short PR < 120ms
- Compare to sinus rhythm: sinus P is UPRIGHT in II
- Distinguish from: low atrial rhythm (P upright but non-sinus shape)
and from AVNRT (where P is buried IN QRS typically)
ECG 7 - AVNRT vs. AJR (Retrograde P Pattern)
Analysis (LITFL - AVNRT pattern for comparison):
- Rate: >150 bpm (tachycardia range)
- Retrograde P waves at END of QRS / just after
- Pseudo-R' in V1 (retrograde P distorts terminal QRS)
- Pseudo-S waves in inferior leads
- Compare with junctional tachycardia: similar appearance
but junctional automatic tachy has gradual onset/offset
and slight rate variation
5.4 AV Dissociation - Detailed Explanation
- Definition: Independent firing of atria (SA node) and ventricles (junctional pacemaker)
- P waves and QRS are unrelated - P waves "march through" at their own rate
- Capture beats: Sinus P reaches AV node at right moment → conducts → normal QRS (narrower, normal PR) - proves AV dissociation
- Fusion beats: Simultaneous activation from sinus + junctional → intermediate QRS morphology
AV DISSOCIATION ON ECG:
Beat: 1 2 3 4 5 6 7
P: P P P P (SA rate: 50 bpm)
QRS: Q Q Q (Junctional rate: 65 bpm)
Notice: P waves are not followed by QRS every time
QRS complexes are not preceded by P waves consistently
P gradually "walks through" different positions relative to QRS
Capture beat (beat 5 in example):
P ──► QRS: P happens to precede QRS by 120-200ms → conducts
→ Normal appearing QRS (same morphology as sinus)
→ This "capture" beat PROVES AV dissociation
5.5 Summary ECG Features Table
| Feature | Junctional Escape (40-60) | Accelerated Junctional (60-100) | Junctional Tachy (>100) |
|---|---|---|---|
| Rate | 40-60 bpm | 60-100 bpm | >100 bpm |
| Rhythm | Regular | Regular | Regular (slight variability if automatic) |
| P waves | Absent/retrograde/hidden | Absent/retrograde | Absent/retrograde/dissociated |
| PR interval | <120ms (if P before QRS) | <120ms | Short or absent |
| RP interval | Very short (if P after) | Very short | Short |
| QRS | Narrow (<120ms) | Narrow (<120ms) | Narrow (<120ms) |
| AV dissociation | Possible | Possible | Common |
| Onset | Gradual | Gradual | Gradual (auto) or abrupt (reentry) |
Sources: Tintinalli's Emergency Medicine Table 18-6; Harrison's 22E; LITFL ECG Library
6. ECG DIFFERENTIAL DIAGNOSIS
6.1 Bradycardia Differential Comparison
| Feature | Junctional Escape | Sinus Bradycardia | Sinus Arrest | SA Exit Block | Ventricular Escape | Complete Heart Block |
|---|---|---|---|---|---|---|
| Rate | 40-60 bpm | <60 bpm | Variable | Variable | 20-40 bpm | Varies |
| P waves | Absent/retrograde/inverted | Upright, before every QRS | Absent during arrest | Absent during block | Usually absent | Present but dissociated |
| PR interval | Short/absent | Normal (120-200ms) | N/A | Normal when present | N/A | No relationship |
| QRS | Narrow | Narrow | Narrow (escape) | Narrow | Wide (>120ms) | Narrow (junctional) or Wide (ventricular) |
| Rhythm | Regular | Regular | Irregular (pauses) | Irregular (grouped) | Regular | Regular but P and QRS independent |
| Key clue | Inverted P/no P + narrow QRS | Normal sinus P + long PR | Long pause, no P wave | Pauses = multiples of PP | Wide QRS + very slow rate | P rate > QRS rate, no conduction |
| Atropine response | Good | Good | Good | Good | Poor | Poor (infranodal) |
6.2 Tachycardia Differential Comparison
| Feature | Junctional Tachy (Auto) | AVNRT | AVRT (ORT) | Atrial Tachycardia | Sinus Tachycardia |
|---|---|---|---|---|---|
| Rate | 100-180 bpm | 150-250 bpm | 150-250 bpm | 150-250 bpm | 100-150 bpm |
| Onset/termination | Gradual (warm-up) | Abrupt | Abrupt | Gradual or abrupt | Gradual |
| P wave | Retrograde/dissociated | Retrograde, buried IN QRS | Retrograde, AFTER QRS | Ectopic P BEFORE QRS | Upright, before QRS |
| RP relationship | Variable | Very short RP (<80ms) | Short RP (>70ms, RP<PR) | Long RP | Long RP |
| Adenosine response | May slow/terminate | Terminates | Terminates | May unmask/slow | Transient slowing |
| AV dissociation | Common | Rare | Absent | Possible | No |
| Rate variability | Yes (automatic) | No | No | May vary | Varies with physiology |
| Delta wave (resting ECG) | No | No | Yes (if WPW) | No | No |
| Carotid sinus massage | Variable | Terminates | Terminates | Rate slows or unaffected | Temporary slowing |
6.3 Junctional Escape vs. Idioventricular Rhythm (Most Important Differential)
| Feature | Junctional Escape Rhythm | Idioventricular Rhythm (IVR) |
|---|---|---|
| Origin | AV node / His bundle | Ventricle (Purkinje fibers) |
| Rate | 40-60 bpm | 20-40 bpm |
| QRS | Narrow (<120 ms) | Wide (>120 ms) |
| QRS morphology | Normal | Bizarre; LBBB or RBBB pattern |
| P waves | Absent/retrograde | Usually absent or dissociated |
| Clinical context | SA node failure | Complete heart block, late rescue |
| Treatment urgency | Moderate | HIGH - pacing usually needed |
| Atropine response | May help | Usually ineffective |
KEY POINT: Narrow = junctional. Wide = ventricular. This single feature is the most important differentiator.
Source: Tintinalli's Emergency Medicine, Table 18-7
6.4 Accelerated Junctional (AJR) vs. Accelerated Idioventricular (AIVR)
| Feature | AJR | AIVR |
|---|---|---|
| Rate | 60-100 bpm | 50-110 bpm |
| QRS | Narrow | Wide (>120ms) |
| Context | Digoxin toxicity, inferior MI | Post-MI reperfusion, digoxin |
| AV dissociation | Common | Common |
| Capture beats | Present | Present |
| Atropine response | May help | Minimal |
6.5 Low Atrial Rhythm vs. Junctional Rhythm
| Feature | Low Atrial Rhythm | Junctional Rhythm |
|---|---|---|
| Origin | Low right atrium (near AV node) | AV node/His bundle |
| P wave | Upright but different shape (non-sinus) | Inverted in II/III/aVF |
| PR interval | Short but may be near 120ms | Very short (<120ms) or absent |
| Rate | Usually 50-100 bpm | Depends on type |
| Treatment | Usually observe | Depends on type |
7. CLINICAL FEATURES
7.1 Symptoms
| Symptom | Mechanism | Notes |
|---|---|---|
| Asymptomatic | Adequate CO at escape rates | Most junctional escape rhythms |
| Fatigue/Weakness | Reduced cardiac output | Common |
| Palpitations | Awareness of arrhythmia | Accelerated/tachycardia forms; sensation of "neck pounding" |
| Lightheadedness/Presyncope | Reduced cerebral perfusion | Slower rates or compromised hearts |
| Syncope | Severe bradycardia or initial long pause before escape | Less common |
| Dyspnea | Reduced CO → pulmonary congestion | Advanced or tachycardia-induced cardiomyopathy |
| Neck pulsations | Cannon A waves (AV dissociation) | Classic bedside sign |
| Chest discomfort | Underlying ischemia or reduced CO | Especially in inferior MI context |
7.2 Signs - Cannon A Waves (Pathognomonic of AV Dissociation)
MECHANISM OF CANNON A WAVES:
═════════════════════════════════════════════════════
NORMAL SEQUENCE:
Atria contract (P wave) → AV valves OPEN → blood flows to ventricles
→ A wave in JVP = normal small wave
AV DISSOCIATION IN JUNCTIONAL RHYTHM:
Atria contract at their own rate (SA node)
Ventricles contract at junctional rate
SOMETIMES: Atria contract when AV valves are CLOSED
(ventricle already contracting)
↓
Blood CANNOT exit atria → reflected back
↓
Large pressure wave transmitted to jugular veins
↓
VISIBLE CANNON A WAVE in neck
PATTERN:
• Regular cannon A waves:
→ AV dissociation affects EVERY beat
→ Seen in junctional tachycardia with complete AV dissociation
• Intermittent cannon A waves:
→ Only when P wave falls just before/during QRS
→ Seen in incomplete AV dissociation
→ Classic physical finding for diagnosing AV dissociation at bedside
7.3 Hemodynamic Consequences
| Hemodynamic Effect | Mechanism | Consequence |
|---|---|---|
| Loss of atrial "kick" | No synchronized atrial contraction | ↓ CO by 15-25% |
| Reduced diastolic filling | Tachycardia → short diastole | ↓ Stroke volume |
| Hypotension | Reduced CO | Dizziness, presyncope, shock |
| Heart failure | Prolonged junctional tachycardia | Tachycardia-induced cardiomyopathy |
| Cardiogenic shock | Severe bradycardia/tachycardia in compromised LV | Emergency pacing needed |
| AV dyssynchrony | Loss of atrial kick | Significant in poor LV function (EF <35%) |
| Mitral regurgitation | AV dyssynchrony | Functional MR in some patients |
7.4 Clinical Pearls
Pearl 1: In a patient with suspected AV dissociation - lay them flat and watch the jugular vein. Intermittent large "cannon" pulsations clinch the diagnosis without any test.
Pearl 2: A junctional rhythm in a patient on digoxin means digoxin toxicity until proven otherwise. Stop digoxin immediately. Measure serum level and potassium.
Pearl 3: After inferior STEMI, a junctional escape rhythm is a protective rhythm - treat with reperfusion (PCI/lysis) and monitor. Do not rush to pace unless hemodynamically compromised.
Pearl 4: POJET after congenital heart surgery: ventricular rate > atrial rate is the hallmark. Distinguish from complete heart block where atrial rate > ventricular rate.
Pearl 5: An athlete with heart rate 45 and junctional escape on ECG during rest/sleep is NORMAL - do not workup or treat.
8. DIAGNOSTIC EVALUATION
8.1 History - Key Questions
| Question | Relevance |
|---|---|
| Drug history (digoxin, beta-blockers, CCBs, amiodarone, ivabradine) | Drug-induced; dose adjustment needed |
| Onset: gradual vs. sudden | Automatic vs. re-entrant mechanism |
| Recent cardiac surgery/catheterization | POJET, surgical trauma |
| Chest pain, diaphoresis, nausea | Inferior MI |
| Exercise tolerance | Athletes may have benign junctional escape |
| Sleep history (snoring, apnea) | Sleep apnea → nocturnal junctional rhythm |
| Family history of conduction disease | Congenital JET, SSS |
| Visual changes (yellow/green) | Digoxin toxicity |
| Thyroid symptoms | Hypothyroidism |
8.2 Physical Examination
| Finding | Significance |
|---|---|
| Heart rate and rhythm | Bradycardia or tachycardia; regularity |
| Blood pressure | Hemodynamic compromise? |
| JVP: cannon A waves | AV dissociation (pathognomonic) |
| JVP: elevated | Right heart failure |
| Lungs: crepitations | Left heart failure |
| Signs of inferior MI | RCA territory ischemia |
| Yellow/green xanthopsia | Digoxin toxicity |
| Cool extremities + delayed cap refill | Reduced cardiac output |
| Peripheral edema | Heart failure |
| Chvostek/Trousseau signs | Hypocalcemia |
8.3 Laboratory Investigations
| Test | Indication | Key Findings |
|---|---|---|
| CBC | Routine | Anemia (contributing hypoxia); WBC for infection/myocarditis |
| Serum K+ | ALL patients | Hyperkalemia (depresses SA); Hypokalemia (worsens digoxin toxicity) |
| Serum Mg2+ | ALL patients | Hypomagnesemia enhances automaticity; synergizes digoxin toxicity |
| Serum Ca2+ | All patients | Hypocalcemia → conduction disturbance; hypercalcemia → bradycardia |
| Serum Na+, Cl-, HCO3- | Metabolic panel | Acidosis, electrolyte imbalance |
| TSH, fT4 | Bradycardia workup | Hypothyroidism → SA suppression; hyperthyroidism → tachycardia |
| Cardiac troponin | Suspected MI/myocarditis | Elevation confirms myocardial injury |
| Serum digoxin level | Digoxin use | Therapeutic: 0.5-0.9 ng/mL; toxic: >2.0 ng/mL |
| ABG | Respiratory symptoms or ICU | Hypoxia, acidosis affecting automaticity |
| BNP/NT-proBNP | Heart failure symptoms | Elevated in decompensation |
| Lactate | Hemodynamic compromise | Tissue hypoperfusion marker |
8.4 Cardiac Investigations
| Investigation | Indication | Key Findings |
|---|---|---|
| 12-lead ECG | ALL patients (first test) | Rate, rhythm, P wave morphology, QRS duration, intervals, ST changes |
| Serial ECG | MI, evolving block | Dynamic ST changes; progression of AV block |
| Continuous telemetry | Inpatients, post-surgery | Captures intermittent rhythms; detects progression |
| 24-hour Holter | Outpatients with symptoms | Symptom-rhythm correlation; burden of arrhythmia |
| Event recorder | Infrequent palpitations | Long-term monitoring (days-weeks) |
| Implantable loop recorder | Unexplained syncope | Long-term monitoring (up to 3 years) |
| Echocardiography | All with junctional rhythm | Structural disease, LV function, pericardial effusion, wall motion |
| Exercise stress test | Chronotropic evaluation | Rate response; rule out ischemia |
| Electrophysiology study (EPS) | Recurrent tachycardia; pre-ablation | Map re-entrant circuit; measure HV interval; ablation target |
| Cardiac MRI | Myocarditis, cardiomyopathy | Fibrosis, inflammation (late gadolinium enhancement) |
| Coronary angiography | Suspected ischemic cause | Coronary anatomy; PCI if indicated |
9. APPROACH ALGORITHM
══════════════════════════════════════════════════════════════════
CLINICAL APPROACH TO JUNCTIONAL RHYTHM
══════════════════════════════════════════════════════════════════
PATIENT WITH SUSPECTED JUNCTIONAL RHYTHM
│
▼
┌─────────────────┐
│ 12-LEAD ECG │ ← First and most important test
└────────┬────────┘
│
┌─────────────────┼─────────────────┐
▼ ▼ ▼
Narrow QRS + Wide QRS + Narrow QRS +
absent/ slow rate rate >100
retrograde P (wide)
│ │ │
JUNCTIONAL Consider: JUNCTIONAL
RHYTHM Ventricular TACHYCARDIA
escape,
Complete HB
│
┌────────▼─────────┐
│ HEMODYNAMICALLY │
│ STABLE OR NOT? │
└───┬──────────┬───┘
│ │
STABLE UNSTABLE
(BP OK, (Hypotension,
symptoms syncope,
mild/none) AMS, CHF, angina)
│ │
│ ▼
│ ┌─────────────────────────────┐
│ │ EMERGENCY TREATMENT: │
│ │ • O2, IV access, monitoring │
│ │ • Atropine 0.5mg IV (if brady)│
│ │ • Dopamine/Epinephrine │
│ │ • Transcutaneous pacing │
│ │ → Transvenous pacing │
│ └─────────────┬───────────────┘
│ │
│ STABILIZE FIRST
│ THEN investigate cause
│
▼
IDENTIFY REVERSIBLE CAUSE
┌──────────┬──────────┬──────────┬──────────┐
▼ ▼ ▼ ▼ ▼
Drugs Inferior Electrolyte Cardiac Vagal/
(digoxin, MI imbalance surgery Athletic
BB, CCB)
│
▼
REVERSIBLE CAUSE?
┌───────────────────────────┐
│ YES → Treat cause: │
│ • Stop offending drug │
│ • Reperfuse MI │
│ • Correct electrolytes │
│ • Wait (vagal/post-op) │
└────────────┬──────────────┘
│
▼
REASSESS ECG + SYMPTOMS
┌────────────────────────┐
│ Resolved → Discharge │
│ with follow-up │
└────────────────────────┘
│
(Persists/No cause)
│
▼
┌────────────────────────┐
│ PERMANENT PACEMAKER │
│ CONSIDERATION │
│ (if symptomatic) │
└────────────────────────┘
══════════════════════════════════════════════════════════════════
10. ACUTE MANAGEMENT
10.1 Initial Stabilization (ALL Patients)
ABC APPROACH:
─────────────────────────────────────────────────────────
A - Airway: Ensure patent; intubate if Glasgow Coma Score ≤ 8
B - Breathing: O2 via nasal cannula (2-4 L/min) or mask
Target SpO2 > 94%; correct hypoxia (common cause!)
C - Circulation:
• Large bore IV access (18G or larger, bilateral if unstable)
• Continuous cardiac monitor (12-lead telemetry if available)
• 12-lead ECG STAT
• Non-invasive BP monitoring; arterial line if unstable
• Labs: electrolytes, digoxin level, troponin, ABG, CBC
• IV fluid challenge if hypotensive (250mL normal saline)
─────────────────────────────────────────────────────────
10.2 Stable Patient Management
| Situation | Specific Action |
|---|---|
| Asymptomatic junctional escape rhythm | Monitor; investigate cause; no acute drug treatment |
| Digoxin toxicity | Stop digoxin immediately; check K+ and correct; Fab if severe |
| Beta-blocker/CCB excess | Stop drug; glucagon/calcium IV if overdose |
| Inferior MI | Immediate reperfusion (PCI/thrombolysis); atropine if symptomatic bradycardia |
| Electrolyte cause | IV potassium (if K+<3.0: 10-20mEq/hr IV); IV magnesium sulfate 2g over 10-20min |
| Vagal (athlete, sleep) | Reassurance; no treatment; routine follow-up |
| Post-cardiac surgery (slow JR) | Monitor; temporary pacing if rate <40 or hemodynamic compromise |
| POJET | Cooling + magnesium + amiodarone + atrial overdrive pacing above junctional rate |
10.3 Unstable Patient - Emergency Algorithm (ACC/AHA/ACLS)
UNSTABLE BRADYCARDIA PROTOCOL
(Junctional Bradycardia/Escape with Hemodynamic Compromise)
════════════════════════════════════════════════════════════
Signs of instability:
✓ Hypotension (SBP < 90 mmHg)
✓ Altered mental status
✓ Signs of heart failure (pulmonary edema)
✓ Ongoing ischemic chest pain
✓ Syncope / near-syncope
──────────────────────────────────────────────────────────
FIRST LINE: ATROPINE
──────────────────────────────────────────────────────────
Dose: 0.5 mg IV bolus
Repeat: Every 3-5 minutes if no response
Maximum: 3 mg total (0.04 mg/kg)
Mechanism: Blocks muscarinic receptors
→ removes vagal brake
→ increases SA node rate
→ enhances AV conduction
IMPORTANT NOTES:
⚠ Less effective for INFRANODAL block
(If no response to atropine → go directly to pacing)
⚠ NOT effective in digoxin-induced junctional rhythm
(May worsen or cause paradoxical bradycardia)
⚠ Avoid in cardiac transplant patients
(Denervated heart; may cause paradoxical worsening)
──────────────────────────────────────────────────────────
SECOND LINE: PHARMACOLOGICAL SUPPORT (While preparing pacing)
──────────────────────────────────────────────────────────
DOPAMINE: 2-10 mcg/kg/min IV infusion
Low dose: dopaminergic (renal vasodilation)
2-5 mcg/kg/min: beta-1 (↑HR, ↑contractility)
5-10 mcg/kg/min: alpha + beta (↑BP + ↑HR)
Use when: hypotension + bradycardia both present
EPINEPHRINE: 2-10 mcg/min IV infusion
Alpha + beta-1 + beta-2 agonist
Use when: severe shock + bradycardia
Increases automaticity and rate directly
ISOPROTERENOL: 2-10 mcg/min IV infusion
Pure beta-1 + beta-2 agonist
Very effective at increasing heart rate
Risk: hypotension (beta-2 vasodilation) + VT/VF
Use: bridge to pacing; rarely used alone
──────────────────────────────────────────────────────────
THIRD LINE: PACING (If above fails or severe instability)
──────────────────────────────────────────────────────────
10.4 Pacing Options Comparison
| Type | Access | Setup Time | Reliability | Indication | Key Notes |
|---|---|---|---|---|---|
| Transcutaneous pacing (TCP) | Skin electrodes | < 2 minutes | Moderate | Emergent; first-line while preparing TVP | Painful (requires sedation/analgesia); pacing capture not always reliable; use as bridge |
| Transvenous pacing (TVP) | Femoral/subclavian/IJV vein → RV | 15-30 min | High | Definitive temporary pacing | Needs fluoroscopy/bedside echo guidance; complications: pneumothorax, cardiac perforation |
| Transesophageal pacing | Esophagus | 5-10 min | Atrial only | POJET; atrial pacing only | Cannot pace ventricles; limited use |
| Permanent pacemaker (PPM) | Subcutaneous + transvenous leads | Days-weeks | Definitive | Persistent symptomatic bradycardia | DDD pacing restores AV synchrony; VVI for AF |
Pacing Settings:
- Temporary pacing threshold: usually 5-10 mA (set output at 2x threshold)
- Pacing rate: set at 60-80 bpm for bradycardia
- POJET: overdrive atrial pacing at rate > junctional rate to restore AV synchrony
10.5 Digoxin Toxicity - Specific Protocol
DIGOXIN TOXICITY WITH JUNCTIONAL RHYTHM:
══════════════════════════════════════════
1. STOP digoxin IMMEDIATELY (always first step)
2. Continuous cardiac monitoring in ICU/telemetry
3. Serum digoxin level + electrolytes STAT
4. Correct HYPOKALEMIA (IV KCl: maintain K+ > 4.0 mEq/L)
→ Hypokalemia amplifies digoxin toxicity
5. Correct HYPOMAGNESEMIA (MgSO4 2g IV over 10 min)
6. DO NOT give CALCIUM (worsens digoxin toxicity → "stone heart")
7. Atropine: cautious use; may be less effective or worsen
8. Lidocaine or phenytoin: for ventricular arrhythmias
9. CARDIOVERSION: ⛔ CONTRAINDICATED
→ Risk of refractory ventricular fibrillation
10. DIGOXIN-IMMUNE FAB (Digibind/DigiFab) - ANTIDOTE:
Indications:
✓ Life-threatening arrhythmia (VT/VF)
✓ Serum K+ > 5.0 mEq/L
✓ Ingestion > 10 mg in adults
✓ Serum digoxin > 10-15 ng/mL
Dose: based on serum level × body weight
Onset: 20-30 minutes after infusion
══════════════════════════════════════════
11. LONG-TERM TREATMENT
11.1 Treat Underlying Cause
| Cause | Long-Term Treatment |
|---|---|
| Digoxin toxicity | Discontinue digoxin permanently or reduce dose; use alternative drugs |
| Beta-blocker excess | Dose reduction; switch to lower dose or alternative |
| Sick sinus syndrome | Permanent pacemaker (DDD or DDDR) |
| Inferior MI with persistent block | Permanent pacemaker if block persists >2 weeks post-reperfusion |
| Myocarditis | Treat underlying infection/inflammation; usually resolves |
| Electrolyte disturbance | Maintain normal levels; address underlying cause |
| Congenital JET | Antiarrhythmics (amiodarone, flecainide); catheter ablation |
| POJET | Usually self-limiting by day 3-5; no permanent treatment usually needed |
11.2 Permanent Pacemaker Indications
- Symptomatic bradycardia due to sinus node dysfunction including junctional escape
- Complete AV block (3rd degree) - any rate - with symptoms
- 3rd degree AV block with rate <40 bpm or asystole >3 seconds while awake
- Bradycardia due to required drug therapy with no alternatives
- Post-inferior MI: persistent complete AV block >2 weeks
- Asymptomatic bradycardia with HR <40 during waking hours
- Sinus node dysfunction with HR <40 and symptoms attributable to bradycardia
- Chronotropic incompetence with significant symptoms
11.3 Catheter Ablation
| Indication | Target | Success Rate | Risk |
|---|---|---|---|
| AVNRT | Slow pathway | >95% | AV block 1-3% |
| Congenital JET | His bundle/AV junction region | 70-80% | Complete AV block (requires simultaneous PPM) |
| Automatic junctional tachycardia | Ectopic focus near His | 70-85% | AV block risk |
11.4 Follow-Up Strategy
- Asymptomatic benign junctional rhythm: annual ECG; Holter if symptoms develop
- Post-inferior MI: 24-48 hours monitoring; permanent pacing in <5%
- Post-cardiac surgery: ICU monitoring until stable sinus rhythm
- Pacemaker patients: device clinic at 1 month, 3 months, 6 months, then annually
- Congenital JET survivors: cardiology review every 6-12 months
12. DRUG-INDUCED JUNCTIONAL RHYTHM
12.1 Summary Table
| Drug | Mechanism | Type of JR Caused | Reversal Agent | Management |
|---|---|---|---|---|
| Digoxin | Vagotonic (Na/K-ATPase inhibition) + enhanced AV junction automaticity | NPJT (70-130 bpm); AV dissociation | Digoxin-immune Fab | Stop digoxin; K+/Mg2+ correction; Fab if severe |
| Beta-blockers | Block beta-1 receptors → ↓ SA node rate | Junctional escape (40-60 bpm) | Glucagon 5-10mg IV | Reduce/stop drug; glucagon; high-dose insulin therapy (HIET) if severe |
| Calcium channel blockers (diltiazem, verapamil) | Block L-type Ca2+ channels → ↓ SA + AV node | Junctional escape | Calcium chloride/gluconate IV | Stop drug; CaCl 1g IV or CaGluconate 3g IV; glucagon; HIET |
| Amiodarone | Multi-channel + beta-block + thyroid effects | Junctional bradycardia / escape | No specific antidote | Reduce dose; temporary pacing if symptomatic; long half-life (~50 days) |
| Ivabradine | Blocks HCN4 (I_f) in SA node | Junctional escape (SA slows more than AV junction) | None specific | Reduce dose; stop if symptomatic; short half-life |
| Adenosine | A1 receptor → transient IKAdo ↑ → transient AV block | Brief junctional escape (15-30 sec, self-terminating) | Not needed | Self-terminating; reassure patient |
12.2 Key Drug Pearls
Digoxin is unique: The ONLY drug that causes accelerated junctional rhythm (enhanced automaticity). All other bradycardia-causing drugs produce junctional escape (SA suppression only).
Beta-blocker overdose: Glucagon 5-10mg IV bolus bypasses beta receptor (activates adenylyl cyclase directly). Follow with high-dose insulin-glucose therapy (HIET: 1 unit/kg insulin + dextrose) in severe cases.
CCB overdose: Calcium chloride 1g IV (10mL of 10% solution) preferred over gluconate (3x more elemental calcium per vial). Repeat every 10-20 min up to 3-4 doses. Add HIET for severe cases.
Amiodarone: Half-life ~50 days. Effects persist weeks after stopping. Patient may need temporary pacing bridge for weeks post-discontinuation.
Adenosine effect: The junctional escape seen after adenosine administration for SVT termination is expected and self-terminating (15-30 seconds). Warn the patient beforehand.
13. SPECIAL SITUATIONS
13.1 Inferior Wall Myocardial Infarction
INFERIOR MI AND JUNCTIONAL RHYTHM:
═══════════════════════════════════
• RCA supplies SA node (55%) and AV node (90%) in dominant right
• ST elevation in leads II, III, aVF → RCA territory ischemia
Junctional rhythm may represent:
1. Sinus arrest or severe bradycardia → junctional escape
2. High-degree AV block → junctional escape (narrow QRS)
3. NPJT (enhanced automaticity from ischemia)
ECG Clue (from Frameworks for Internal Medicine):
"Narrow-complex bradycardia, no clearly discernible P waves with 1:1
conduction → junctional escape. If P waves dissociated → sinus with
complete heart block and junctional escape."
Management Priorities:
┌────────────────────────────────────────────────────────┐
│ 1. IMMEDIATE REPERFUSION (PCI preferred; lysis if no PCI)│
│ 2. Aspirin + anticoagulation + P2Y12 inhibitor │
│ 3. Atropine 0.5-1mg IV for symptomatic bradycardia │
│ 4. Temporary pacing if atropine fails │
│ 5. Most cases RESOLVE after reperfusion │
│ 6. Permanent pacemaker RARELY needed (<5% of cases) │
└────────────────────────────────────────────────────────┘
KEY DIFFERENCE from anterior MI:
• Inferior MI block: usually transient (days); AV nodal level;
responds to atropine; narrow QRS escape
• Anterior MI block: often permanent; infranodal; no atropine
response; wide QRS escape; PPM almost always needed
═══════════════════════════════════════════════════════
13.2 Digoxin Toxicity
- Classic presentation: nausea/vomiting + visual disturbances (yellow-green xanthopsia) + bradycardia + NPJT
- Digoxin level >2 ng/mL is toxic (symptoms may occur at lower levels with hypokalemia)
- ECG findings in digoxin toxicity (range):
- Scooped ST depression ("Salvador Dali mustache")
- NPJT with AV dissociation
- PAT with block (multifocal atrial tachycardia + AV block)
- Bidirectional VT (severe toxicity - pathognomonic)
- Hyperkalemia (K+>5 mEq/L) = severe toxicity → immediate Fab fragments
13.3 Cardiac Surgery
| Situation | Junctional Rhythm Type | Management |
|---|---|---|
| Pediatric congenital heart surgery | POJET (170-260 bpm, V>A rate) | Cooling, MgSO4, amiodarone, atrial overdrive pacing |
| Adult CABG/valve surgery | Junctional escape (slow, transient) | Temporary epicardial pacing wires (placed intraoperatively) |
| Septal defect repair | AV block → junctional escape | Temporary then permanent PPM if persistent |
13.4 Congenital Heart Disease
- ASD/VSD repair, tetralogy of Fallot repair → proximity to AV node/His bundle
- Late conduction disease may develop years post-repair
- Long-term monitoring: periodic Holter, 12-lead ECG, cardiology review
- Higher risk of complete AV block and need for PPM later in life
13.5 Athletes
- Highly trained athletes: enhanced vagal tone → marked sinus bradycardia → junctional escape
- Typically: rate 40-55 bpm; asymptomatic; disappears with exercise
- No treatment needed
- Important: do not misdiagnose as pathological
- Pre-participation screening: 12-lead ECG; reassure if junctional escape at rest with normal exercise rate response
- "Detraining test": junctional escape disappears after 6-8 weeks of detraining = confirms benign etiology
13.6 Pregnancy
- Physiological tachycardia during pregnancy; junctional escape uncommon
- Junctional tachycardia management:
- Beta-blockers (metoprolol): relatively safe; first-line
- Flecainide: for resistant cases
- Avoid amiodarone: teratogenic; causes neonatal hypothyroidism
- Adenosine: safe for acute termination of SVT/junctional tachycardia
- Temporary pacing if hemodynamic compromise before delivery
13.7 Pediatric Patients
| Age Group | Common Junctional Rhythm | Notes |
|---|---|---|
| Neonates (<6 months) | Congenital JET | Incessant; tachycardia-cardiomyopathy risk; amiodarone first-line |
| Infants post-CHD surgery | POJET | 170-260 bpm; within 72h; V>A rate; cooling + amiodarone |
| Children (2-12 years) | Junctional escape, AVNRT | Structural disease or vagal; EPS if recurrent tachycardia |
| Adolescents | AVNRT, AJR | Often benign; EPS + ablation if symptomatic |
- Harriet Lane Handbook: "Junctional rhythm is common after atrial surgery; often requires no treatment; if rate slow enough, may require pacemaker." - Harriet Lane Handbook, p. 234
13.8 ICU Patients
- Common causes: hypoxia, sedative drugs, catecholamine excess, electrolyte disturbances, post-surgery
- Monitor continuously; address metabolic causes first
- Reduce sedative/opioid dose if contributing
- Temporary pacing available at bedside; low threshold for pacing if hemodynamically compromised
13.9 Electrolyte Abnormalities
| Electrolyte | Effect on AV Junction | ECG Findings | Treatment |
|---|---|---|---|
| Hyperkalemia | Depresses SA node preferentially → junctional escape | Peaked T waves, wide QRS, absent P waves (severe) | Calcium gluconate (stabilize), insulin+glucose, bicarbonate, dialysis |
| Hypokalemia | Enhances automaticity → accelerated junctional | Flat T waves, prominent U waves, increased ectopy | IV/PO potassium replacement |
| Hypomagnesemia | Enhances automaticity; potentiates digoxin toxicity | Variable | IV MgSO4 2g over 10-20 min |
| Hypocalcemia | Prolonged QT, conduction slowing | Long QT, Chvostek/Trousseau signs | IV calcium gluconate 1-2g |
14. COMPLICATIONS
| Complication | Mechanism | Time Frame | Management |
|---|---|---|---|
| Syncope | Inadequate cerebral perfusion (bradycardia or initial pause) | Acute | Emergency pacing |
| Pre-syncope/Falls | Cerebral hypoperfusion | Ongoing | Treat underlying rhythm |
| Heart failure | Loss of atrial kick + rate issues → ↓ CO | Subacute to chronic | Rate control, diuretics, treat cause |
| Hypotension | ↓ CO from bradycardia or tachycardia | Acute | Pharmacological support + pacing |
| AV dyssynchrony | Loss of coordinated atrial-ventricular contraction | During rhythm | DDD pacing to restore synchrony |
| Tachycardia-induced cardiomyopathy | Prolonged junctional tachycardia (esp. JET) | Weeks to months | Rate control; resolve tachycardia |
| Cardiogenic shock | Severe compromise of CO in vulnerable heart | Acute | ICU; inotropes; emergency pacing |
| Progression to complete AV block | Worsening conduction disease | Variable | Permanent pacemaker |
| Asystole | Failure of all escape mechanisms | Acute emergency | CPR; emergent pacing |
| Ventricular tachycardia/fibrillation | Digoxin toxicity, underlying ischemia | Acute | Fab fragments; lidocaine; defibrillation |
15. PROGNOSIS
15.1 Benign vs. Pathological Junctional Rhythm
| Feature | Benign | Pathological |
|---|---|---|
| Clinical context | Athletes, sleep, increased vagal tone | Post-MI, post-surgery, digoxin toxicity, SSS |
| Rate | 40-60 bpm; normal exercise response (rate rises) | Persistent bradycardia or tachycardia; poor rate response |
| Symptoms | Asymptomatic | Symptomatic: syncope, CHF, hypotension |
| Structural heart disease | Absent | Often present |
| Reversibility | Yes (resolves with activity or treatment) | Variable |
| Treatment needed | No | Often yes |
| Risk of asystole | Minimal | Significant |
| Prognosis | Excellent | Depends on underlying cause |
15.2 Prognostic Factors
| Factor | Better Prognosis | Worse Prognosis |
|---|---|---|
| Underlying cause | Reversible (drugs, vagal tone, inferior MI) | Irreversible (advanced SSS, complete CHD) |
| Heart rate | 40-60 (junctional escape) | <40 (junctional bradycardia) |
| LV function | EF preserved (>50%) | EF reduced (<35%) |
| Structural heart disease | Absent | Present (CHD, cardiomyopathy) |
| Response to atropine | Good → nodal level block | Poor → infranodal block; go to pacing |
| Post-MI reperfusion response | Resolves | Persists despite reperfusion |
| Duration of rhythm | Transient | Persistent |
| Age | Young, no comorbidities | Elderly with multiple comorbidities |
15.3 Specific Prognostic Points
- Usually transient (resolves 2-7 days post-reperfusion)
- Permanent pacemaker needed in <5% of cases
- Good long-term prognosis with successful revascularization
- Mortality if untreated: significant
- With modern management (cooling, amiodarone, pacing): mortality <5%
- Usually resolves by day 3-5 post-operatively
- Untreated: tachycardia-induced cardiomyopathy; high infant mortality
- With catheter ablation: ~70-80% cure but risk of complete AV block
- Requires lifelong cardiology follow-up
- Excellent prognosis once digoxin discontinued and electrolytes corrected
- Rhythm usually resolves within 24-48 hours of stopping digoxin
- Progressive condition
- Permanent pacemaker greatly improves symptoms and quality of life
- Minimal effect on mortality unless associated with VT
QUICK REFERENCE SUMMARY CARD
╔══════════════════════════════════════════════════════════════════════════╗
║ JUNCTIONAL RHYTHM - QUICK REFERENCE CARD ║
╠══════════════════════════════════════════════════════════════════════════╣
║ TYPE RATE ECG KEY FEATURE MAIN CAUSE ║
║ ─────────────────────────────────────────────────────────────────────── ║
║ Junctional escape 40-60 bpm No P / retrograde P SSS, AV block, ║
║ Narrow QRS vagal, drugs ║
║ Accelerated JR 60-100 Retrograde P or AV Digoxin toxicity, ║
║ dissociation, narrow inferior MI, post-op║
║ Junctional tachy >100 bpm P < V (AV block) Digoxin, post-Sx ║
║ Narrow, gradual onset ║
║ POJET 170-260 V rate > A rate Congenital heart Sx║
║ Congenital JET 150-300 Incessant, narrow Congenital, neonate║
╠══════════════════════════════════════════════════════════════════════════╣
║ TREATMENT ALGORITHM: ║
║ STABLE → Find cause → Treat cause ║
║ UNSTABLE → O2+IV+Monitor → Atropine 0.5mg IV (max 3mg) → ║
║ Dopamine/Epinephrine → Transcutaneous → Transvenous Pacing ║
╠══════════════════════════════════════════════════════════════════════════╣
║ KEY DIFFERENTIALS: ║
║ Narrow QRS slow → Junctional vs. Sinus bradycardia vs. CHB ║
║ Wide QRS slow → Idioventricular vs. Ventricular escape ║
║ Narrow fast → Junctional tachy vs. AVNRT vs. Atrial tachy ║
╠══════════════════════════════════════════════════════════════════════════╣
║ NEVER cardiovert digoxin-induced arrhythmias (→ refractory VF) ║
║ Atropine ineffective for INFRANODAL block → go straight to pacing ║
║ POJET: V rate > A rate (OPPOSITE of complete heart block) ║
║ Inferior MI JR: resolves with reperfusion; pacing rarely needed ║
║ NARROW QRS escape = junctional; WIDE QRS escape = ventricular ║
║ Digoxin: ONLY drug causing ACCELERATED junctional (enhanced auto.) ║
╚══════════════════════════════════════════════════════════════════════════╝
ECG IMAGE REFERENCE GALLERY
REFERENCES
- Tintinalli JE, et al. Tintinalli's Emergency Medicine, 9th ed. Chapter 18, p. 147 (Tables 18-6, 18-7)
- Harrison's Principles of Internal Medicine, 22nd Edition (2025). Chapter 253, p. 1976 (Figure 253-1)
- Marx JA, et al. Rosen's Emergency Medicine, 9th ed. Chapter: Digoxin toxicity
- Harriet Lane Handbook, 23rd ed. Johns Hopkins Hospital. p. 234
- Tanski S, et al. Frameworks for Internal Medicine. Chapter 1
- LITFL ECG Library. Burns E, Buttner R. Accelerated Junctional Rhythm; Junctional Escape Rhythm
- StatPearls - Junctional Rhythm. NCBI Bookshelf NBK507715
- Sasikumar N, et al. "Diagnosis and management of junctional ectopic tachycardia." PMC8457265 (2021)
- Page RL, et al. 2015 ACC/AHA/HRS Guideline for Management of SVT. JACC 2016;67(13):e27-e115
- 2022 ACC/AHA/HRS Guideline on Cardiac Pacing and Cardiac Resynchronization Therapy