Give me detailed study material for pathology practical exam for my prefinal..
Urine-15 Peripheral smear-15 Ospi charts-20 Short case-10 Spotters-20 Viva-20
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Searching the Web
pathology practical exam prefinal MBBS urine analysis peripheral smear OSPI spotters checklist
Reading Web Page
https://www.pathologyoutlines.com/topic/chemistryurinalysis.…
Loading Image
Here is your complete prefinal pathology practical study material covering all six exam components.
PATHOLOGY PRACTICAL EXAM - PREFINAL STUDY MATERIAL
SECTION 1: URINE EXAMINATION (15 Marks)
Step-by-Step Reporting Sequence (follow this order in the exam)
1. Physical Examination
2. Chemical Examination
3. Microscopic Examination
A. Physical Examination
| Parameter | Normal | Abnormal + Significance |
|---|---|---|
| Volume | 1000-1500 mL/24h | Oliguria <400 mL; Anuria <100 mL; Polyuria >2.5 L |
| Color | Pale to deep amber/yellow | See table below |
| Appearance | Clear | Turbid = infection, crystals, pus |
| Smell | Faintly aromatic | Fruity = ketones (DM/starvation); Ammonia = UTI |
| Specific gravity | 1.010-1.025 | Low = DI, renal failure; High = dehydration, DM |
| pH | 4.5-8.0 (avg 6.0) | Alkaline urine = UTI, RTA, vegetarian diet |
| Foam | Minimal white | Persistent frothy = proteinuria (nephrotic syndrome) |
Urine Color Chart - HIGH YIELD
| Color | Cause |
|---|---|
| Red/pink | Hematuria, hemoglobinuria, myoglobinuria, rifampicin, beets |
| Dark yellow/amber | Concentrated urine, urobilinogen excess |
| Dark brown/cola | Acute glomerulonephritis, myoglobinuria |
| Yellow-green | Bilirubin (obstructive jaundice) |
| Milky white | Pyuria (UTI), chyluria (lymphatic obstruction) |
| Black | Alkaptonuria, melanuria |
| Orange | Bile pigments, pyridium |
B. Chemical Examination (Dipstick)
| Parameter | Normal | Positive finding = Suggests |
|---|---|---|
| Protein | Negative (trace <15 mg/dL) | Nephrotic syndrome (3-4+), nephritic syndrome (1-2+), UTI, fever |
| Glucose | Negative | DM (renal threshold exceeded), renal glycosuria (low threshold) |
| Ketones | Negative | DM ketoacidosis, starvation, alcoholism, prolonged vomiting |
| Bilirubin | Negative | Conjugated hyperbilirubinemia (hepatic/obstructive jaundice) |
| Urobilinogen | Trace (0.1-1 EU/dL) | Increased = hemolytic jaundice, hepatic; Absent = obstructive jaundice |
| Blood (Heme) | Negative | Hematuria (RBCs visible), hemoglobinuria (no RBCs), myoglobinuria |
| Leukocyte esterase | Negative | UTI (WBCs in urine) |
| Nitrite | Negative | Gram-negative bacterial UTI (E. coli, Klebsiella) |
| pH | 4.5-8.0 | Alkaline = UTI, RTA; Acid = urate stones, gout |
| Specific gravity | 1.005-1.030 | Fixed SG 1.010 = isosthenuria (renal tubular failure) |
KEY: Bilirubin vs Urobilinogen in jaundice types
| Jaundice | Urine Bilirubin | Urine Urobilinogen |
|---|---|---|
| Prehepatic (hemolytic) | Negative | Very increased |
| Hepatic (hepatocellular) | Positive | Increased |
| Post-hepatic (obstructive) | Strongly positive | Absent/decreased |
C. Microscopic Examination
Preparation: Centrifuge at 1500 rpm x 5 min, decant supernatant, resuspend sediment, examine under 10x (low) and 40x (high power).
RBCs
- Normal: 0-2 RBCs/HPF
- Dysmorphic RBCs (acanthocytes) = glomerular bleeding
- Isomorphic RBCs = lower urinary tract bleeding
-
3 RBCs/HPF = microscopic hematuria
WBCs (Pus cells)
- Normal: 0-4 WBCs/HPF
- Pyuria: >5 WBCs/HPF
- Causes: UTI (most common), pyelonephritis, interstitial nephritis, TB of kidney
Casts - MASTER TABLE (Most important in exam!)
| Cast | Composition | Clinical significance |
|---|---|---|
| Hyaline cast | Tamm-Horsfall mucoprotein | Normal (in concentrated urine, after exercise); minimal significance |
| RBC cast | RBCs in protein matrix | Glomerulonephritis - pathognomonic; nephritic syndrome |
| WBC cast | WBCs in matrix | Pyelonephritis, acute interstitial nephritis |
| Granular cast | Degenerated cell debris | Non-specific: glomerulonephritis, pyelonephritis, ATN |
| Waxy cast | Advanced degeneration | End-stage renal disease, chronic renal failure; "broad casts" = severe |
| Fatty cast | Lipid droplets | Nephrotic syndrome (also oval fat bodies with Maltese cross under polarized light) |
| Epithelial cast | Renal tubular cells | Acute tubular necrosis (ATN) |
| Bacterial cast | Bacteria in matrix | Pyelonephritis |
Memory tip for casts: "Hyaline-RBC-WBC-Granular-Waxy-Fatty-Epithelial" = Helping Renal Work Gets Wider Faster Eventually
Crystals
| Crystal | Appearance | Condition |
|---|---|---|
| Uric acid | Yellow-brown rhomboid/barrel | Gout, uric acid stones (acid urine) |
| Calcium oxalate | "Envelope" or dumbbell shape | Nephrolithiasis, ethylene glycol poisoning |
| Triple phosphate (struvite) | "Coffin lid" shape | UTI with urease-producing bacteria (Proteus) |
| Cystine | Hexagonal plates | Cystinuria (autosomal recessive) |
| Calcium phosphate | Rosette/needle-shaped | Alkaline urine |
| Ammonium biurate | "Thorny apple" | Alkaline urine, old specimen |
| Tyrosine | Fine silky needles in clusters | Severe liver disease |
| Leucine | Yellow-brown oily spheres | Severe liver disease |
URINE EXAM - Disease Pattern Recognition
| Disease | Key Urine Finding |
|---|---|
| Nephrotic syndrome | Heavy proteinuria 3.5g+, fatty casts, oval fat bodies, hyaline casts, lipiduria |
| Nephritic syndrome (AGN) | Hematuria, RBC casts, mild-moderate proteinuria, oliguria |
| Pyelonephritis | WBC casts, WBCs, bacteria, +leukocyte esterase, +nitrite |
| ATN | Epithelial casts, granular casts, renal tubular epithelial cells |
| Chronic renal failure | Waxy/broad casts, isosthenuria (SG fixed ~1.010), proteinuria |
| DM | Glucosuria, proteinuria (early sign of nephropathy), ketonuria |
| Rhabdomyolysis | Myoglobinuria (dipstick positive heme but no RBCs in sediment), myoglobin casts |
| Obstructive jaundice | Bilirubin strongly positive, urobilinogen absent, bile salts positive |
| UTI (uncomplicated) | Pyuria, +leukocyte esterase, +nitrite, bacteria, cloudy urine |
SECTION 2: PERIPHERAL SMEAR (15 Marks)
Step-by-Step Reporting in Exam
- Name the stain used - Leishman/Wright/Giemsa/Romanowsky
- Describe RBCs - size, color, shape, inclusions
- Describe WBCs - perform differential count
- Describe platelets - number, morphology
- Give a provisional diagnosis
A. RBC Morphology - MASTER TABLE
| Abnormal RBC | Description | Key Associations |
|---|---|---|
| Microcyte | Small RBC, MCV <80 fL | IDA, Thalassemia, chronic disease (sometimes) |
| Macrocyte | Large RBC, MCV >100 fL | B12/Folate deficiency, liver disease, MDS |
| Hypochromia | Increased central pallor (>1/3 diameter) | IDA, thalassemia, sideroblastic anemia |
| Spherocyte | Small, dense, no central pallor | Hereditary spherocytosis, AIHA |
| Target cell (codocyte) | Bull's-eye appearance | Thalassemia, HbC disease, liver disease, post-splenectomy |
| Schistocyte (helmet cell) | Fragmented RBC | MAHA (TTP, HUS), DIC, mechanical heart valve |
| Sickle cell (drepanocyte) | Elongated crescent/sickle shape | Sickle cell disease (HbSS) |
| Elliptocyte (ovalocyte) | Oval/elongated RBC | Hereditary elliptocytosis, severe IDA |
| Acanthocyte (spur cell) | Irregular spicules (5-10), uneven spacing | Abetalipoproteinemia, severe liver disease |
| Echinocyte (burr cell) | Regular crenations (10-30), even spacing | Uremia, artifact, liver disease |
| Stomatocyte | Slit-like central pallor ("mouth") | Hereditary stomatocytosis, liver disease, alcohol |
| Teardrop cell (dacrocyte) | Teardrop/pear shape | Myelofibrosis, thalassemia, megaloblastic anemia |
| Rouleaux formation | Stack of coins | Multiple myeloma, inflammation (raised ESR) |
| Agglutination | Irregular clumps | Cold agglutinin disease |
| Pencil cell | Long thin elliptocyte | Iron deficiency anemia |
| Bite cell (degmacyte) | Missing "bite" from RBC | G6PD deficiency (Heinz body removal by spleen) |
Peripheral smear image - Iron Deficiency Anemia (from Robbins Pathology):

Note: Hypochromic microcytic RBCs with enlarged zone of central pallor. Scattered normochromic cells from recent transfusion. - Robbins Pathology
B. Differential Leukocyte Count (DLC) - Normal Values
| Cell | Normal % | Normal Absolute |
|---|---|---|
| Neutrophils | 50-70% | 2000-7500/μL |
| Lymphocytes | 20-40% | 1500-4000/μL |
| Monocytes | 2-8% | 200-800/μL |
| Eosinophils | 1-4% | 40-500/μL |
| Basophils | 0-1% | 0-100/μL |
WBC morphology at a glance:
| Cell | Key Feature | Nucleus | Granules |
|---|---|---|---|
| Neutrophil (seg) | "Lobulated" | 2-5 lobes connected by filaments | Fine pink-purple, inconspicuous |
| Band neutrophil | "Immature" | U-shaped, no filament | Same as neutrophil |
| Lymphocyte (small) | Lymphopenia/lymphocytosis | Round, dark, scant cytoplasm | None (or rare azurophilic) |
| Monocyte | Largest WBC | Kidney/horse-shoe shaped | Fine azurophilic, vacuoles |
| Eosinophil | 2-lobed | Bilobed (figure-of-8) | Large bright orange-red granules |
| Basophil | Rarest; nucleus hidden | Bilobed/irregular, hidden by granules | Large dark-blue/black granules |
C. Peripheral Smear Patterns - Disease Recognition
Iron Deficiency Anemia (IDA)
- Hypochromic microcytic RBCs
- Pencil cells (elongated hypochromic cells)
- Anisocytosis, poikilocytosis
- Target cells (occasionally)
- Platelets: often increased (reactive thrombocytosis)
Megaloblastic Anemia (B12/Folate Deficiency)
- Macro-ovalocytes (large oval RBCs)
- Hypersegmented neutrophils (>5 lobes, or even 1 cell with 6+ lobes = diagnostic)
- Anisocytosis, poikilocytosis
- Pancytopenia (in severe cases)
- Howell-Jolly bodies (sometimes)
Thalassemia
- Hypochromic microcytic (MCV lower than IDA for same Hb level)
- Target cells (prominent)
- Basophilic stippling
- Nucleated RBCs (especially in major form)
- Tear drop cells
Sickle Cell Disease
- Sickle cells (irreversibly sickled)
- Target cells
- Howell-Jolly bodies (functional asplenia)
- Nucleated RBCs
Hereditary Spherocytosis
- Spherocytes (no central pallor)
- Polychromasia (reticulocytes)
- Increased MCHC
- Osmotic fragility test positive
Hemolytic Anemia (general)
- Polychromasia (reticulocytosis - bluish RBCs)
- Nucleated RBCs
- Specific cell types depend on cause
Malaria
- Ring forms (early trophozoites) inside RBCs - Plasmodium falciparum (multiple rings, appliqué/accole forms)
- P. vivax - enlarged RBCs, Schuffner's dots, ameboid trophozoites
- P. malariae - band form (ribbon-shaped) trophozoite
- P. ovale - oval RBCs, Schuffner's dots
Peripheral smear image - Leukocytes including neutrophils (band and segmented):
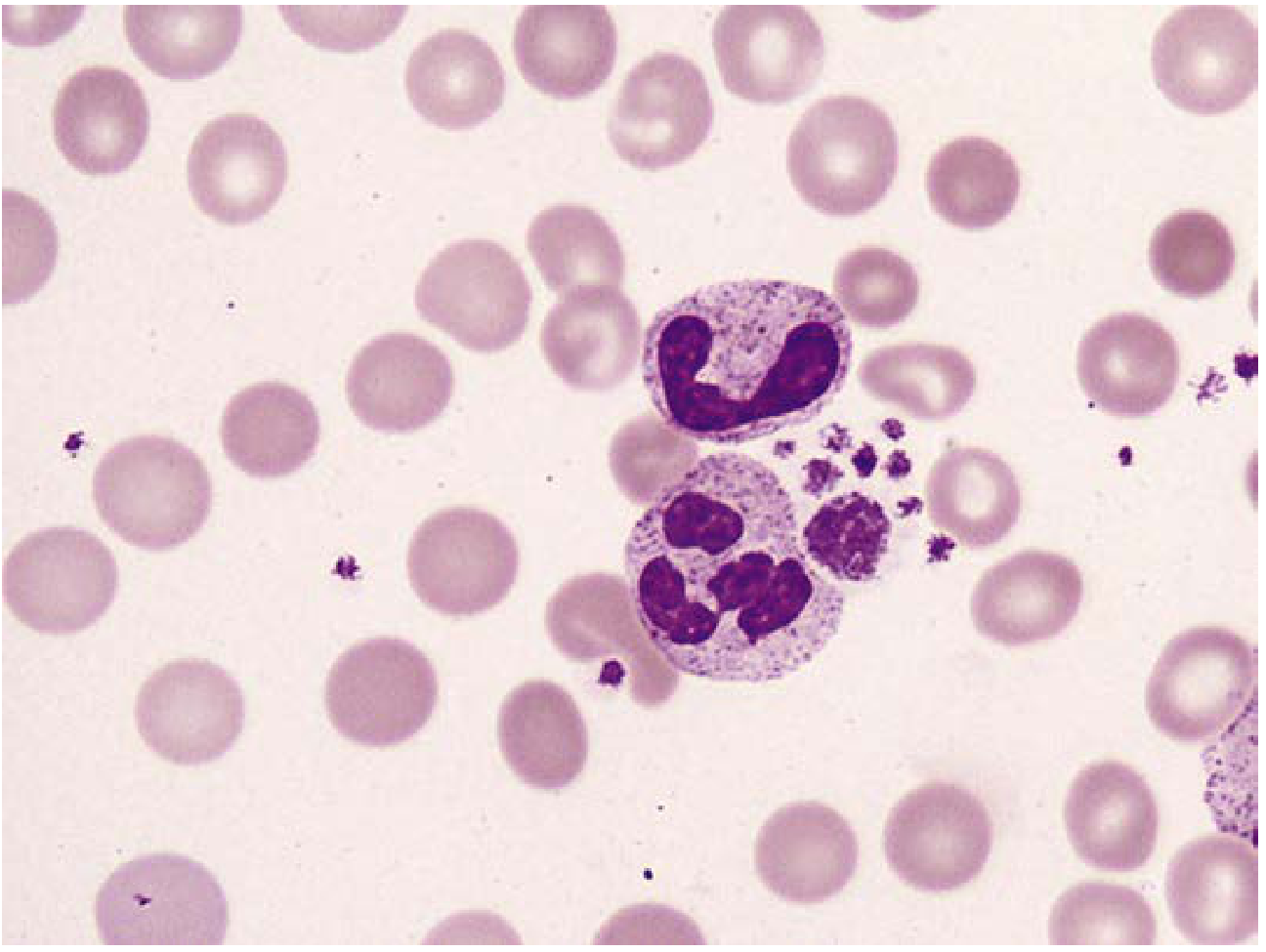
D. WBC Abnormalities
| Finding | Description | Association |
|---|---|---|
| Neutrophilia | >7500/μL | Bacterial infections, stress, steroids, CML |
| Neutropenia | <1500/μL | Viral infections, aplastic anemia, drugs |
| Left shift | Increased band forms, metamyelocytes in blood | Severe bacterial infection, CML |
| Hypersegmentation | Neutrophils >5 lobes | Megaloblastic anemia |
| Toxic granulation | Coarse dark granules in neutrophils | Severe bacterial infection, sepsis |
| Dohle bodies | Pale blue cytoplasmic inclusions (neutrophils) | Infections, burns, pregnancy |
| Auer rods | Pink rod-shaped cytoplasmic inclusions (blasts) | AML (pathognomonic) |
| Lymphocytosis | >4000/μL | Viral infections, CLL, TB, pertussis |
| Atypical lymphocytes | Large, irregular, abundant cytoplasm | EBV (infectious mononucleosis), CMV |
| Blast cells | Large immature cells, prominent nucleoli | Leukemia (AML/ALL) |
| Smudge cells | Disrupted lymphocytes on smear | CLL (pathognomonic) |
SECTION 3: OSPI CHARTS (20 Marks)
OSPI = Objective Structured Practical Interpretation. Charts are usually:
- Hematology value charts / CBC interpretation
- Liver function test (LFT) charts
- Coagulation profile charts
- Renal function / urinalysis interpretation charts
A. CBC Chart Interpretation
Normal CBC Values (MEMORIZE)
| Parameter | Normal Value |
|---|---|
| Hemoglobin (M) | 13.5-17.5 g/dL |
| Hemoglobin (F) | 12.0-15.5 g/dL |
| Hematocrit (M) | 40-52% |
| Hematocrit (F) | 36-48% |
| RBC count | 4.5-6.5 x 10⁶/μL (M); 3.9-5.5 (F) |
| WBC count | 4000-11000/μL |
| Platelets | 1.5-4.5 x 10⁵/μL |
| MCV | 80-100 fL |
| MCH | 27-33 pg |
| MCHC | 32-36 g/dL |
| RDW | <14.5% |
| Reticulocyte count | 0.5-2.5% |
B. Anemia Classification Chart (OSPI Favourite)
By MCV:
| Type | MCV | MCH | MCHC | Common Causes |
|---|---|---|---|---|
| Microcytic hypochromic | <80 fL | Low | Low | IDA, Thalassemia, Sideroblastic anemia, Anemia of chronic disease |
| Normocytic normochromic | 80-100 fL | Normal | Normal | Acute blood loss, hemolytic anemia, aplastic anemia, ACD |
| Macrocytic | >100 fL | High | Normal | B12/Folate def, liver disease, hypothyroidism, MDS, drugs (MTX, hydroxyurea) |
IDA vs Thalassemia Minor - Chart Differentiation
| Feature | IDA | Thalassemia minor |
|---|---|---|
| MCV | Low | Very low (disproportionately low) |
| RBC count | Low | Normal or High |
| RDW | High (>14.5%) | Normal/slightly raised |
| Serum iron | Low | Normal |
| TIBC | High | Normal |
| Ferritin | Low | Normal/high |
| HbA2 (HPLC) | Normal | >3.5% (Beta thal minor) |
| Mentzer Index (MCV/RBC) | >13 = IDA | <13 = Thalassemia |
C. Coagulation Profile Chart
| Test | Normal Value | Prolonged in |
|---|---|---|
| PT (Prothrombin Time) | 12-14 sec | Warfarin, Vit K deficiency, liver disease, DIC, Factor VII deficiency (extrinsic pathway) |
| aPTT (activated PTT) | 25-40 sec | Heparin, hemophilia A/B, DIC, lupus anticoagulant (intrinsic pathway) |
| TT (Thrombin Time) | 14-16 sec | Afibrinogenemia, dysfibrinogenemia, heparin excess |
| INR | ~1.0 | Elevated in anticoagulation therapy; target 2-3 for DVT treatment |
| Fibrinogen | 200-400 mg/dL | Low in DIC, liver disease, thrombolytic therapy |
| D-dimer | <0.5 μg/mL | Elevated in DIC, PE, DVT, sepsis |
| Bleeding time (BT) | 1-9 min (Ivy) | Platelet disorders, VWD, aspirin use |
| Clotting time (CT) | 5-11 min | Heparin, coagulation factor deficiencies |
DIC Chart Recognition:
| Parameter | DIC |
|---|---|
| PT | Prolonged |
| aPTT | Prolonged |
| Platelets | Decreased |
| Fibrinogen | Decreased |
| D-dimer | Increased |
| Peripheral smear | Schistocytes |
D. LFT Chart Interpretation
| Parameter | Hepatocellular | Cholestatic/Obstructive |
|---|---|---|
| AST/ALT | Very high (100-1000s) | Mild elevation |
| ALP | Mild elevation | Very high |
| GGT | High | Very high |
| Bilirubin | Mostly unconjugated (early) / mixed | Mostly conjugated |
| Albumin | Low in chronic | Normal early |
| PT | Prolonged | May be prolonged |
| Urine bilirubin | Positive | Strongly positive |
| Urine urobilinogen | Increased | Absent |
SECTION 4: SHORT CASE (10 Marks)
In a short case, you will be given a clinical scenario + lab reports and asked to:
- Identify the diagnosis
- Justify with lab findings
- Suggest additional investigations
- Outline management
Classic Short Cases and Their Approach
Case 1: Anemia workup
- Clinical: Fatigue, pallor, pica (clay eating)
- Lab: Hb 7 g/dL, MCV 68, MCH 20, MCHC 28, RDW 18%, Serum ferritin 4 ng/mL
- Peripheral smear: Hypochromic microcytic RBCs, pencil cells
- Diagnosis: Iron Deficiency Anemia
- Additional: Serum iron, TIBC, transferrin saturation; find the cause (GI bleed, menorrhagia)
- Management: Oral ferrous sulfate 200 mg TID x 3-6 months; treat underlying cause
Case 2: Megaloblastic Anemia
- Clinical: Elderly vegetarian, weakness, sore tongue, subacute combined degeneration signs
- Lab: Hb 8 g/dL, MCV 115, pancytopenia, hypersegmented neutrophils, macro-ovalocytes
- Diagnosis: Megaloblastic anemia (B12 deficiency)
- Additional: Serum B12, folate, homocysteine, methylmalonic acid
- Management: B12 IM injections (cyanocobalamin 1000 μg); address dietary cause
Case 3: Nephrotic Syndrome
- Clinical: Puffiness of face, pedal edema, frothy urine
- Lab: Albumin 2.0 g/dL, proteinuria 4+, cholesterol high
- Urine: Fatty casts, oval fat bodies, heavy proteinuria >3.5 g/day
- Diagnosis: Nephrotic Syndrome
- Management: Treat cause (steroids for MCD); diuretics; ACE inhibitors
Case 4: DIC
- Clinical: Post-obstetric complication, sepsis, or malignancy; bleeding from multiple sites
- Lab: Low platelets, prolonged PT/aPTT, low fibrinogen, high D-dimer, schistocytes on smear
- Diagnosis: Disseminated Intravascular Coagulation
- Management: Treat underlying cause; FFP, platelet transfusion, cryoprecipitate
Case 5: CML (Chronic Myeloid Leukemia)
- Clinical: Splenomegaly, fatigue, weight loss
- Lab: WBC very high (50,000-500,000/μL), all stages of granulocyte maturation on smear ("left shift continuum"), eosinophilia + basophilia
- Diagnosis: Chronic Myeloid Leukemia
- Confirm: BCR-ABL fusion gene (Philadelphia chromosome)
- Management: Imatinib (STI-571)
SECTION 5: SPOTTERS (20 Marks)
Spotters are typically gross specimens, histology slides, or instruments. Common categories:
A. Gross Specimens - Common Spotters
| Specimen | Key Features to Identify | Diagnosis |
|---|---|---|
| Liver - nutmeg liver | Brown-yellow mottled appearance ("nutmeg"), alternating congestion and fatty change | Chronic passive congestion (Right heart failure) |
| Lung - red hepatization | Solid, heavy, dark red, liver-like consistency | Lobar pneumonia (Day 2-4) |
| Lung - grey hepatization | Solid, grey, dry cut surface | Lobar pneumonia (Day 4-8) |
| Kidney - contracted granular | Small, shrunken, granular surface | Chronic glomerulonephritis / hypertensive nephropathy |
| Kidney - large white | Enlarged, pale, smooth | Nephrotic syndrome (amyloidosis / membranous nephropathy) |
| Brain - cerebral softening | Pale/yellow soft area | Infarction |
| Heart - vegetations on mitral | Warty/irregular masses on valve leaflets | Infective endocarditis (large, irregular) or Rheumatic fever (small, along line of closure) |
| Spleen - lardaceous | Enlarged, pale, waxy, firm | Amyloidosis |
| Appendix - acute appendicitis | Congested, hyperemic, fibrin-covered serosa | Acute appendicitis |
B. Histology Slides - Common Spotters
| Slide/Lesion | Key Microscopic Features |
|---|---|
| Acute inflammation | Vascular dilation, neutrophil infiltration, edema |
| Chronic inflammation | Lymphocytes, plasma cells, macrophages, fibrosis, giant cells |
| Granuloma (tuberculosis) | Epithelioid cells, Langerhans giant cells, central caseous necrosis, lymphocytic cuff |
| Caseous necrosis | Amorphous pink material with ghost outlines (vs coagulative = ghost outline visible; vs liquefactive = none) |
| Amyloidosis | Homogeneous pink amorphous deposits; Congo red stain = apple-green birefringence under polarized light |
| Carcinoma in-situ (CIS) | Full-thickness epithelial dysplasia, no basement membrane breach |
| Invasive carcinoma | Malignant cells breaching basement membrane, desmoplastic stroma |
| Adenocarcinoma | Glandular formation by malignant cells |
| Squamous cell carcinoma | Keratin pearls, intercellular bridges |
| Reed-Sternberg cells | Large binucleate cell, "owl-eye" nucleoli - Hodgkin lymphoma |
| Psammoma bodies | Laminated calcified concentric spheres - papillary thyroid carcinoma, meningioma, serous cystadenocarcinoma |
| Foam cells | Lipid-laden macrophages - atherosclerotic plaque (fatty streak) |
| Hyaline membrane | Eosinophilic membrane lining alveoli - ARDS, RDS of newborn |
C. Instruments/Procedures - Spotters
| Instrument | Use |
|---|---|
| Disposable syringe | Blood collection |
| EDTA tube (lavender/purple top) | CBC, blood smear |
| Citrate tube (blue top) | Coagulation studies (PT, aPTT) |
| SST/Serum tube (red/gold) | Serum biochemistry, LFTs |
| Fluoride-oxalate tube (grey) | Blood glucose (inhibits glycolysis) |
| Urine dipstick | Urinalysis |
| Centrifuge | Urine sediment, blood component separation |
| Bone marrow biopsy needle (Jamshidi) | Bone marrow biopsy |
| Turk's fluid | WBC counting (dilutes and lyses RBCs) |
| Hayem's fluid | RBC counting (dilutes RBCs) |
SECTION 6: VIVA (20 Marks)
High-frequency viva questions and model answers:
Q1. What is the difference between RBC cast and WBC cast? What is the clinical significance of each?
- RBC cast: Red cells within a Tamm-Horsfall protein matrix. Pathognomonic of glomerulonephritis. Indicates glomerular damage with bleeding into the tubule.
- WBC cast: White cells in a protein matrix. Indicates pyelonephritis or acute interstitial nephritis - infection/inflammation within the renal parenchyma.
Q2. How do you differentiate IDA from Thalassemia minor on CBC?
- Use Mentzer Index: MCV/RBC. >13 = IDA; <13 = Thalassemia
- In IDA: RDW high, serum ferritin low, TIBC high
- In thalassemia minor: RBC count normal or high, HbA2 >3.5%, ferritin normal
Q3. What are the causes of macrocytic anemia?
- Megaloblastic: B12 deficiency, folate deficiency
- Non-megaloblastic: Liver disease, hypothyroidism, aplastic anemia, MDS, reticulocytosis, drugs (hydroxyurea, methotrexate, zidovudine, alcohol)
Q4. What is the significance of hypersegmented neutrophil?
- Defined as neutrophil with 5 or more lobes, OR any cell with 6+ lobes
- Pathognomonic of megaloblastic anemia (B12/Folate deficiency)
- Also seen in uremia, iron overload, myelodysplastic syndrome
Q5. What is DIC? How do you diagnose it on lab?
- DIC = Disseminated Intravascular Coagulation - widespread activation of the coagulation cascade consuming clotting factors and platelets, paradoxically causing both thrombosis and bleeding
- Lab: Low platelets, prolonged PT + aPTT, low fibrinogen, elevated D-dimer, elevated FDPs, schistocytes on peripheral smear
Q6. What is the Congo Red stain used for? What does it show under polarized light?
- Used to identify amyloid deposits in tissues
- Under normal light: pink-red staining of amyloid
- Under polarized light: apple-green birefringence - pathognomonic of amyloid
Q7. Name 5 causes of splenomegaly and how pathology differentiates them.
- Infections (malaria, kala-azar, EBV)
- Hemolytic anemias (HS, thalassemia)
- Congestion (portal hypertension)
- Infiltrations (amyloidosis, Gaucher disease)
- Neoplasms (CML, lymphoma)
Q8. Differentiate between exudate and transudate.
| Feature | Exudate | Transudate |
|---|---|---|
| Protein | >3 g/dL | <3 g/dL |
| Specific gravity | >1.020 | <1.015 |
| LDH | High | Low |
| Cells | Many (neutrophils, lymphocytes) | Few |
| Cause | Inflammation, infection, malignancy | Heart failure, cirrhosis, hypoproteinemia |
Q9. What is a Schiller-Duval body?
- Seen in yolk sac tumor (endodermal sinus tumor)
- Looks like a glomerulus: central vessel surrounded by tumor cells in a cystic space
Q10. What are the special stains and what they identify?
| Stain | Identifies |
|---|---|
| PAS (Periodic Acid-Schiff) | Glycogen, mucin, fungal cell walls |
| Congo red | Amyloid (apple-green birefringence) |
| Ziehl-Neelsen (ZN) | Acid-fast bacilli (Mycobacterium TB) |
| Prussian blue (Perl's) | Hemosiderin/iron deposits |
| Oil red O | Lipids/fat (requires fresh frozen sections) |
| Reticulin (Silver) | Reticular fibers (hepatic architecture, myelofibrosis) |
| Masson's trichrome | Collagen (blue/green), muscle (red) |
| Mucicarmine | Mucin (cryptococcus capsule) |
| Toluidine blue | Mast cells (metachromatic) |
| Alcian blue | Acid mucopolysaccharides |
Q11. What is the difference between necrosis and apoptosis?
| Feature | Necrosis | Apoptosis |
|---|---|---|
| Type | Pathological | Physiological/Pathological |
| Cells affected | Groups of cells | Single cells |
| Membrane | Disrupted | Intact |
| Inflammation | Yes (prominent) | No |
| ATP required | No | Yes |
| DNA | Random fragments | Ladder pattern (180 bp multiples) |
| Phagocytosis | Neutrophils first | Macrophages |
EXAM DAY TIPS
- Urine exam: Always report in the sequence - Physical → Chemical → Microscopic. State "normal" for each if negative.
- Peripheral smear: Identify the predominant RBC abnormality first, then name it, then give 2-3 causes.
- OSPI charts: Read all values before giving a diagnosis. Compare values with normals.
- Short case: Use a systematic approach - history clue → lab → diagnosis → management.
- Spotters: State the specimen type, organ, gross appearance, then give the diagnosis with one key feature justification.
- Viva: Speak confidently. If unsure, mention what you know and what you would investigate.
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods; Robbins & Cotran Pathologic Basis of Disease; ROSEN's Emergency Medicine; Tietz Textbook of Laboratory Medicine; Pathology Outlines - Urinalysis
This is a shared conversation. Sign in to Orris to start your own chat.