Cryphorchidism reproductive system phisiology long question
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full long-answer response.
Cryptorchidism: Reproductive System Physiology - Long Answer
Definition
Cryptorchidism (Greek: kryptos = hidden, orchis = testis) is the failure of one or both testes to descend from the abdominal cavity into the scrotal sac. It is the most common congenital anomaly of the male genitalia and a significant cause of male infertility and testicular malignancy.
Embryology and Normal Testicular Descent
Origin of the Testis
- At ~32 days postovulation, gonads arise as thickenings on the medial aspect of the urogenital ridge (posterior abdominal wall)
- The SRY gene (sex-determining region, Y chromosome) triggers testicular differentiation - it activates SOX9, which drives Sertoli cell specification
- By 6-8 weeks, primordial germ cells (PGCs) migrate from the yolk sac and localize within forming testicular cords
- Leydig cells appear in the interstitium by weeks 8-10 and begin testosterone secretion under hCG stimulation
Two Phases of Testicular Descent
(Robbins, Cotran & Kumar Pathologic Basis of Disease)
Phase 1 - Transabdominal Phase (weeks 10-15):
- The testes migrate from the posterior abdominal wall to the lower abdomen/pelvic brim
- Controlled by Müllerian-inhibiting substance (MIS)/Anti-Müllerian Hormone (AMH) secreted by Sertoli cells
- The gubernaculum (a fibromuscular band) swells and anchors the testis to the inguinal region, while the cranial suspensory ligament regresses
- INSL3 (insulin-like factor 3, produced by Leydig cells) acting via its receptor RXFP2/LGRF8 is critical for gubernacular swelling and anchoring in this phase
Phase 2 - Inguinoscrotal Phase (weeks 25-35, third trimester):
- The testis passes through the inguinal canal into the scrotum
- This phase is androgen-dependent - testosterone (converted to DHT) acts via the androgen receptor
- Androgens are required to induce regression of the cranial suspensory ligament and drive gubernacular elongation/migration
- The genitofemoral nerve (GFN) provides essential innervation to the gubernaculum; calcitonin gene-related peptide (CGRP) released from GFN is the downstream mediator
- Complete descent into the scrotum is not achieved until the third trimester
Key hormonal regulators: INSL3 (Phase 1) + Androgens/DHT (Phase 2)
(Campbell Walsh Wein Urology)
Epidemiology
| Parameter | Data |
|---|---|
| Premature infants | ~30% affected at birth |
| Full-term infants | 3-5% at birth; ~1% by 1 year of age |
| Unilateral vs bilateral | Unilateral ~2x more common than bilateral |
| Bilateral accounts for | ~25% of cases |
| Spontaneous descent | Most inguinal UDT descend by end of Year 1 |
(The Developing Human; Robbins & Kumar)
Classification
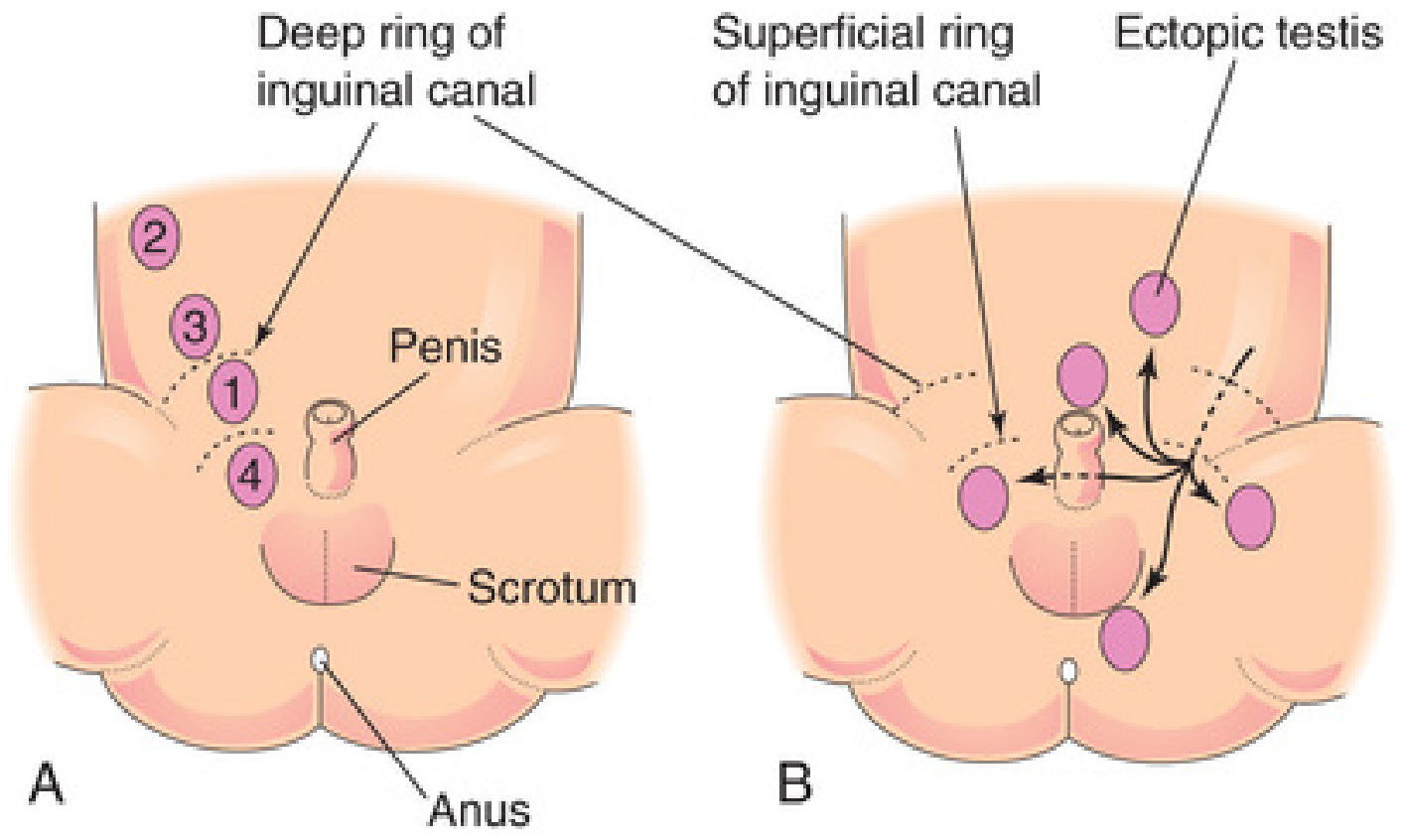
1. Undescended Testis (True Cryptorchidism)
- Testis arrested along its normal path of descent
- Locations in order of frequency (see figure below):
- Inguinal canal (most common, ~70%)
- Just inside the deep inguinal ring
- Just outside the superficial inguinal ring
- High scrotal
2. Ectopic Testis
- Testis has deviated from the normal path of descent after exiting the inguinal canal
- Sites: superficial inguinal pouch (most common), perineum, root of penis (pubic type), femoral triangle
- Due to rupture/dominance of an accessory tail of the gubernaculum (Lockwood's five tails: scrotal, pubic, perineal, inguinal, femoral)
- An ectopic testis is usually well-developed (unlike an undescended testis, which is small and atrophied)
3. Retractile Testis
- A normally descended testis that retracts into the inguinal canal due to hyperactive cremasteric reflex
- Can be manually brought into the scrotum - does NOT require surgery
Pathophysiology and Consequences
Why the Scrotum Matters - Thermoregulation
Normal spermatogenesis requires a temperature 2-4°C below core body temperature (33-35°C). The scrotum achieves this via:
- Pampiniform plexus (countercurrent heat exchange)
- Cremaster muscle (temperature-regulated elevation/lowering)
- Dartos muscle and thin scrotal skin
In cryptorchidism, the retained testis is exposed to normal abdominal temperature (~37°C), which is toxic to the germinal epithelium (spermatogonia are heat-sensitive) while Leydig cells are relatively spared.
Histological Changes (Robbins, Cotran & Kumar)
| Timeline | Histological Change |
|---|---|
| At birth | Usually normal |
| By 2 years | Basement membrane thickening of seminiferous tubules |
| Progressive | Loss of spermatogonia; tubules contain only Sertoli cells |
| Late stage | Hyalinized tubular cords; increased interstitial stroma |
| Any stage | Germ cell neoplasia in situ (GCNIS) may appear |
| Throughout | Leydig cells are SPARED → testosterone production relatively preserved |
Notably, similar histologic changes may appear in the contralateral normally descended testis in unilateral cryptorchidism - suggesting an underlying intrinsic gonadal developmental defect (testicular dysgenesis syndrome) rather than purely positional damage.
Etiology and Risk Factors
Hormonal causes:
- Deficiency of fetal testosterone or DHT production
- Deficiency of INSL3 or RXFP2 mutations
- Deficiency of AMH/MIS
Genetic/syndromic associations:
- Prader-Willi syndrome
- Noonan syndrome
- Androgen insensitivity syndromes
- HOX gene mutations
Environmental factors:
- Endocrine disruptors (estrogen-like compounds in the intrauterine environment)
- Twin studies suggest both maternal inheritance and intrauterine environment play roles
Most cases: etiology unknown (cryptorchidism is rarely associated with a well-defined hormonal disorder in clinical practice)
Clinical Features
- Asymptomatic - usually discovered by parent or physician noting an empty scrotum
- Unilateral > bilateral
- The undescended testis is smaller and less developed than the contralateral testis
Complications:
| Complication | Details |
|---|---|
| Infertility/subfertility | Due to impaired spermatogenesis (Sertoli cell dysfunction, heat damage) |
| Testicular malignancy | 4-10 fold increased risk (most common: seminoma) |
| Testicular torsion | Undescended testis frequently undergoes torsion - mimics strangulated hernia |
| Inguinal hernia | 10-20% of cryptorchid patients (patent processus vaginalis) |
| Psychological | Empty scrotum in older children |
Reproductive Prognosis
(Campbell Walsh Wein Urology)
| Condition | Paternity Rate | Inhibin B | Sperm Density |
|---|---|---|---|
| Normal controls | ~96% | Normal | Normal |
| Unilateral cryptorchidism (treated) | ~96% | ~2/3 of normal | Reduced |
| Bilateral cryptorchidism (treated) | ~70% | ~1/3 of normal | Markedly reduced |
- Fertility impairment in cryptorchidism is primarily due to Sertoli cell/seminiferous epithelium dysfunction (reflected by low inhibin B), rather than Leydig cell dysfunction (testosterone levels less severely affected)
- Bilateral cryptorchidism carries a significantly worse prognosis for fertility than unilateral
Diagnosis
Physical examination - primary tool:
- Examine in warm room; supine and frog-leg position; palpate inguinal canal and scrotum
- Palpable vs non-palpable testis guides management
Investigations:
- Ultrasound - for inguinal testes
- MRI - for suspected intra-abdominal testis
- Laparoscopy - gold standard for non-palpable testis (diagnostic and therapeutic)
- Hormonal stimulation test (hCG stimulation): rise in testosterone confirms functional testicular tissue; no response suggests absent testes (anorchia)
- FSH, LH, inhibin B - markers of Sertoli cell and spermatogenesis status
Treatment
Medical (Hormonal)
- hCG injections (human chorionic gonadotropin) - stimulates Leydig cells to produce testosterone, promoting descent
- GnRH (buserelin) intranasal - less commonly used
- Success rate is modest (~20-30%); not recommended as primary treatment by modern guidelines
Surgical - Orchidopexy (Definitive Treatment)
- Timing: Current recommendation = 6 to 12 months of age (before histologic changes become established)
- Sabiston: orchidopexy at 6-12 months for palpable inguinal testis
- Robbins: "hormone injections followed by early orchiopexy at 6-12 months if medical treatment fails"
Procedure:
- Standard dartos pouch orchidopexy - for palpable inguinal testis; testis brought down and fixed in a sub-dartos pouch in the scrotum
- Two-stage Fowler-Stephens orchidopexy - for high intraabdominal testis with short vessels:
- Stage 1: Ligation of testicular vessels (to allow collateral circulation to develop over 6 months)
- Stage 2: Orchidopexy via collateral blood supply
- Laparoscopic orchidopexy - increasingly preferred single-stage option for intra-abdominal testis
Outcomes of Orchidopexy
- Reduces (but does not eliminate) risk of malignancy
- Reduces risk of torsion
- Improves fertility outcomes if performed early
- Deficient spermatogenesis still reported in 10-60% even after orchidopexy
- Cancer risk remains elevated even after repositioning (linked to intrinsic testicular dysgenesis)
Relationship to Testicular Cancer
- Cryptorchidism is the most important risk factor for testicular germ cell tumors
- Risk is highest with abdominal cryptorchidism (>intra-canalicular)
- Mechanism: Germ cell neoplasia in situ (GCNIS) - malignant transformation of arrested spermatogonia/gonocytes
- The contralateral descended testis is also at higher risk for malignancy - supporting the testicular dysgenesis theory
- Most common tumor arising: seminoma
- Orchidopexy does NOT eliminate the cancer risk but does allow regular physical examination and earlier detection
Summary Table
| Feature | Key Point |
|---|---|
| Definition | Failure of testis to descend into scrotum |
| Incidence | 3-5% at birth; 1% at 1 year |
| Phase 1 hormone | INSL3 + AMH (transabdominal) |
| Phase 2 hormone | Androgens/DHT (inguinoscrotal) |
| Most common site | Inguinal canal |
| Pathology | Spermatogonia lost; Leydig cells spared |
| Complications | Infertility, malignancy, torsion, hernia |
| Treatment timing | Orchidopexy at 6-12 months |
| Cancer risk | 4-10x increased risk |
| Fertility (bilateral) | ~70% paternity rate after treatment |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease | Robbins & Kumar Basic Pathology | Campbell Walsh Wein Urology | The Developing Human: Clinically Oriented Embryology (Moore & Persaud) | Sabiston Textbook of Surgery | S Das Manual on Clinical Surgery
This is a shared conversation. Sign in to Orris to start your own chat.