Difference between hydromyelia and syrindomyelia with mri images
Reading File
Finding Sources
Searching the Web
hydromyelia vs syringomyelia MRI differences imaging
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Searching the Web
hydromyelia MRI central canal dilatation vs syringomyelia parenchymal cavity axial image
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Hydromyelia vs. Syringomyelia
Definitions and Core Distinction
Both conditions involve fluid-filled cavities within the spinal cord, but they differ fundamentally in their anatomical location and lining:
| Feature | Hydromyelia | Syringomyelia |
|---|---|---|
| Definition | Dilatation of the central canal of the spinal cord | Cystic cavity within the cord parenchyma itself |
| Cavity lining | Lined by ependymal cells (ependyma-lined) | NOT lined by ependyma; surrounded by glial tissue |
| Location | Strictly within the central canal | Adjacent to/outside the central canal, in white/grey matter |
| Communication | Communicates with ventricular system/4th ventricle | May or may not communicate with central canal |
| Fluid content | CSF identical to ventricular CSF | CSF-like fluid; may differ slightly |
| Cause | Obstruction/increased CSF pressure, often hydrocephalus | Chiari I malformation, trauma, tumors, arachnoiditis |
| Progression | Often non-progressive ("slit-like," incidental) | Tends to expand and propagate via hydrodynamic forces |
| Clinical significance | Often benign, may be asymptomatic | Progressive neurological deficits |
Pathology
From Robbins & Cotran:
"These disorders are characterized by expansion of the ependymal-lined central canal of the cord (hydromyelia) or by the formation of a fluid-filled cleft-like cavity in the inner portion of the cord (syringomyelia, syrinx) that may extend into the brainstem (syringobulbia)."
From Adams & Victor's Neurology (12th ed.):
- Pure hydromyelia = Type IV in classification: developmental dilatation of the central canal, with or without hydrocephalus - non-progressive
- Syringomyelia = cavitation of central cord, usually cervical, characterized by dissociated sensory loss (loss of pain/temperature with preserved light touch/vibration/position sense) due to disruption of crossing anterior commissural fibers
When both processes coexist (which is common), the combined term syringohydromyelia or hydrosyringomyelia is used. As the syringomyelic cavity expands, it can compress and obliterate the hydromyelic component, and the connection between the two can be lost.
Classification of Syringomyelia (Adams & Victor)
- Type I - With obstruction at foramen magnum + central canal dilatation (developmental): associated with Chiari I malformation or bony foramen magnum anomalies
- Type II - Without foramen magnum obstruction (idiopathic developmental)
- Type III - With other spinal cord diseases (acquired): spinal tumors, traumatic myelopathy, arachnoiditis, cord compression
- Type IV - Pure hydromyelia (developmental), with or without hydrocephalus
MRI Features
Signal Characteristics (both conditions)
- T1-weighted: hypointense (dark) - matches CSF signal
- T2-weighted: hyperintense (bright) - matches CSF signal
- No enhancement on gadolinium contrast (distinguishes from tumor cysts, which may enhance peripherally)
- Flow voids may be seen in ~40% of syringes on T2 (pulsatile CSF movement) - associated especially with Chiari malformations
From Grainger & Allison's Diagnostic Radiology:
"Syringomyelia and its cause are well demonstrated by MRI, which shows a well-circumscribed cavity of a similar signal to CSF on T1 and T2 weighted sequences. Pulsatile cysts may show flow-related signal changes."
Distinguishing on MRI - The Core Problem
The honest answer: hydromyelia and syringomyelia cannot be reliably distinguished on MRI in most cases. The Radiopaedia syrinx article states clearly:
"It is very difficult to distinguish the two on imaging. Hence, the collective terms hydrosyringomyelia or syringohydromyelia can also be used."
However, certain imaging features suggest one over the other:
| MRI Feature | Hydromyelia | Syringomyelia |
|---|---|---|
| Axial location | Central, round/oval, small - in exact midline (central canal position) | Eccentric, larger, may be off-center or multilocular |
| Size | Small, slit-like or narrow tubular | Often larger, may occupy most of cord diameter |
| Cord enlargement | Cord usually normal size | Cord enlarged in ~80% of cases |
| Margins | Smooth, well-defined | Well-defined but may be irregular |
| Flow voids on T2 | Rare | More common (40%), especially with Chiari |
| Associated findings | Hydrocephalus, myelomeningocele | Chiari malformation, tumor at poles, arachnoiditis |
| Extent | Usually shorter, may be limited | Often long-segment, multi-level |
MRI Images
Figure 1 - Syringomyelia with Chiari malformation (sagittal and brainstem extension)
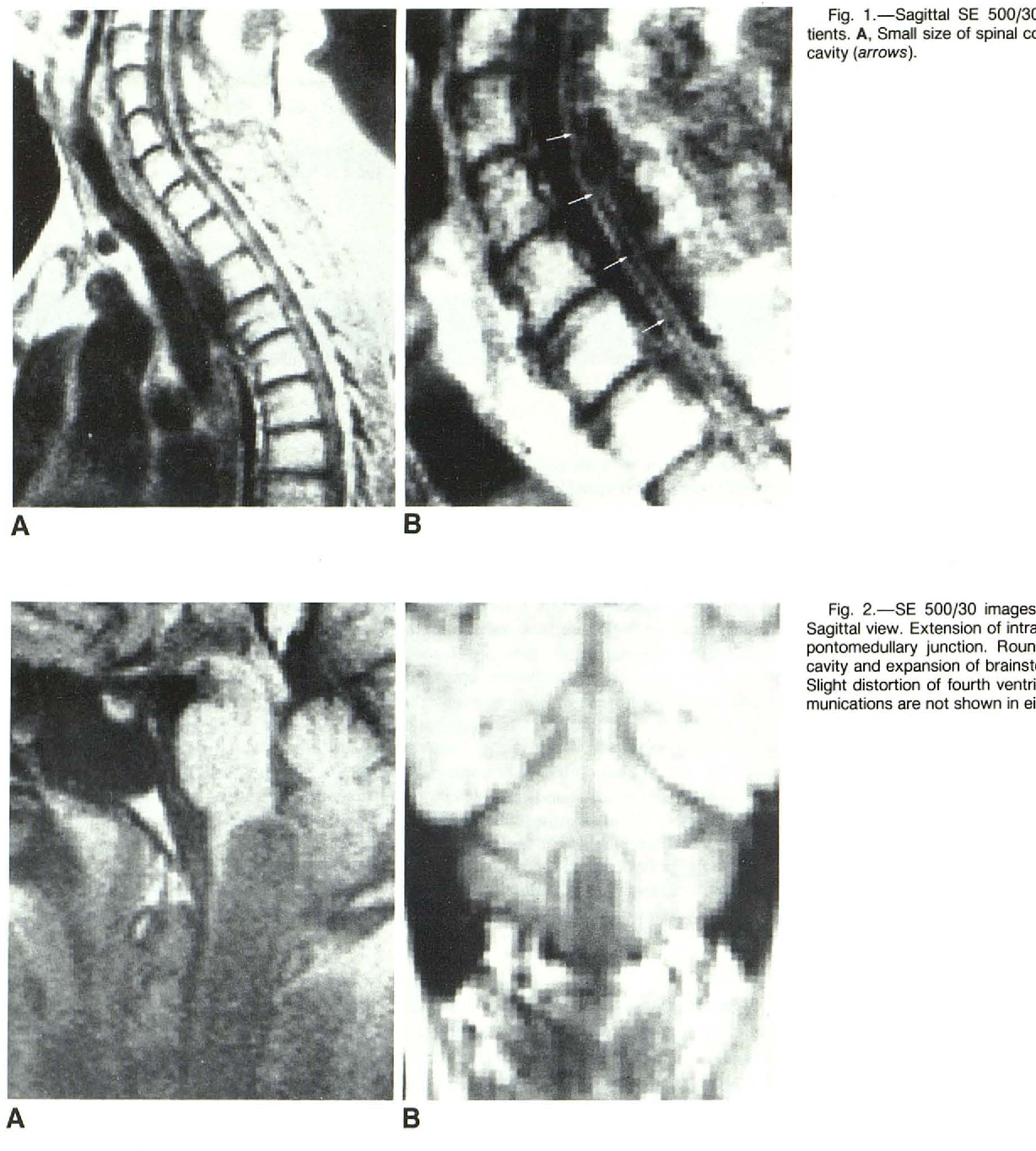
Fig. A (top-left): Sagittal T2 MRI - small syrinx cavity (arrows) in the cervical cord. Fig. B (top-right): Close-up of central cord cavity. Bottom row: Extension into pontomedullary junction (syringobulbia).
Figure 2 - Syringomyelia with Chiari I malformation: cervical to thoracic extent
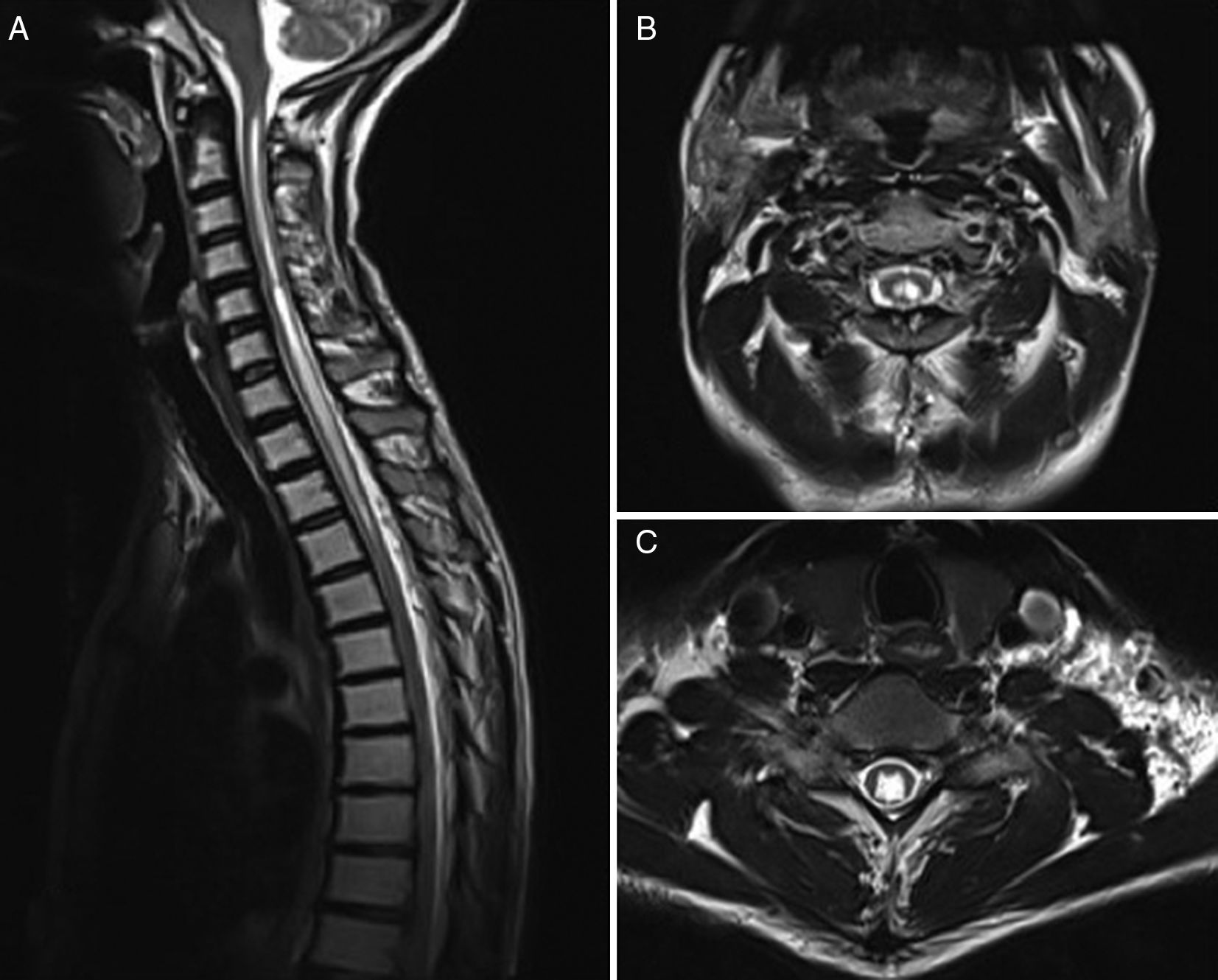
A: Sagittal T2 - large hyperintense fluid cavity (syrinx) running cervicothoracic cord with Chiari I (cerebellar tonsil herniation). B: Axial T2 - round central hyperintense cavity at cervical level. C: Axial T2 at lower level - smaller residual cavity.
Figure 3 - Comparison of different syrinx types (from JCM 2023)

A: Cervical syrinx with Chiari I (upper arrow = tonsillar herniation, lower arrow = syrinx). B: Long-segment thoracic post-traumatic syrinx (multiple arrows). C: Isolated cervical syrinx with Chiari (arrow at foramen magnum).
Clinical Presentation
Both can present with:
- Dissociated sensory loss (cape-like distribution: loss of pain & temperature in upper limbs, preserved vibration/position) - classic for syrinx disrupting anterior commissure
- Painless muscle wasting/weakness in the hands and arms (brachial amyotrophy)
- Horner syndrome (involvement of sympathetic fibers)
- Progressive scoliosis
- Spastic paraparesis (if large)
- Syringobulbia signs: nystagmus, dysarthria, dysphagia (extension to medulla)
Hydromyelia specifically: often asymptomatic; when an isolated dilated central canal is found incidentally on MRI with no associated Chiari, tethering, or tumor, it is frequently a benign, non-progressive finding.
Key Take-Home Points
- Hydromyelia = dilated central canal, ependyma-lined, usually benign
- Syringomyelia = parenchymal cavity NOT lined by ependyma, tends to expand, progressive symptoms
- They commonly coexist and the combined term syringohydromyelia is used clinically
- On MRI both appear CSF-isointense (T1 dark, T2 bright) and cannot be reliably differentiated
- MRI focus should be on identifying the underlying cause (Chiari, tumor, arachnoiditis, trauma) rather than trying to distinguish hydro- from syringomyelia
- Treatment targets the underlying etiology (foramen magnum decompression for Chiari, tumor removal, shunting)
Sources: - Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1152 | Adams & Victor's Principles of Neurology, 12th Ed. | Grainger & Allison's Diagnostic Radiology | Radiopaedia - Syrinx | Medscape Imaging Overview
This is a shared conversation. Sign in to Orris to start your own chat.