Basic mode and newer mode of ventilation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Here is a comprehensive overview of basic and newer modes of mechanical ventilation, drawn from multiple authoritative surgical and pulmonary textbooks.
Modes of Mechanical Ventilation
The mode defines the relationship between mandatory, assisted, supported, and spontaneous breath types, plus how inspiratory phase variables are controlled. Every ventilator mode sets four core parameters: (1) breath size (tidal volume or inspiratory pressure), (2) rate, (3) PEEP, and (4) FiO₂. — Sabiston Textbook of Surgery
Basic / Standard Modes
1. Controlled Mechanical Ventilation (CMV)
The ventilator delivers all breaths at a preset rate; the patient cannot trigger the machine. Used in heavily sedated or paralyzed patients. Two subtypes:
- Volume-Controlled Ventilation (VCV): preset tidal volume, airway pressure is variable — used when CO₂ clearance and minute ventilation must be tightly controlled.
- Pressure-Controlled Ventilation (PCV): preset inspiratory pressure, tidal volume is variable — preferred when compliance is very poor and barotrauma risk is high.
In CMV, prolonged use promotes diaphragmatic atrophy and contractility dysfunction.
2. Assist-Control Ventilation (AC)
The most commonly used mode. The ventilator delivers a full breath either when triggered by the patient's effort or, if no effort occurs within a set interval, independently by the machine. Every breath — patient-initiated or machine-initiated — delivers a full preset breath (volume or pressure target).
- AC-VC (Volume Control): tidal volume set at 6–8 mL/kg predicted body weight; plateau pressure must be kept < 30 cm H₂O.
- AC-PC (Pressure Control): inspiratory pressure set; minute ventilation must be closely monitored because changes in compliance alter tidal volume.
AC is associated with low work of breathing since every breath is fully supported. — Current Surgical Therapy 14e; Sabiston Textbook of Surgery
3. Synchronized Intermittent Mandatory Ventilation (SIMV)
A hybrid of AC and pressure support. The ventilator delivers mandatory breaths at a set rate, synchronized with the patient's effort. Spontaneous breaths above the mandatory rate are supported only by the set pressure support level (not full machine breath).
- If sedation is deep or rate set high → functionally equivalent to VC
- If rate set low → functionally equivalent to PSV with occasional "sigh" breaths
- Useful for gradual weaning by reducing mandatory rate over time
Key distinction from AC: in AC, every patient-triggered breath gets full support; in SIMV, spontaneous breaths above the set rate get only partial pressure support. — Sabiston; Current Surgical Therapy 14e
4. Pressure Support Ventilation (PSV)
A purely spontaneous mode — no mandatory breaths. Every breath is patient-triggered and augmented by a preset inspiratory pressure; flow-cycled (breath ends when flow drops to ~25% of peak). Analogous to BiPAP.
- Requires the patient to have a reliable respiratory drive (apnea alarms mandatory)
- Reduces work of breathing
- Primary use: ventilator weaning and liberation
- Can be used stand-alone or embedded within SIMV
5. Continuous Positive Airway Pressure (CPAP)
Spontaneous mode with no mandatory rate. A constant positive pressure maintained throughout the respiratory cycle. The patient controls all breaths; no inspiratory pressure support is added. Used primarily for weaning trials and in non-invasive settings.
Breath Types Within Modes
| Breath Type | Variable Set | Variable Free | Notes |
|---|---|---|---|
| Volume Control (VC) | Tidal volume (6–8 mL/kg PBW) | Airway pressure | Monitor plateau pressure < 30 cmH₂O |
| Pressure Control (PC) | Inspiratory pressure | Tidal volume | Monitor minute ventilation closely |
| Pressure-Regulated Volume Control (PRVC) | Volume target + pressure limit | Dynamic pressure | Software adjusts pressure breath-to-breath to hit volume target |
| Pressure Support (PSV) | Inspiratory pressure | Volume + rate | Flow-cycled; spontaneous only |
PRVC is a newer "dual-control" mode: ventilator software monitors lung compliance each cycle and adjusts inspiratory pressure for the next breath to hit a target tidal volume. When compliance improves, pressure is automatically reduced. — Current Surgical Therapy 14e
The Pressure-Volume Curve and Safe Window
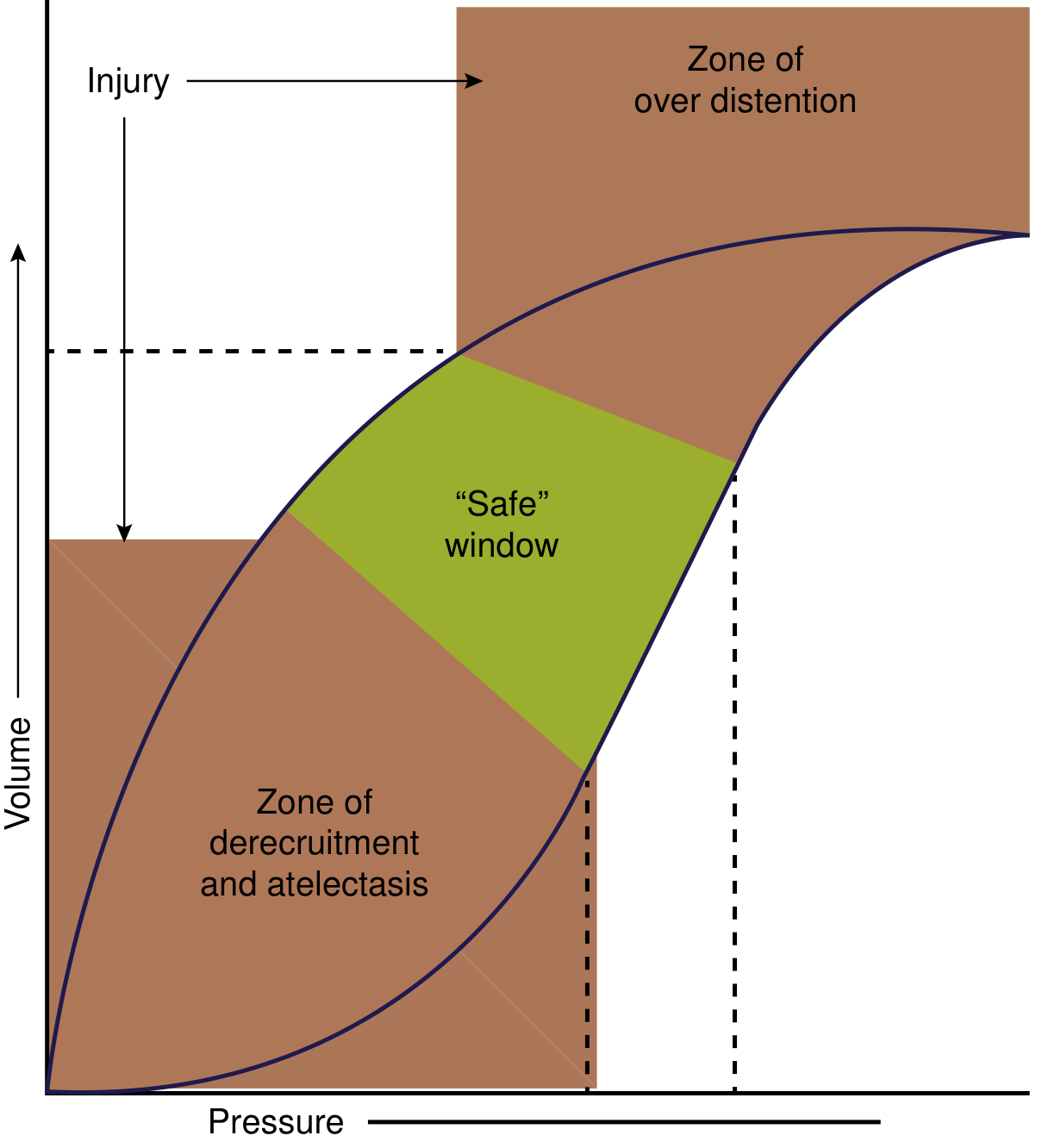
Pressure-volume curve of a diseased lung (e.g., ARDS). Ventilation must stay within the "safe" window: above the lower inflection point (to avoid derecruitment/atelectasis) and below the upper inflection point (to avoid overdistension/barotrauma). — Current Surgical Therapy 14e
Newer / Advanced Modes
6. Airway Pressure Release Ventilation (APRV)
APRV applies two levels of CPAP — a high pressure (P-high) held for a long time (T-high) and a brief "release" to a low pressure (P-low) for a very short time (T-low). Spontaneous breathing is permitted (and encouraged) at both pressure levels.
| Parameter | Typical Setting |
|---|---|
| P-high | 25–30 cm H₂O |
| P-low | 0 cm H₂O |
| T-high | Long (I:E ratio often 7:1 to 10:1) |
| T-low | Very short (~0.4–0.8 s) |
- Tidal volume generated = difference between P-high and P-low
- Achieves high mean airway pressure → improved alveolar recruitment
- Hemodynamically well tolerated with minimal sedation
- Used in severe hypoxemia and ARDS
- A recent meta-analysis (nearly 19 years of data) suggested a mortality benefit in acute hypoxemic respiratory failure vs. conventional modes
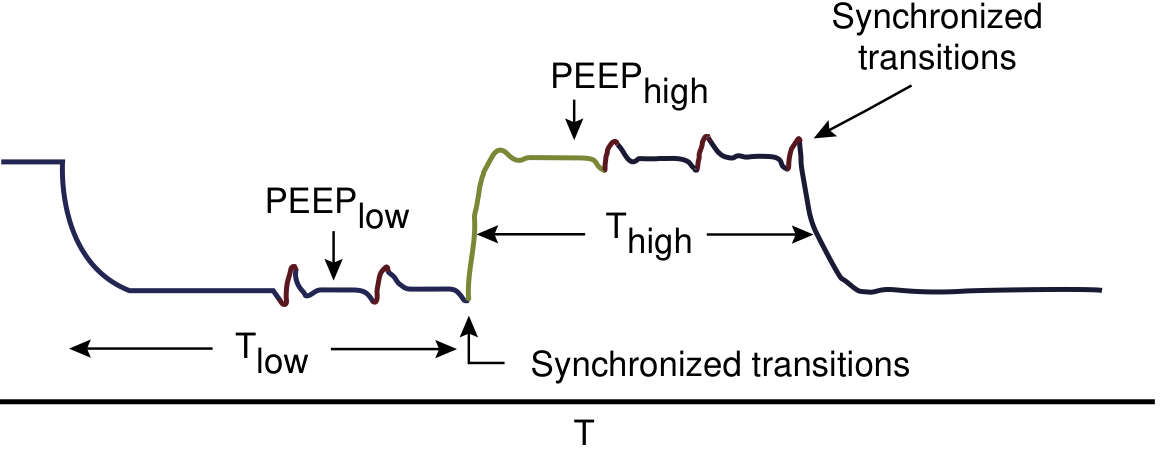
Bilevel/APRV waveform: The ventilator cycles between a high CPAP level (T-high) and a low release pressure (T-low), with spontaneous breaths superimposed at both levels. — Current Surgical Therapy 14e
7. Bilevel Positive Airway Pressure Ventilation (BiLevel / DUOPAP)
Similar to APRV in concept — two PEEP levels with spontaneous breathing allowed at both — but uses a longer T-low (more time at low pressure), resulting in a less extreme I:E ratio than classic APRV. The distinction between APRV and bilevel is mainly in the T-low setting. — Sabiston
8. High-Frequency Oscillatory Ventilation (HFOV)
Delivers extremely small tidal volumes (less than anatomical dead space) at very high frequencies (3–15 Hz / 180–900 breaths/min). Gas exchange occurs via mechanisms beyond bulk flow (asymmetric velocity profiles, molecular diffusion).
- Used as a salvage mode or bridge to ECMO in severe ARDS
- Physiologically appealing for lung protection in ARDS
- Clinical trials (e.g., OSCILLATE, OSCAR) have not shown survival benefit in adults; may even increase mortality in some subgroups
- May have benefit in pediatric ARDS
9. Proportional Assist Ventilation (PAV) / Proportional Pressure Support (PPS)
A newer mode where the ventilator generates pressure in proportion to the patient's own inspiratory effort (both flow and volume). The clinician sets a "gain" rather than a fixed pressure. This maintains patient-ventilator synchrony dynamically and reduces asynchrony. — Fishman's Pulmonary Diseases
Key Concepts: Ventilator-Induced Lung Injury (VILI)
All modes must be set to avoid VILI, caused by:
- Barotrauma — excess airway pressure
- Volutrauma — alveolar overdistension from large tidal volumes
- Atelectrauma — cyclic recruitment/derecruitment
- Biotrauma — inflammatory mediator release from injured lung
Universal protective targets regardless of mode:
- Tidal volume: 6–8 mL/kg predicted body weight
- Plateau pressure: < 30 cm H₂O
- Monitor for auto-PEEP (measured via expiratory hold)
Summary Comparison
| Mode | Mandatory Breaths | Spontaneous Breaths | Primary Use |
|---|---|---|---|
| CMV/VC | Full control, preset | None | Paralyzed/apneic patients |
| AC (VC or PC) | Yes (backup rate) | Full support | Most ICU patients |
| SIMV | Yes (set rate) | Partial (PS only) | Weaning |
| PSV | None | Full support | Weaning, cooperative patients |
| PRVC | Yes (dual control) | — | Better lung protection |
| APRV | Pressure release | Superimposed | ARDS, severe hypoxemia |
| HFOV | Oscillation | None | Refractory ARDS, bridge to ECMO |
| PAV | Proportional | Proportional | Reduce asynchrony |
Sources: Sabiston Textbook of Surgery; Current Surgical Therapy 14e; Fishman's Pulmonary Diseases and Disorders
More information on MV
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Comprehensive content gathered. Here is a full deep-dive on mechanical ventilation:
Mechanical Ventilation — Comprehensive Overview
1. Objectives of Mechanical Ventilation
The goals of MV go beyond simply keeping a patient alive:
| Category | Objectives |
|---|---|
| Gas exchange | Reverse hypoxemia; relieve acute respiratory acidosis |
| Work of breathing | Decrease O₂ cost of breathing; reverse respiratory muscle fatigue |
| Pressure-volume | Prevent/reverse atelectasis; improve lung compliance |
| Lung protection | Prevent further lung injury; permit lung and airway healing |
| Systemic | Allow time to treat the underlying disease; avoid complications |
Increased work of breathing is the most common reason for intubation. It can be clinically assessed by palpating phasic sternomastoid contraction, tracheal tug, suprasternal recession, and intercostal recession — not by any single objective measurement threshold. — Fishman's Pulmonary Diseases
2. Indications for Mechanical Ventilation
Clinical indications:
- Acute hypoxemic respiratory failure (PaO₂/FiO₂ < 200 in ARDS)
- Acute hypercapnic respiratory failure (respiratory acidosis with pH < 7.20–7.25)
- Apnea or impending respiratory arrest
- Airway protection (obtunded, GCS < 8, inability to protect airway from secretions/aspiration)
- Excessive work of breathing that is unsustainable
- Refractory status asthmaticus or status epilepticus
Physiologic thresholds commonly cited (no single cutoff is definitive):
| Parameter | Threshold for Concern |
|---|---|
| Respiratory rate | > 35 breaths/min |
| PaO₂ on high-flow O₂ | < 60 mmHg |
| PaCO₂ (rising acutely) | > 50 mmHg with pH < 7.25 |
| Tidal volume (spontaneous) | < 5 mL/kg |
| Vital capacity | < 15 mL/kg |
| NIF (max inspiratory force) | Less negative than −25 cmH₂O |
3. Initial Ventilator Settings
| Parameter | Typical Initial Setting |
|---|---|
| Mode | AC-VC (most common starting mode) |
| Tidal volume (VT) | 6–8 mL/kg predicted body weight (PBW) |
| Respiratory rate | 12–20 breaths/min (adjusted for pH/PaCO₂) |
| FiO₂ | Start at 1.0, wean rapidly to ≤ 0.6 |
| PEEP | 5 cmH₂O initially; titrate up in ARDS |
| I:E ratio | 1:2 (standard); can invert in ARDS |
| Plateau pressure target | < 30 cmH₂O |
Predicted body weight (not actual) drives VT settings because lung size correlates with height, not weight — critical in obese patients.
4. Ventilator-Induced Lung Injury (VILI)
VILI is the primary hazard of mechanical ventilation itself. Four distinct mechanisms:
| Mechanism | Description |
|---|---|
| Barotrauma | Excess airway pressure ruptures alveoli → pneumothorax, pneumomediastinum, subcutaneous emphysema |
| Volutrauma | Alveolar overdistension from excessive tidal volumes → diffuse alveolar damage |
| Atelectrauma | Cyclic recruitment-derecruitment of unstable alveoli → shear stress injury |
| Biotrauma | Local cytokine release from injured lung → systemic inflammatory response |
The ARMA Trial (ARDS Network): Landmark RCT comparing VT 6 mL/kg vs. 12 mL/kg PBW in ARDS. Mortality 31% vs. 40% — a 9-point absolute reduction with low-tidal-volume ventilation. This is the strongest evidence for lung-protective ventilation. — Harrison's, 22nd Ed.
Key monitoring parameters to prevent VILI:
- Plateau pressure (measured by inspiratory hold): target < 30 cmH₂O
- Driving pressure = Plateau pressure − PEEP: target < 15 cmH₂O (emerging evidence)
- Auto-PEEP (measured by expiratory hold): reflects breath stacking/air trapping
5. PEEP — Titration and Rationale
PEEP prevents alveolar collapse at end-expiration (preventing atelectrauma) and improves oxygenation by:
- Increasing mean airway pressure
- Recruiting collapsed alveoli
- Reducing intrapulmonary shunt
Setting PEEP in ARDS (three approaches):
- ARDS Network FiO₂–PEEP table — empirical combinations of FiO₂ and PEEP levels
- Pressure-volume curve — set PEEP just above the lower inflection point
- Esophageal pressure monitoring — estimates transpulmonary pressure to individualize PEEP; however, a recent phase 2 trial showed no benefit over empirical high PEEP-FiO₂ titration
High PEEP must be balanced against hemodynamic compromise: elevated intrathoracic pressure reduces venous return and cardiac output.
6. MV in ARDS — Special Strategies
| Strategy | Evidence |
|---|---|
| Low VT (6 mL/kg PBW), plateau < 30 cmH₂O | ✅ Mortality benefit (ARMA trial) |
| Prone positioning (≥16 h/day) | ✅ Reduces 28-day mortality 32.8% → 16.0% in severe ARDS (PaO₂/FiO₂ < 150) |
| Neuromuscular blockade (cisatracurium 48h) | ⚠️ Earlier trial showed benefit; subsequent trial showed no mortality benefit — selective use in refractory asynchrony |
| Recruitment maneuvers | ❌ No mortality benefit; may increase mortality when combined with high PEEP |
| HFOV | ❌ No survival benefit in adults (OSCILLATE, OSCAR trials); may increase mortality |
| APRV | Possible mortality benefit in meta-analysis; not standard yet |
| ECMO (VV-ECMO) | ✅ Rescue therapy in severe refractory ARDS; initial use not superior to rescue use — Harrison's |
7. MV in Obstructive Disease (COPD / Asthma)
Key problem: Air trapping and auto-PEEP — incomplete exhalation leads to breath stacking and hyperinflation
Strategies:
- Permissive hypercapnia — accept higher PaCO₂ to allow longer expiratory time
- Low respiratory rate (10–14/min) and long expiratory time (I:E ≥ 1:3 or 1:4)
- Minimize PEEP in asthma (air trapping already generates intrinsic PEEP)
- Extrinsic PEEP set at ~75–85% of measured auto-PEEP in COPD to offset triggering effort
- Deep sedation ± paralysis during most severe phase of asthma
- Non-invasive positive pressure ventilation (NIPPV/BiPAP) is the preferred initial approach in COPD exacerbations — reduces need for intubation and mortality
8. Non-Invasive Ventilation (NIV) vs. Invasive MV
| Feature | NIV (BiPAP/CPAP) | Invasive MV |
|---|---|---|
| Interface | Mask (face, nasal, helmet) | Endotracheal tube |
| Airway protection | None | Full |
| VAP risk | Low | High (~15% incidence) |
| Sedation required | Minimal | Usually required |
| Best indications | COPD exacerbation, cardiogenic pulmonary edema, immunocompromised hypoxemia | Apnea, airway compromise, failure of NIV |
High-Flow Nasal Cannula (HFNC) is an intermediate step: delivers heated/humidified O₂ at 30–60 L/min, provides ~2–5 cmH₂O PEEP, reduces work of breathing. Proven non-inferior to NIV in post-extubation prophylaxis; reduces reintubation vs. conventional O₂ at 48–72h. — Washington Manual
9. Liberation from Mechanical Ventilation (Weaning)
The right approach is active liberation, not slow weaning — excessive caution extends MV time by up to 40%.
Step 1: Daily Readiness Assessment
| Criterion | Target |
|---|---|
| Underlying disease | Improving/resolved |
| Consciousness | Awake, off heavy sedation |
| FiO₂ | ≤ 0.5 |
| PEEP | < 8 cmH₂O |
| SaO₂ | > 88% |
| Hemodynamics | Stable |
| Secretions | Manageable; adequate cough |
Step 2: Weaning Predictor — Rapid Shallow Breathing Index (RSBI)
RSBI = f/VT (respiratory frequency ÷ tidal volume in liters)
- Measured during unaided spontaneous breathing (not with PS or CPAP, which falsely lower it)
- RSBI < 100 → likely to tolerate extubation (high sensitivity ≥ 0.90)
- RSBI > 100 → rapid shallow breathing pattern predicts failure
RSBI is a screening test (high sensitivity), not a confirmatory test. A positive screen should prompt an SBT, not immediate extubation. — Fishman's Pulmonary Diseases
Step 3: Spontaneous Breathing Trial (SBT)
A 30–120 minute trial of minimal ventilator support:
| Method | Details |
|---|---|
| T-piece | Disconnected from ventilator; breathes through heated/humidified circuit |
| Low PSV (5–8 cmH₂O) | Still connected; minimal pressure support to offset ETT resistance |
| CPAP 5 cmH₂O | Maintains PEEP; no inspiratory assistance |
SIMV-based weaning (gradual rate reduction) has the poorest weaning outcomes of all techniques and is not recommended as the primary weaning strategy.
SBT pass criteria:
- Comfortable, no marked anxiety or dyspnea
- RR < 35/min
- SaO₂ > 90%
- SBP 90–180 mmHg
- HR change < 20% from baseline
Step 4: Extubation Decision
Additional criteria beyond a passed SBT:
- Ability to follow commands
- Adequate cough and ability to manage secretions
- No excessive secretion burden
Post-extubation strategies:
- COPD patients — extubate to NIPPV → reduced mortality and HAP
- Chronic hypercapnic respiratory failure — NIPPV reduces reintubation rates
- General low-risk patients — HFNC reduces reintubation vs. conventional O₂ at 48–72h
10. Failure to Wean — Causes
| Category | Examples |
|---|---|
| Respiratory | Unresolved underlying disease; small ETT increasing resistance; auto-PEEP |
| Neuromuscular | Critical illness myopathy/polyneuropathy; prolonged NMB (especially with corticosteroids) |
| Metabolic | Non-AG metabolic acidosis → compensatory hyperventilation → fatigue; metabolic alkalosis → blunted drive → hypercapnia post-extubation |
| Psychological | Delirium, anxiety, PTSD interfering with SBTs |
| Cardiovascular | Weaning-induced cardiac ischemia or pulmonary edema (particularly in patients with LV dysfunction) |
11. Complications of Mechanical Ventilation
Pulmonary
- VILI (barotrauma, volutrauma, atelectrauma, biotrauma)
- Pneumothorax, pneumomediastinum
- Ventilator-Associated Pneumonia (VAP)
VAP — Key Facts
- Incidence: up to 15% of mechanically ventilated patients
- Mortality: ~50% when it occurs
- Defined as pneumonia ≥ 48h after intubation
- Common pathogens: S. aureus, P. aeruginosa, gram-negative enteric rods
- Empiric treatment: IV β-lactam (pip-tazo, cefepime, or ceftazidime) ± vancomycin/linezolid (for MRSA risk) or carbapenem (MDR gram-negative risk)
- Treatment duration: 7 days (shorter is non-inferior)
VAP Prevention Bundle
| Intervention | Efficacy |
|---|---|
| Head-of-bed elevation ≥ 30–45° | 70% VAP reduction |
| Subglottic secretion drainage ETT | 50% VAP reduction |
| Minimize ventilator circuit tubing changes | Reduces bacterial entry |
| Hand hygiene | Standard precaution |
| Daily sedation interruption + SBT | Reduces MV duration |
| Oral/dental hygiene | Reasonable, uncertain evidence |
Extrapulmonary Complications
- GI stress ulcers/bleeding → PPI or H₂ blocker prophylaxis
- DVT/PE → pharmacological ± mechanical prophylaxis
- Delirium and sleep disruption → minimize sedation, early mobility, day-night cycle
- ICU-acquired weakness (diaphragm and peripheral muscle atrophy) → minimize NMB, early physiotherapy
12. Hemodynamic Effects of Positive Pressure Ventilation
Positive pressure ventilation has the opposite hemodynamic effects to spontaneous breathing:
- Increases intrathoracic pressure → reduces venous return → reduces preload → may drop cardiac output
- High PEEP exaggerates this effect
- RV afterload may increase (alveolar overdistension compresses alveolar vessels)
- Clinically important in patients with hypovolemia or RV dysfunction — always assess fluid responsiveness when hemodynamic instability develops on the ventilator
Sources: Harrison's Principles of Internal Medicine 22E; Fishman's Pulmonary Diseases and Disorders; Washington Manual of Medical Therapeutics; Current Surgical Therapy 14e; Sabiston Textbook of Surgery
Reperfusion injury after tornique in regional anaesthesia
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
I now have enough from the textbooks to give a thorough answer. Let me synthesise everything.
Tourniquet Reperfusion Injury in Regional Anaesthesia
1. Background — Why Tourniquets Are Used
In regional anaesthesia (RA), a pneumatic tourniquet is routinely applied to:
- Create a bloodless surgical field (limb exsanguination with Esmarch/Martin bandage)
- Confine local anaesthetic to the limb in Intravenous Regional Anaesthesia (IVRA / Bier block)
- Reduce intraoperative blood loss in procedures like Total Knee Arthroplasty (TKA)
Standard pressure: 250 mmHg or 50–100 mmHg above systolic BP
Maximum safe ischemia time: 2 hours (historically); after which the cuff is deflated for at least 15 minutes of reperfusion before re-inflation
2. The Core Problem — Ischemia-Reperfusion Injury (IRI)
Tourniquet inflation creates a period of complete limb ischemia. Paradoxically, the injury is not just from the ischemia itself — restoration of blood flow (reperfusion) triggers a second wave of tissue damage.
"Prolonged distal ischemia can result in venous congestion or muscle damage and reperfusion injury after release." — Sabiston Textbook of Surgery
"When blood flow is restored to ischemic tissues, cells that might otherwise recover are damaged by new processes set in motion during reperfusion." — Robbins & Cotran Pathologic Basis of Disease
3. Mechanisms of Reperfusion Injury
Four interacting pathophysiological mechanisms operate simultaneously on tourniquet release:
A. Reactive Oxygen Species (ROS) / Oxidative Stress
- During ischemia, xanthine dehydrogenase is converted to xanthine oxidase in endothelial cells
- On reperfusion, oxygen returns → xanthine oxidase uses it to generate superoxide (O₂⁻), hydrogen peroxide (H₂O₂), and hydroxyl radicals (·OH)
- Leukocytes recruited to the ischemic zone are a major additional source of ROS via NADPH oxidase
- Cellular antioxidant defenses (superoxide dismutase, catalase, glutathione) are depleted during ischemia, so cells are hypersensitive to ROS on reflow
- ROS cause: lipid peroxidation of cell membranes, DNA strand breaks, protein oxidation, mitochondrial dysfunction
B. Intracellular Calcium Overload
- Ischemia impairs Na⁺/K⁺-ATPase and Na⁺/Ca²⁺ exchanger → intracellular Na⁺ rises → intracellular Ca²⁺ accumulates
- On reperfusion, ROS further damage the sarcoplasmic reticulum and cell membranes → Ca²⁺ influx is amplified
- High intracellular Ca²⁺ → opens the mitochondrial permeability transition pore (mPTP) → ATP depletion → cell death
- In muscle: pathological Ca²⁺ accumulation → contraction band necrosis
C. Neutrophil-Mediated Inflammation
- Ischemic cells release DAMPs (damage-associated molecular patterns) and cytokines
- Endothelial cells upregulate adhesion molecules (ICAM-1, selectins) → neutrophils adhere and extravasate
- Infiltrating neutrophils release ROS (respiratory burst), proteases, and elastase → amplify tissue damage
- Complement activation (via IgM antibodies deposited in ischemic tissue) further fuels the inflammatory cascade
D. Endothelial Dysfunction
- Reperfused endothelium loses its anti-thrombotic, vasodilatory properties
- Reduced nitric oxide (NO) production → vasoconstriction, platelet aggregation
- Increased endothelin-1 → further vasoconstriction → "no-reflow" phenomenon in microcirculation
- Pro-thrombotic state → microvascular thrombosis → secondary ischemia despite macrovascular patency
4. Tissues Affected in the Limb
| Tissue | Mechanism | Clinical Result |
|---|---|---|
| Skeletal muscle | ROS + Ca²⁺ + neutrophil infiltration | Myonecrosis, rhabdomyolysis, compartment syndrome |
| Peripheral nerves | Ischemia + mechanical compression under cuff | Neuropraxia, axonotmesis; tourniquet palsy |
| Vascular endothelium | ROS, ICAM-1, platelet aggregation | No-reflow, thrombosis |
| Skin | Direct pressure + ischemia | Blistering, pressure necrosis under cuff |
5. Systemic Effects at Tourniquet Release
When the tourniquet is deflated, all accumulated metabolites from the ischemic limb are washed into the systemic circulation simultaneously:
| Parameter | Change | Clinical Significance |
|---|---|---|
| PaCO₂ | ↑ (CO₂ washout from ischemic limb) | Transient hypercapnia |
| pH | ↓ (lactic acidosis + CO₂) | Metabolic + respiratory acidosis |
| Potassium | ↑ | Risk of arrhythmia (especially in bilateral TKA or prolonged tourniquet) |
| Temperature | ↓ (cold ischemic blood returns) | Core temperature drop |
| Mean arterial pressure | ↓ | Peripheral vasodilation from ischemic metabolites; requires vasopressor support if severe |
| Heart rate | ↑ reflex | Compensatory tachycardia |
| PaO₂ | ↓ transiently | Ischemic blood mixing with arterial blood |
"After tourniquet release, mean arterial blood pressure decreases significantly, partly owing to the release of metabolites from the ischemic limb into the circulation and the decrease in peripheral vascular resistance." — Miller's Anesthesia, 10e
This is especially relevant under regional anaesthesia because:
- Sympathetic block from neuraxial/peripheral RA already attenuates compensatory vasoconstriction
- Vasodilation from RA + vasodilation from tourniquet release can combine to produce profound hypotension
- Opioid adjuncts to spinal/epidural anaesthesia partially attenuate tourniquet pain but not the hemodynamic response
6. Tourniquet Pain Under Regional Anaesthesia
A specific clinical challenge is tourniquet pain, which occurs despite apparently adequate RA:
- Develops after ~60 minutes of inflation
- Mechanism: unmyelinated C fibers (carrying dull aching pain) are resistant to or "outlast" the block on slow-conducting nerve fibers; as the neuraxial/peripheral block recedes, C fibers become unblocked
- Under spinal anaesthesia: a dense sacral/lumbar block may cover surgery but C fibers eventually breakthrough
- Under peripheral nerve block: some C-fiber pathways may escape blockade
- Management:
- Add opioids to spinal/epidural (e.g., fentanyl, morphine) — reduces tourniquet pain
- Double cuff technique in IVRA: inflate distal cuff over anaesthetized skin, then deflate proximal cuff — delays pain
- Ketamine sub-dissociative doses IV
- Limit tourniquet time to < 60–90 minutes where possible
7. Specific Context: IVRA (Bier Block) and Reperfusion
In IVRA, the tourniquet serves a dual role — it confines local anaesthetic and creates the bloodless field. The critical risk at tourniquet deflation is not only reperfusion injury but also local anaesthetic systemic toxicity (LAST):
- Local anaesthetic (typically lidocaine 0.5%, 3 mg/kg; or prilocaine in UK/Europe) is retained by the tourniquet
- If the cuff deflates before 30 minutes, a bolus of LA enters the systemic circulation → LAST (seizures, cardiovascular collapse)
- After 45 minutes, much of the LA is protein-bound or redistributed → risk greatly reduced
- On deflation: cyclic deflation (inflate-deflate-inflate for 5-second cycles) reduces peak plasma LA concentration
The reperfusion on Bier block deflation additionally delivers:
- Ischemic metabolites (lactic acid, K⁺, CO₂)
- Any unbound LA in the limb vasculature
- Pro-inflammatory cytokines
8. Nerve Injury — Tourniquet Neuropraxia
- Nerve injury from tourniquet is attributable to the combined effects of ischemia and mechanical compression at the cuff site
- The radial nerve at the spiral groove (upper arm) and the common peroneal nerve at the fibular neck (lower limb) are most vulnerable
- Clinically: post-tourniquet syndrome — weakness, paralysis, paresthesia in the distribution of the compressed nerve
- Usually neuropraxia (demyelination without axon loss) → recovers in days to weeks
- Prolonged inflation > 2 hours, excessive pressure, or poor cuff placement → axonotmesis (wallerian degeneration) → slower recovery
"Nerve injury after tourniquet inflation has been attributed to the combined effects of ischemia and mechanical trauma. When prolonged tourniquet inflations are required, deflating the tourniquet for 30 minutes of reperfusion may reduce neural ischemia." — Miller's Anesthesia, 10e
9. Special Populations — Higher Risk of IRI
| Population | Additional Risk |
|---|---|
| Peripheral vascular disease | Baseline poor perfusion; collateral collapse during ischemia |
| Sciatic neuropraxia / pre-existing neuropathy | May worsen; tourniquet often avoided |
| Bilateral TKA | Dual metabolite load on deflation → greater hemodynamic instability, higher K⁺ load, fat embolism risk |
| Sickle cell disease | Sickling in hypoxic, acidotic ischemic environment → vascular occlusion |
| Diabetic neuropathy | Vulnerable nerves more susceptible to compression |
"In patients with known preexisting sciatic neuropraxias, neuropathic pain, and vascular disease in the operative leg, the operation can be performed without a tourniquet." — Miller's Anesthesia, 10e
10. Prevention and Mitigation Strategies
| Strategy | Mechanism | Evidence |
|---|---|---|
| Limit inflation time to < 2 hours | Reduces ischemic metabolite accumulation | Standard practice |
| Reperfusion intervals (deflate 30 min) | Allows washout of metabolites before re-inflation | Reduces neural ischemia |
| Graduated cuff pressure | Minimum effective pressure (LOP + 40 mmHg) rather than fixed 250 mmHg | Reduces nerve compression force |
| Limb elevation before exsanguination (in infection/tumour) | Avoids Esmarch embolic spread | Standard practice |
| Remote Ischemic Preconditioning (RIPC) | Brief tourniquet inflation-deflation cycles on a remote limb prior to the main ischemic insult → activates endogenous cytoprotective pathways (adenosine, K-ATP channels, NO) | Studied in cardiac/renal surgery; early data in orthopaedics |
| Antioxidant pretreatment (N-acetylcysteine, allopurinol) | Scavenge ROS on reperfusion | Experimental; not routine |
| Fluid loading before deflation | Blunts hypotension from vasodilation | Practical clinical measure |
| Vasopressors ready | Treats hypotension post-deflation | Standard ICU/theatre preparation |
Summary
| Phase | Key Event | Clinical Consequence |
|---|---|---|
| Tourniquet inflation | Limb ischemia | Muscle & nerve ischemia; anaerobic metabolism; lactate/K⁺ accumulation |
| > 60 min inflation | C-fiber breakthrough | Tourniquet pain despite RA |
| Tourniquet deflation | Reperfusion + metabolite washout | ↓ MAP, ↑ CO₂, ↑ K⁺, ↓ temperature; possible arrhythmia |
| Reperfusion (minutes–hours) | ROS burst, Ca²⁺ overload, neutrophil influx | Muscle necrosis, nerve injury, compartment syndrome |
| IVRA-specific | LA systemic bolus on deflation | LAST risk (seizures, cardiac arrest) |
Sources: Robbins & Cotran Pathologic Basis of Disease; Miller's Anesthesia, 10e; Sabiston Textbook of Surgery; Barash Clinical Anesthesia, 9e; Brenner & Rector's The Kidney
Spinal needles with diagram in Anesthesia
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Searching Images
spinal needle types Quincke Whitacre Sprotte tip design comparison
Loading Image
Finding Sources
I now have all the content and images needed for a comprehensive answer.
Spinal Needles in Anaesthesia
Overview
Spinal needles are purpose-built for subarachnoid (intrathecal) injection during spinal anaesthesia. All modern spinal needles share four basic features:
- A tightly fitting, removable stylet that completely occludes the lumen — to prevent tracking epithelial cells into the subarachnoid space
- A hub for syringe attachment and for feeling needle advancement
- A shaft of varying length (standard ~90 mm for adults) and gauge (16–29 G)
- A tip design — the most important variable in clinical practice
"The most important characteristics of a spinal needle are the shape of the tip and the needle diameter." — Miller's Anesthesia, 10e
Classification by Tip Design
Spinal needles fall into two fundamental categories:
| Category | Type | Mechanism of Dural Entry |
|---|---|---|
| Cutting (bevelled) | Quincke, Pitkin | Sharp bevelled edge cuts through dural fibres |
| Non-cutting (pencil-point / atraumatic) | Whitacre, Sprotte, Pencan, Gertie Marx | Blunt conical tip separates/splits dural fibres |
Diagram — Tip Designs
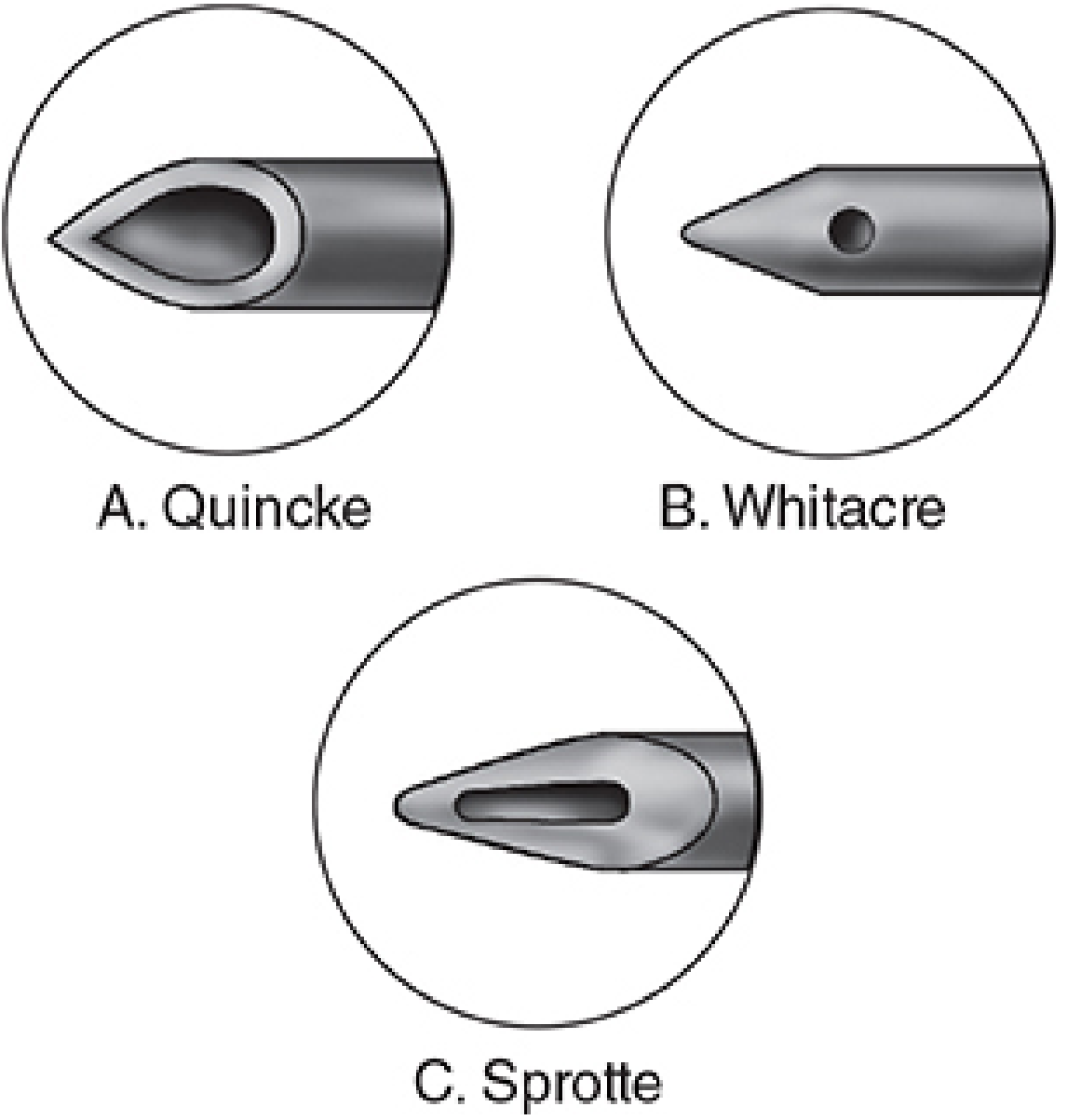
Tip designs of the three main spinal needles. A: Quincke — sharp bevelled cutting tip, end injection. B: Whitacre — conical pencil-point, small side injection port. C: Sprotte — conical pencil-point, large elongated side injection port. — Morgan & Mikhail's Clinical Anesthesiology, 7e
Scanning Electron Micrograph — Actual Needle Tips
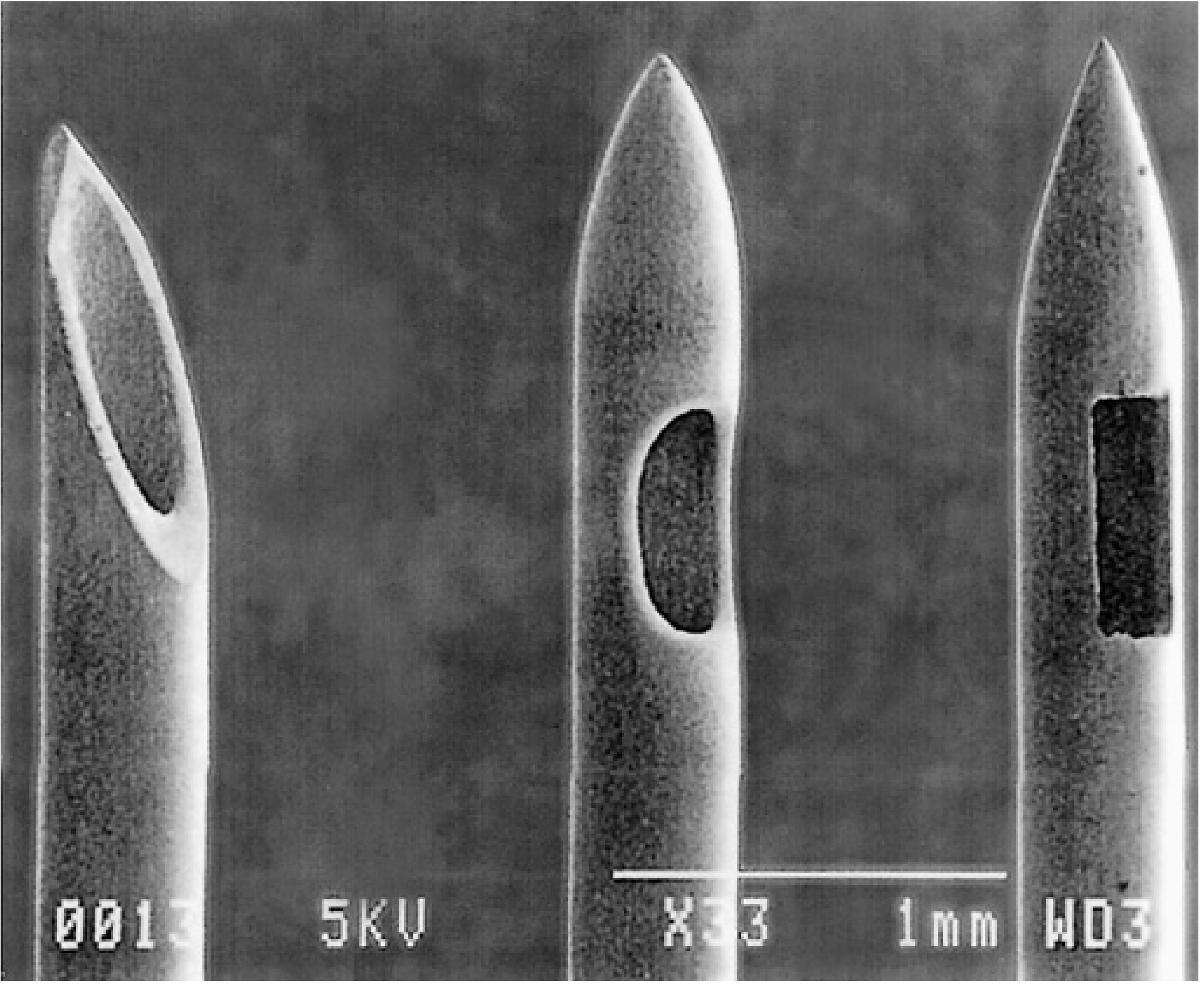
Scanning electron micrographs of spinal needle tips: Quincke (left) — angled cutting bevel; Sprotte (centre) — conical atraumatic tip with large oval lateral port; Whitacre (right) — conical atraumatic tip with smaller rectangular lateral port. Scale bar = 1 mm. — Miller's Anesthesia, 10e
Individual Needle Types
1. Quincke Needle (Cutting, End-Injection)
- Tip: Sharp cutting bevel, angled ~45°
- Injection: From the end of the needle (bevel)
- Available gauges: 20–29 G
- CSF flow: Fast and reliable — easy to confirm placement
- PDPH risk: Highest — the sharp bevel cuts dural fibres longitudinally, leaving a slit that CSF leaks through
- Key clinical rule: Orient bevel parallel to the longitudinal axis of the spine (parallel to dural fibres) — this parts fibres rather than cutting across them, reducing PDPH incidence
- Advantages: Reliable, inexpensive, excellent tactile feedback
- Disadvantages: Higher PDPH, not preferred as first choice for elective spinal
2. Whitacre Needle (Pencil-Point, Side-Injection)
- Tip: Solid conical pencil-point — separates rather than cuts dural fibres
- Injection: Side port (small circular or oval aperture just proximal to the tip)
- Available gauges: 22–27 G (most commonly 25–27 G)
- CSF flow: Slightly slower than Quincke of equivalent gauge (due to side port)
- PDPH risk: Markedly lower than Quincke — dural fibres are separated and recoil closed after withdrawal
- Advantages: Low PDPH, good tactile feedback
- Disadvantages: Slightly higher failure rate at very fine gauges; aspiration may be needed to confirm CSF in ≤25 G
3. Sprotte Needle (Pencil-Point, Long Side-Opening)
- Tip: Solid conical pencil-point (similar to Whitacre)
- Injection: Long elongated oval side port — significantly larger than Whitacre
- Available gauges: 24–29 G
- CSF flow: Fastest among pencil-point needles due to the large side opening
- PDPH risk: Low (similar to Whitacre)
- Unique risk: If the tip is subarachnoid (CSF flows freely) but the proximal part of the long port is not yet past the dura, part of the injected dose is delivered outside the subarachnoid space → failed or patchy block
- Advantages: Excellent CSF flow, low PDPH
- Disadvantages: Larger side port → risk of incomplete intrathecal injection
4. Pencan Needle
- Similar pencil-point design to Whitacre/Sprotte
- Belongs to the non-cutting group
- Available in 25–27 G
- Used in combined spinal-epidural (CSE) kits
5. Pitkin Needle (Cutting)
- Cutting tip (similar to Quincke in concept)
- Less commonly used in modern practice
- Listed among cutting-tip needles in Miller's Anesthesia
Combined Spinal-Epidural (CSE) Setup
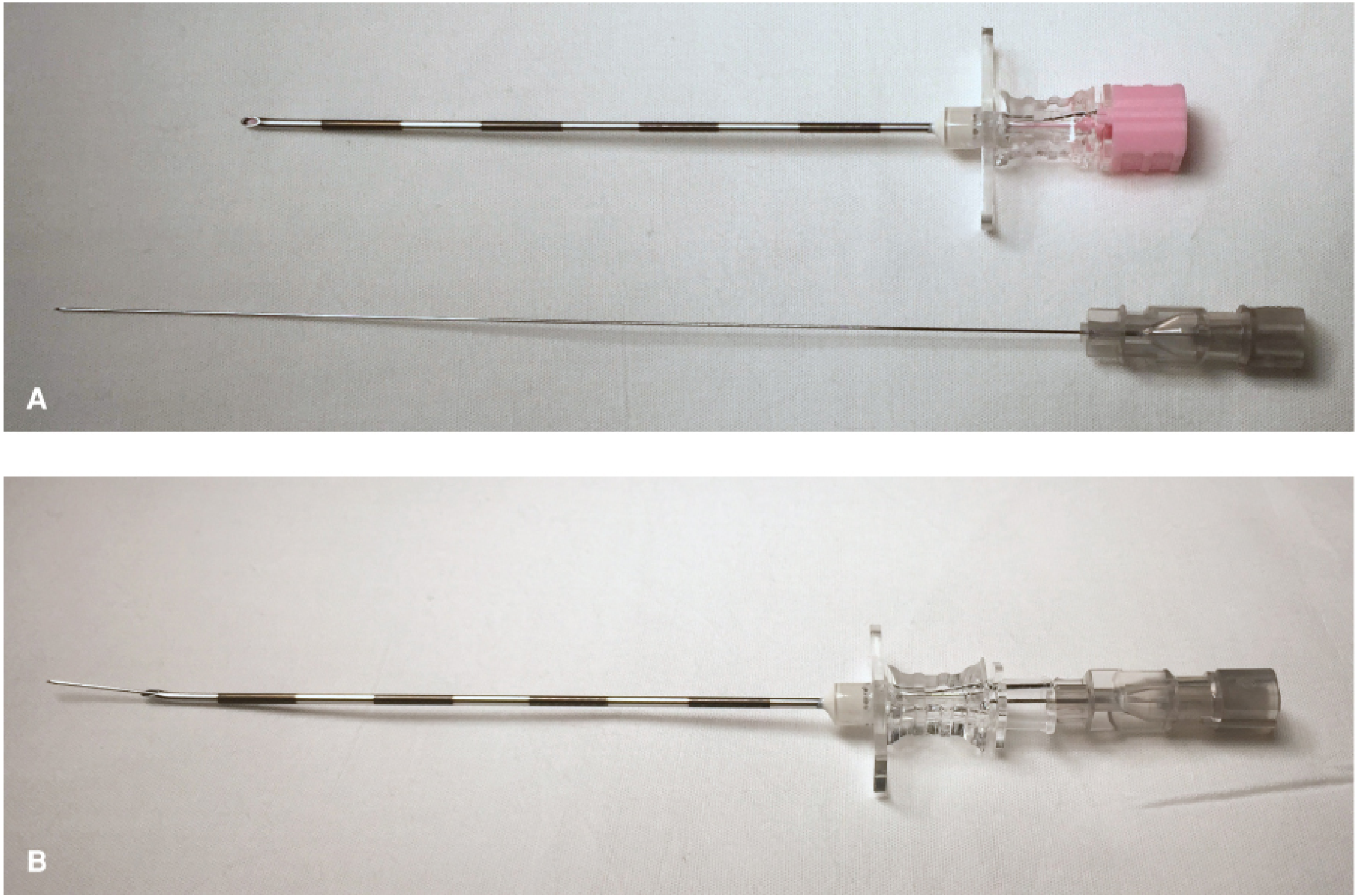
CSE technique: A 27G Whitacre spinal needle passed through an 18G Tuohy epidural needle. After intrathecal injection, the spinal needle is removed and an epidural catheter is threaded. — Barash Clinical Anesthesia, 9e
In CSE technique:
- The Tuohy (epidural) needle is sited in the epidural space first (loss of resistance technique)
- A long fine-gauge pencil-point spinal needle is then passed through the Tuohy lumen, penetrating the dura ("needle through needle")
- Intrathecal injection is made → spinal needle removed → epidural catheter threaded
- The spinal needle must protrude 2–3 mm beyond the Tuohy tip to reach the subarachnoid space
Gauge and PDPH — Key Data
| Gauge | PDPH Incidence |
|---|---|
| 22G cutting (Quincke) | ~40% |
| 25G pencil-point | ~2–5% |
| 27G pencil-point | ~1–2% |
| 29G pencil-point | < 2% |
"The use of small-gauge needles reduces the incidence of post-dural puncture headache from 40% with a 22G needle to less than 2% with a 29G needle. The probability of PDPH or procedure failure is reportedly lowest with 26G atraumatic needles." — Miller's Anesthesia, 10e
Trade-off with very fine gauges (29G):
- Lower PDPH
- But higher procedural failure rate — weaker tactile feedback, slower CSF flow (aspiration needed to confirm), needle deflects in tissue
The Introducer Needle
Fine-gauge spinal needles (≤25G) are too flexible to be inserted directly through skin and deeper tissues. An introducer (finder) needle (typically 19G, 38 mm long) is used:
- Inserted first into subcutaneous/interspinous tissues (not beyond ligamentum flavum)
- Acts as a guide and stiffener for the finer spinal needle
- Prevents contamination of the spinal needle tip with skin flora/epidermal cells
- Note: The introducer itself has a bevelled tip → if it accidentally enters the subarachnoid space in a thin patient, orient bevel parallel to the spine axis to minimise PDPH
Summary Comparison Table
| Feature | Quincke | Whitacre | Sprotte |
|---|---|---|---|
| Tip type | Cutting bevel | Pencil-point | Pencil-point |
| Injection site | End | Side (small port) | Side (long oval port) |
| PDPH risk | Highest | Low | Low |
| CSF flow | Fast | Moderate | Fastest (pencil-point) |
| Tactile feedback | Good | Good | Good |
| Failure risk | Low | Low | Risk of partial extra-dural injection if port not fully advanced |
| Gauges available | 20–29G | 22–27G | 24–29G |
| Common clinical use | Diagnostic LP, emergencies, obstetric (with care) | Elective spinal, CSE | Elective spinal |
| Dural mechanism | Cuts fibres → slit | Separates fibres → recoil | Separates fibres → recoil |
Clinical Tips
- Bevel orientation for Quincke: Always insert with bevel parallel to the spine's long axis — reduces PDPH by parting rather than severing dural fibres (longitudinal orientation)
- Confirm CSF with fine gauges: With 25G and smaller, remove stylet after each "pop"; active aspiration may be needed
- The Sprotte "partial injection" trap: Ensure the long side port is fully through the dura before injecting
- NR-Fit (non-Luer) connectors: Newer spinal kits use non-standard connectors to prevent accidental intrathecal injection of wrong drugs — rely on the correct drug being drawn up into the non-Luer syringe
- Sterility is paramount: Wear a mask — Streptococcus viridans (oral commensal) is a leading cause of post-spinal bacterial meningitis; full aseptic technique including hand wash, gloves, drape, and chlorhexidine-alcohol skin prep is mandatory
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e; Miller's Anesthesia, 10e; Barash, Cullen & Stoelting's Clinical Anesthesia, 9e
This is a shared conversation. Sign in to Orris to start your own chat.