Rheumatic heart disease Pathology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have all the content and images needed. Here is the comprehensive answer:
Rheumatic Heart Disease - Pathology
Overview
Rheumatic heart disease (RHD) is the cardiac manifestation of acute rheumatic fever (ARF), an immunologically mediated, multisystem inflammatory disease triggered by Group A beta-hemolytic streptococcal (GAS) pharyngeal infection. It is characterized by inflammation of all three layers of the heart (pancarditis), but valvular scarring produces the most clinically significant, permanent damage.
RHD remains the most important form of acquired heart disease in children and young adults in low-income countries. In high-income countries, its incidence has fallen dramatically due to improved socioeconomic conditions, rapid antibiotic treatment, and declining streptococcal virulence.
Pathogenesis
The characteristic 2-3 week latency between streptococcal infection and symptom onset reflects the time needed to mount an immune response. The core mechanism is molecular mimicry:
- Antibodies and CD4+ T cells directed against streptococcal M proteins cross-react with cardiac antigens (myocardial, valvular, and pericardial)
- Cross-reactive autoantibodies target: streptococcal carbohydrate epitope (N-acetyl-beta-D-glucosamine / GlcNAc), laminin in valve endothelium, and cardiac myosin
- Anti-body binding activates complement and recruits Fc-receptor-bearing neutrophils and macrophages
- Cytokine release by stimulated T cells leads to macrophage activation within Aschoff bodies
- Streptococci are completely absent from the lesions - confirming the immunological basis
- Only 0.3% to 3% of those with streptococcal infection develop RF, implying an underlying genetic susceptibility (HLA class II alleles are implicated; heritability estimated at ~60%)
Morphology: Acute Rheumatic Fever (Pancarditis)
During the acute phase, focal inflammatory lesions are found in all three layers of the heart.
1. The Aschoff Body (Pathognomonic Lesion)
The Aschoff body (also called Aschoff-Geipel body) is the hallmark granulomatous lesion of rheumatic fever, found in the myocardium. It is pathognomonic for this disease.
Composition:
- Central zone of fibrinoid necrosis
- Surrounding infiltrate of T lymphocytes (primarily), plasma cells
- Plump activated macrophages called Anitschkow cells (also called "caterpillar cells")
Anitschkow cells have:
- Abundant cytoplasm
- Central round-to-ovoid nuclei (occasionally binucleate)
- Chromatin condensed into a slender, central, wavy ribbon - classically described as the "caterpillar nucleus" or "owl-eye" nucleus on cross-section
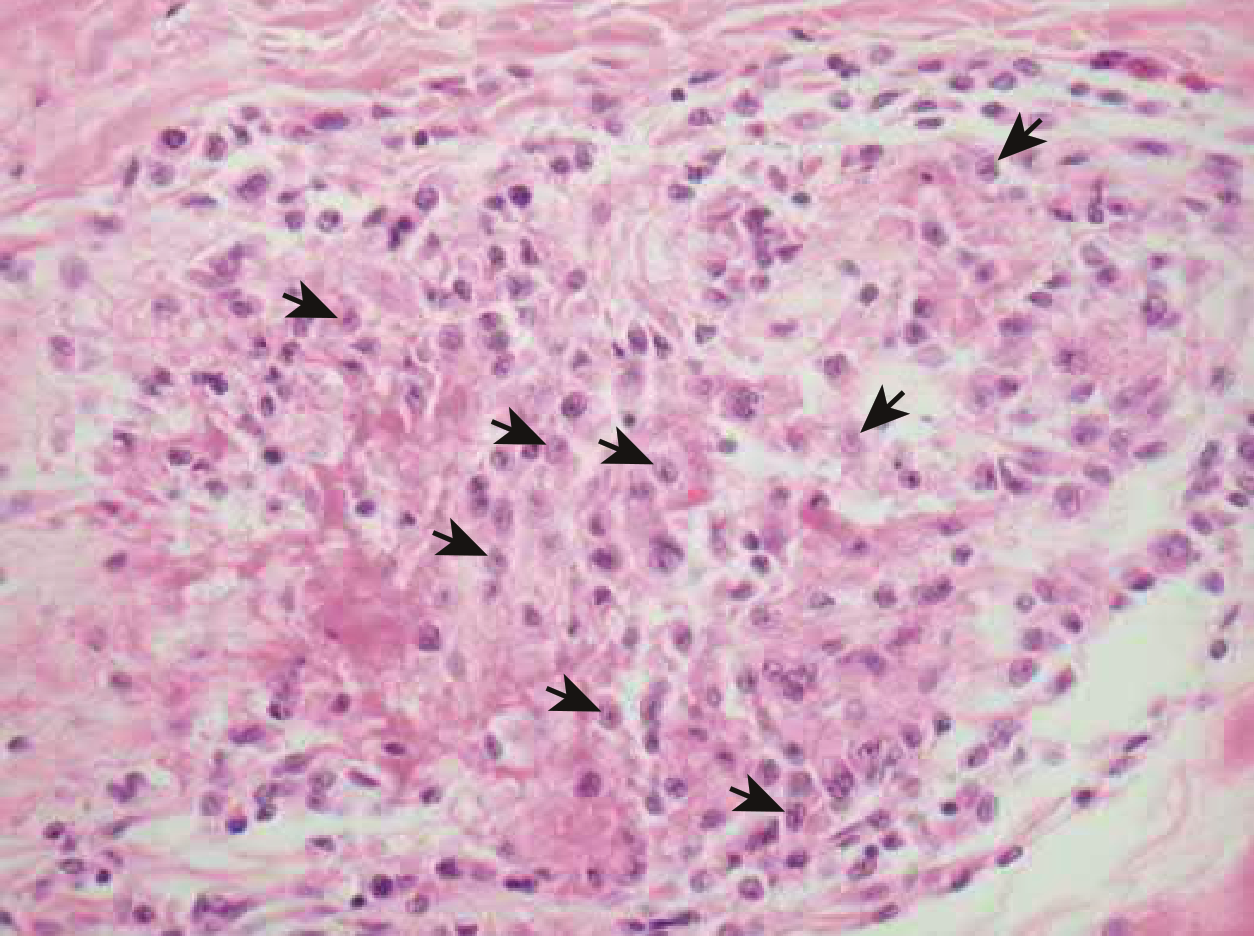
Aschoff body (Braunwald's Heart Disease): Anitschkow cells (arrows) with their characteristic caterpillar nuclei, surrounded by mononuclear infiltrate. Adjacent myocardial fibers are undergoing destruction.
2. Endocarditis (Most Clinically Important)
- Inflammation of the endocardium and left-sided valves causes fibrinoid necrosis within cusps or tendinous cords
- Overlying necrotic foci along the lines of closure form small (1-2 mm) verrucae (vegetations)
- These are sterile, flat, wartlike deposits - unlike the bulky vegetations of infective endocarditis
- MacCallum plaques: irregular subendocardial thickenings in the left atrium, often on the posterior wall, caused by regurgitant jet injury
3. Myocarditis
- Diffuse interstitial Aschoff bodies throughout the myocardium
- May be sufficiently severe to cause cardiac dilation and functional mitral insufficiency in acute phase
4. Pericarditis
- Fibrinous, sometimes with effusion ("bread-and-butter" pericarditis)
- Occurs only alongside endocardial inflammation
- Generally subsides without permanent damage
Morphology: Chronic Rheumatic Heart Disease
The chronic fibrotic lesions are the predictable consequence of healing and scarring. Clinical manifestations appear years to decades after the initial acute episode. Each recurrence of ARF adds cumulative damage.
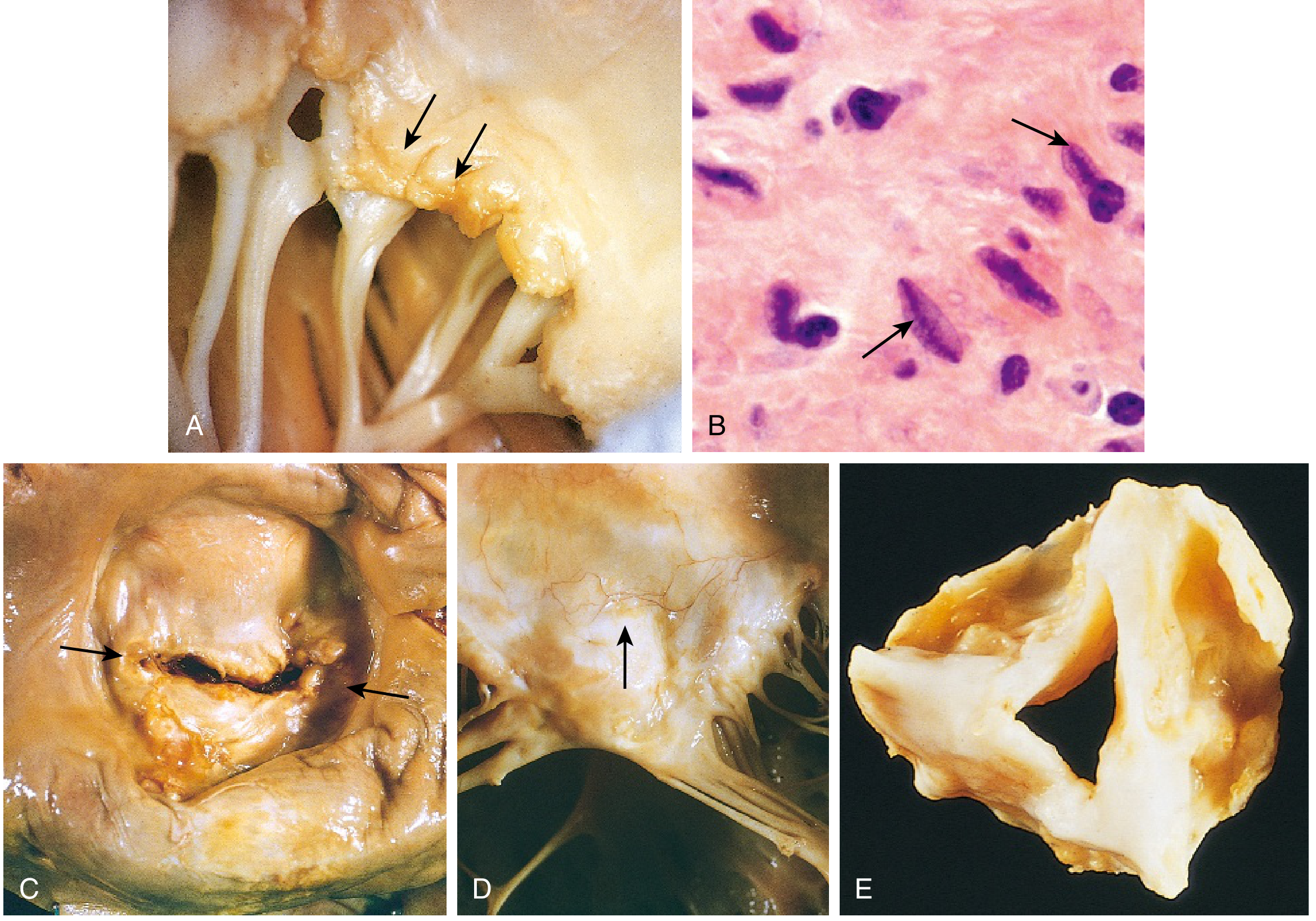
(A) Acute rheumatic mitral valvulitis: small verrucae along the line of valve closure (arrows), with fibrous thickening and fusion of chordae. (B) Aschoff body: Anitschkow cells with caterpillar chromatin. (C) Chronic mitral stenosis viewed from above: commissural fusion (arrows). (D) Anterior mitral leaflet: neovascularization (arrow). (E) Rheumatic aortic stenosis: thickening and commissural fusion.
Valve Changes
The cardinal anatomic changes in the chronic mitral valve:
| Feature | Detail |
|---|---|
| Leaflet thickening | Progressive fibrosis obliterates normal architecture |
| Commissural fusion | Leaflets fuse at the edges - most characteristic change |
| Chordae tendineae | Thickened, shortened, fused |
| Calcification | Progressive calcification of valvular and subvalvular apparatus |
| Neovascularization | New vessel ingrowth visible in leaflets |
| Overall shape | Funnel-shaped valve with domed leaflets; "fish-mouth" orifice |
Aschoff bodies are rarely found in chronic RHD surgical specimens or autopsy tissue due to the long interval between the initial insult and development of the deformity.
Valve Frequency of Involvement
| Valve | Frequency |
|---|---|
| Mitral alone | ~70% (isolated); ~two-thirds of all chronic RHD |
| Mitral + Aortic | ~25% |
| Tricuspid | Infrequent, less severe |
| Pulmonary | Almost always spared |
RHD is essentially the only cause of acquired mitral stenosis. Mitral regurgitation is the most common valvular abnormality in RHD overall.
Microscopic Changes (Chronic)
- Organization of acute inflammation
- Post-inflammatory neovascularization within leaflets
- Transmural fibrosis obliterating the normal leaflet architecture
- Aschoff bodies absent or rare
Consequences of Chronic RHD
- Mitral stenosis - progressive left atrial dilation; normal valve area (4-5 cm²) reduced to ≤1.5 cm² in severe disease
- Atrial fibrillation - from left atrial pressure overload and dilation
- Mural thrombi - fertile substrate from dilated, fibrillating left atrium; risk of systemic thromboembolism (stroke)
- Pulmonary hypertension - from long-standing elevated left atrial pressure transmitted to pulmonary vasculature
- Right ventricular hypertrophy/failure - secondary to pulmonary hypertension
- Left ventricle - generally normal in pure mitral stenosis
- Infective endocarditis - scarred, deformed valves are highly susceptible
- Arrhythmias (atrial fibrillation predominates)
Summary Table: Acute vs. Chronic RHD Pathology
| Feature | Acute RHD | Chronic RHD |
|---|---|---|
| Lesion type | Aschoff bodies, fibrinoid necrosis | Fibrosis, calcification, commissural fusion |
| Valve vegetations | Small (1-2 mm) verrucae along line of closure | None; replaced by fibrous scar |
| Aschoff bodies | Present (pathognomonic) | Absent/rare |
| Chordae tendineae | Mild involvement | Shortened, thickened, fused |
| Pericardium | Fibrinous pericarditis | Usually no permanent damage |
| Valve shape | Near normal outline, inflamed | "Fish-mouth" / funnel-shaped stenosis |
| Left atrium | Mildly affected | Markedly dilated |
Sources:
- Robbins & Kumar Basic Pathology, Chapter 9 (Valvular Heart Disease)
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 12
- Braunwald's Heart Disease, Chapter 81 (Pathologic Features)
- Schwartz's Principles of Surgery, 11th Ed., Chapter 21 (Mitral Valve Disease)
This is a shared conversation. Sign in to Orris to start your own chat.