Drug induced oxidative stress in neurotoxicity
"drug-induced" AND "oxidative stress" AND "neurotoxicity"
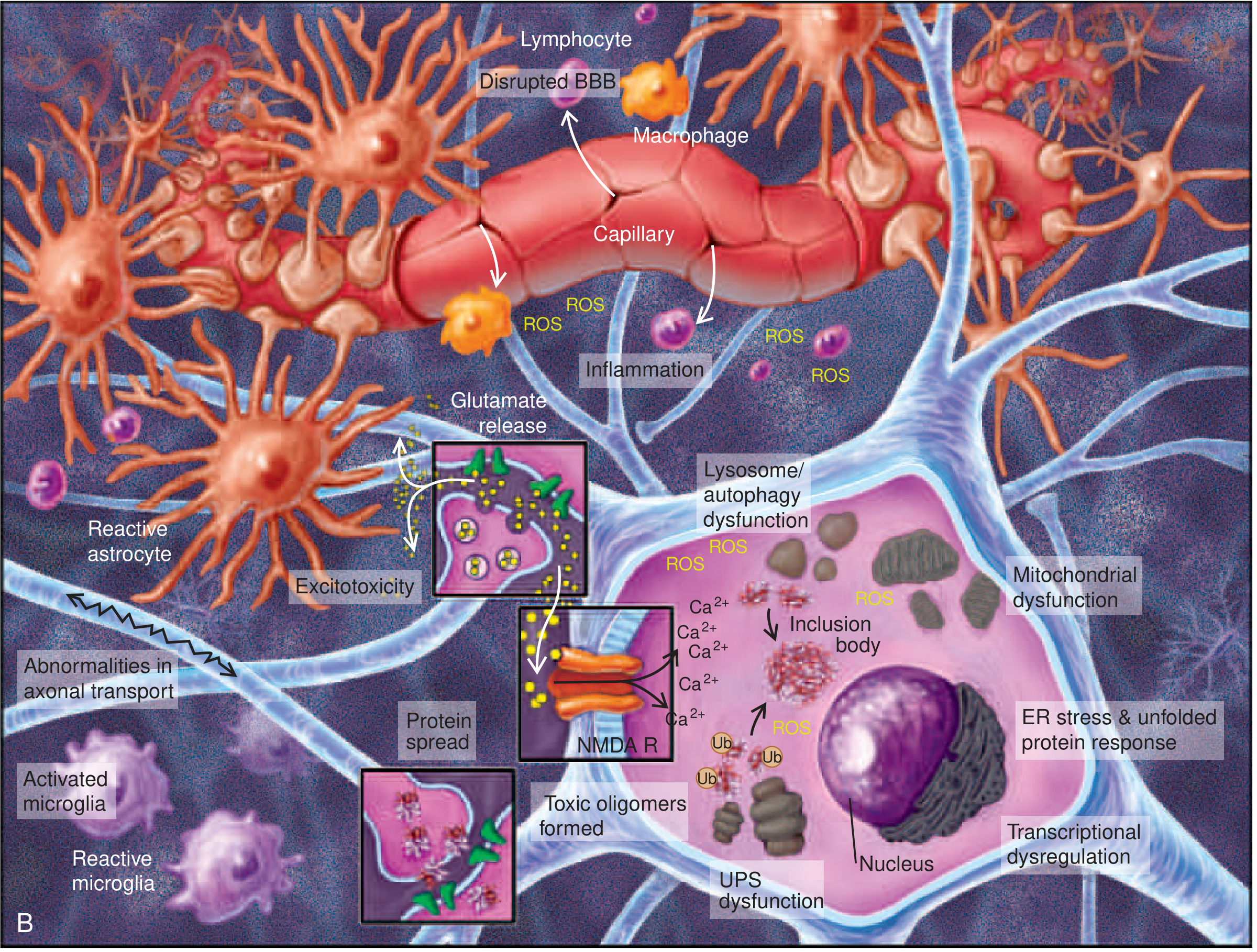
Drug-Induced Oxidative Stress in Neurotoxicity
1. The Oxidative Stress Framework in the Nervous System
2. Core Molecular Mechanisms
2a. Mitochondrial Dysfunction → ROS Generation
- Heavy metals (manganese, lead, arsenic)
- Certain chemotherapy agents
- Drugs of abuse (methamphetamine, alcohol)
2b. Excitotoxicity and Calcium-Mediated ROS
2c. Dopamine Auto-oxidation
- H₂O₂ (hydrogen peroxide)
- Superoxide radicals
- Dopamine-quinones (highly reactive, directly toxic to mitochondria and proteins)
3. Drug-Specific Mechanisms
3a. Methamphetamine and Stimulants
- Massive dopamine release from vesicular stores → dopamine auto-oxidation → H₂O₂ and superoxide formation
- Free radical production - highly reactive peroxides and ROS directly damage dopaminergic and serotonergic terminals
- Excitotoxicity - excess glutamate activity → NMDA receptor overactivation → Ca²⁺ influx → ROS amplification
- Neuroinflammation - activation of astrocytes and microglia → cytokine storm (TNF-α, IL-1β, IL-6) → further ROS generation
- Hyperthermia - methamphetamine-induced hyperthermia amplifies all oxidative processes
3b. Alcohol (Ethanol)
- Direct oxidative stress via ethanol metabolism (CYP2E1 pathway generates ROS)
- Glutamate excitotoxicity - chronic alcohol suppresses NMDA receptors; upon withdrawal, rebound NMDA hyperactivity floods neurons with Ca²⁺ and ROS
- Combined with thiamine (B1) deficiency in alcoholics → Wernicke-Korsakoff syndrome (though the direct toxic oxidative effect is distinct from nutritional deficiency)
3c. Manganese (Mn)
- Accumulates in the globus pallidus and striatum (unlike Parkinson disease, which targets substantia nigra)
- Mn²⁺/Mn³⁺ redox cycling generates ROS via Fenton-like reactions
- Disrupts GABAergic and glutamatergic neurotransmitter synthesis and metabolism
- Impairs mitochondrial function in dopaminergic neurons
3d. Lead (Pb)
- Oxidative stress (possibly via impaired antioxidant enzyme activity and direct mitochondrial damage)
- Disruption of calcium-dependent cell signaling (Pb²⁺ substitutes for Ca²⁺)
- Inhibition of nitric oxide synthase
- Altered glutamatergic signaling (inhibits NMDA receptors, disrupting synaptic plasticity)
3e. Chemotherapy Agents
- Vinca alkaloids (vincristine, vinblastine) → axonal degeneration → "stocking-glove" sensorimotor neuropathy with pain, loss of DTRs
- Cisplatin → sensorimotor neuropathy and ototoxicity (especially >400 mg/m²), partly via ROS-mediated cochlear hair cell damage
- Antibody-drug conjugates (ADCs) (e.g., brentuximab vedotin) → significant central and peripheral neurotoxicity, dose-dependent
- "Chemo brain" (chemotherapy-related cognitive impairment) - occurs in ~35% of cancer survivors; mechanisms include neurodegeneration, immune dysregulation, cytokine production, and oxidative stress gene polymorphisms
3f. HIV Antiretroviral Drugs + HIV Itself
- HIV-1 proteins gp120 and Tat trigger macrophages and microglia to release neurotoxins
- Monocyte-derived neurotoxic factors kill neurons via NMDA receptor activation and induction of oxidative stress
- Cytokines (TNF-α, IL-1, IL-6) amplify ROS production
- gp120 elevates intracellular Ca²⁺ and reduces neurotrophic factor levels
- Certain antiretroviral drugs (particularly older NRTIs) carry their own neurotoxic potential
4. Convergent Downstream Pathways
| Pathway | Mechanism | Outcome |
|---|---|---|
| Lipid peroxidation | ROS attack polyunsaturated fatty acids in membranes | Membrane disruption, cell death |
| Protein carbonylation | ROS oxidize proteins → loss of function | Proteasome overload, inclusion bodies |
| DNA oxidation | 8-OH-deoxyguanosine formation | Mutation, apoptosis |
| Mitochondrial membrane permeability | Cytochrome C release | Caspase activation → apoptosis |
| BBB disruption | ROS damage tight junctions | Peripheral immune cell entry → more inflammation |
| ER stress / UPR | Misfolded proteins overwhelm ER | Apoptotic signaling via CHOP/caspase-12 |
| Neuroinflammation | ROS activate NF-κB in microglia | Sustained cytokine release → secondary ROS |
5. Antioxidant Defense Systems and Their Pharmacological Failure
- N-acetylcysteine (GSH precursor)
- Vitamin E / Vitamin C supplementation
- Selenium-dependent glutathione peroxidase support
6. Recent Evidence (PubMed, 2025)
Summary Table: Drug-Induced Oxidative Stress in Neurotoxicity
| Drug/Agent | Primary ROS Source | Key Brain Region Affected | Clinical Syndrome |
|---|---|---|---|
| Methamphetamine | Dopamine auto-oxidation, mitochondrial dysfunction | Striatum, prefrontal cortex | Parkinsonism, psychosis, cognitive decline |
| Alcohol | CYP2E1-mediated ROS; NMDA rebound on withdrawal | Cerebellum (Purkinje cells), cortex | Cerebellar ataxia, dementia, neuropathy |
| Manganese | Mn redox cycling (Fenton-like) | Globus pallidus, striatum | Manganism (parkinsonism-like) |
| Lead | Mitochondrial impairment, Ca²⁺ signaling disruption | Motor cortex, peripheral nerves | Motor neuropathy, encephalopathy |
| Cisplatin/Vinca alkaloids | Mitochondrial ROS, axonal oxidative damage | Peripheral neurons, cochlea | Sensorimotor neuropathy, ototoxicity |
| HIV/ARV drugs | NMDA activation → Ca²⁺ → nNOS → ONOO⁻ | Basal ganglia, white matter | HAND, HIV encephalopathy |
- Bradley and Daroff's Neurology in Clinical Practice - Mechanisms of Cell Loss, Lead
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry - Stimulant Use Disorders, Neurotoxicity
- Goldman-Cecil Medicine - Alcohol Dementia; Manganese Parkinsonism
- Tietz Textbook of Laboratory Medicine, 7th Ed. - Manganese Toxicokinetics
- Harrison's Principles of Internal Medicine 22E (2025) - Chemotherapy Neurologic Dysfunction; HIV Neuropathogenesis
- Ganong's Review of Medical Physiology - SOD and free radicals in neurodegeneration
Find recent PubMed papers on novel biomarkers for drug-induced oxidative neuronal injury
"oxidative stress" AND "biomarkers" AND "neurotoxicity"
"neuronal injury" AND "biomarkers" AND "oxidative damage" AND drug
"neurofilament light chain" OR "NfL" AND "oxidative stress" AND "drug-induced"
PMID: 38986832
PMID: 40253933
PMID: 38852866
"neurofilament" AND "drug-induced" AND "neurotoxicity" AND "biomarker"
"8-OHdG" OR "isoprostane" OR "4-hydroxynonenal" AND "neurotoxicity" AND "biomarker"
PMID: 38292901
PMID: 39551123
PMID: 41726560
"GFAP" AND "NfL" AND "neurotoxicity" AND blood
"oxidative stress biomarkers" AND "chemotherapy" AND "neurotoxicity"
PMID: 37933726
PMID: 39831665
PMID: 40507935
"metabolomics" OR "proteomics" AND "oxidative stress" AND "drug-induced neurotoxicity"
Recent PubMed Papers: Novel Biomarkers for Drug-Induced Oxidative Neuronal Injury
Category 1: Structural Neuroaxonal Biomarkers (Blood/CSF)
NfL, NSE, Tau, and GFAP for Compound-Induced NS Injury (2023)
- Neurofilament light chain (NfL) was the top performer for detecting both CNS and PNS injury in plasma (AUC 0.97-0.99) - the highest sensitivity and specificity of all markers tested
- Tau in CSF correlated best with CNS injury (AUC 0.97) but not PNS
- NSE and GFAP were suitable for CNS injury monitoring but with lesser sensitivity than NfL
- Combining NfL (plasma) + Tau/NSE (CSF) allows localization of injury to CNS vs. PNS
- Results support cross-species translation for clinical drug safety monitoring
NfL for Chemotherapy-Induced Peripheral Neurotoxicity (2025)
- Plasma NfL was the most sensitive indicator of PNS toxicity, specifically detecting moderate dorsal root ganglion (DRG) degeneration - even when histopathology was minimal
- NF-H (neurofilament heavy chain), Tau, NSE, VEGFA, and GFAP were also measured; none matched NfL's sensitivity for peripheral injury
- A combined functional assessment + NfL biomarker approach outperformed histopathology alone
- Recommends NfL as the go-to biomarker for chemotherapy-induced peripheral neuropathy (CIPN) monitoring
NfL and GFAP for ICI-Induced Neurologic irAEs (2025)
- NfL was significantly elevated in peripheral neurologic irAEs (PNirAEs) vs. neuromuscular irAEs - making it a subtype differentiator
- GFAP was highest in CNS irAEs (CNSirAEs) - reflecting astrocytic injury specifically in central lesions
- Both markers correlated with symptom severity (CTCAE grading) and NfL elevation predicted worse outcomes (p = 0.0199)
- Tested using ultrasensitive Simoa (Single Molecule Array) technology - enabling detection at pg/mL concentrations
NfL and GFAP in Isolated Limb Perfusion (2024)
- NfL and Tau were significantly elevated in the treated extremity versus systemic circulation at the end of ILP (NfL: 17 vs 6 ng/L, p < 0.01)
- Systemic NfL and GFAP remained elevated at day 3 and day 30 post-ILP
- Simoa technology was essential for detection at this sensitivity level
- No significant correlation with regional clinical toxicity grading - suggesting subclinical injury that conventional grading misses
Category 2: Oxidative Stress-Specific Biomarkers (Tissue/Immunohistochemistry)
Multi-Biomarker Oxidative Stress Panel for Cytarabine Neurotoxicity (2026)
| Biomarker | Change with Cytarabine | Notes |
|---|---|---|
| MDA (malondialdehyde) | ↑ significantly | Lipid peroxidation end-product |
| GST (glutathione-S-transferase) | ↑ | Compensatory antioxidant enzyme |
| CAT (catalase) | ↓ | Antioxidant defense depleted |
| GSH-Px (glutathione peroxidase) | ↓ | Key ROS scavenger depleted |
| 8-OHdG (8-hydroxydeoxyguanosine) | ↑ (immunohistochemistry) | DNA oxidative damage marker |
| Bax | ↑ | Pro-apoptotic, downstream of OS |
| GPX4 | ↓ | Ferroptosis-relevant lipid peroxidase |
| Bcl-2 | ↓ | Anti-apoptotic, suppressed |
Category 3: Heavy Metal/Environmental Neurotoxin Biomarkers
Methylmercury Neurotoxicity Biomarkers - Systematic Review (2024)
- Antioxidant enzymes (SOD, catalase, GPx) and oxidative stress markers are consistently the most sensitive to MeHg exposure in both in vitro and in vivo models
- Key biomarker categories: oxidative stress markers, neurotransmitter levels + receptor densities, synaptic proteins, proinflammatory markers (consistently overexpressed), DNA methylation (epigenetic marks)
- Proinflammatory biomarkers are uniformly elevated across all MeHg-exposed models
- Apoptotic pathway markers (caspase-3, Bax/Bcl-2 ratio) provide mechanistic confirmation
Mercury - Transcriptomics/Proteomics/Metabolomics "Omics" Biomarkers (2024)
- Transcriptomics: Gene expression changes in oxidative stress pathways (Nrf2/ARE target genes, heat shock proteins)
- Proteomics: Thiol-modified proteins, carbonylated proteins, altered cytoskeletal proteins (tubulin, neurofilaments)
- Metabolomics: Altered redox metabolites, disrupted glutathione metabolism profiles
- Emphasis on thiol/selenol-protein interactions as specific molecular signatures of mercury exposure
- Calcium homeostasis disruption as an early upstream biomarker
Organophosphate (OP) Biomarker Framework (2025)
- Beyond acetylcholinesterase (AChE): Highlights that AChE alone is insufficient as a biomarker for chronic or developmental neurotoxicity
- Non-cholinergic biomarkers prioritized:
- Neuroinflammation markers (cytokines, GFAP)
- Mitochondrial dysfunction markers (complex I/II activity, ATP levels)
- Oxidative stress markers (GSH/GSSG ratio, lipid peroxidation, 8-OHdG)
- Epigenetic modifications (DNA methylation changes in neuronal genes)
- Promotes non-invasive biomarkers (blood, urine) that correlate with behavioral and neuropathological outcomes
- Proposes a regulatory-grade biomarker ranking framework
Long-term Toxic Oil Syndrome - Blood Biomarkers Decades Later (2025)
- NfL was slightly elevated in TOS patients (p = 0.025); no significant differences in pTau217 or GFAP
- Age was the strongest predictor of all biomarker levels (especially GFAP and pTau217)
- Female sex independently associated with higher GFAP
- Suggests current blood biomarker panels may miss subtle or compartmentalized chronic neurotoxic processes
- Calls for serial biomarker assessments + oxidative stress markers + advanced neuroimaging in longitudinal studies
Summary Table: Novel Biomarkers by Type and Application
| Biomarker | Class | Specimen | Drug/Toxin Application | Key Evidence |
|---|---|---|---|---|
| NfL (neurofilament light chain) | Structural/axonal | Blood/plasma | Chemotherapy (oxaliplatin, cisplatin, paclitaxel), ICI, ILP, metals | PMIDs: 38292901, 39551123, 37933726, 39831665 |
| GFAP (glial fibrillary acidic protein) | Glial/astrocytic | Blood/plasma | CNS drug-induced irAEs, ILP, TOS | PMIDs: 37933726, 39831665, 40507935 |
| Tau / pTau217 | Microtubule/axonal | Blood/CSF | CNS injury, chronic toxin exposure | PMIDs: 38292901, 40507935 |
| NSE (neuron-specific enolase) | Neuronal cytoplasm | Blood/CSF | CNS injury monitoring | PMID: 38292901 |
| MDA (malondialdehyde) | Lipid peroxidation | Tissue/serum | Cytarabine, metals | PMID: 41726560 |
| 8-OHdG | DNA oxidation | Tissue/urine | Cytarabine, UV, metals | PMID: 41726560 |
| GSH/GSSG ratio | Antioxidant depletion | Blood/tissue | OPs, metals, chemotherapy | PMID: 40253933 |
| CAT, GSH-Px, SOD | Antioxidant enzymes | Blood/tissue | MeHg, cytarabine, general | PMIDs: 38986832, 41726560 |
| GPX4 | Ferroptosis/lipid peroxide | Tissue (IHC) | Cytarabine | PMID: 41726560 |
| Multi-omics panel (transcriptomics/proteomics/metabolomics) | Molecular signatures | Tissue/blood | Mercury, OPs | PMIDs: 38852866, 40253933 |
| Epigenetic markers (DNA methylation) | Epigenetic | Blood | MeHg, OPs | PMIDs: 38986832, 40253933 |
Key Themes and Future Directions
-
NfL as the leading candidate for a universal, blood-based drug-induced neuronal injury biomarker - sensitive to both CNS and PNS damage, measurable non-invasively via ultrasensitive Simoa technology
-
CNS vs. PNS distinction can be made by combining NfL (peripheral axons) + GFAP (central astrocytes) + Tau/NSE (CSF, central origin)
-
Oxidative stress-specific markers (MDA, 8-OHdG, GSH-Px, CAT, GPX4) remain important for mechanistic confirmation and tissue-level characterization, though less suited for non-invasive monitoring
-
Multi-omics approaches (transcriptomics + proteomics + metabolomics) are emerging as powerful discovery tools, especially for identifying drug-specific molecular fingerprints (e.g., thiol-modified proteins for mercury)
-
Epigenetic biomarkers (DNA methylation at neuronal gene loci) offer a window into delayed and developmental neurotoxicity that acute-phase markers may miss
-
Regulatory-grade standardization of biomarker frameworks (as proposed for OPs) is an active area - bridging preclinical animal data to clinical trial safety monitoring
Search for clinical protocols using these biomarkers in ongoing drug trials
"neurofilament light" AND "clinical trial" AND "neurotoxicity" AND "safety biomarker"
"GFAP" AND "NfL" AND "chemotherapy" AND "neuropathy" AND "monitoring"
ClinicalTrials.gov NfL GFAP biomarker drug-induced neurotoxicity ongoing trials 2024 2025
https://link.springer.com/article/10.1007/s00415-025-13246-2
"neurofilament" AND "CAR-T" AND "neurotoxicity" AND "biomarker"
"neurofilament light" AND "cisplatin" OR "oxaliplatin" AND "clinical" AND "biomarker"
PMID: 39317455
PMID: 40765152
PMID: 41553539
ClinicalTrials.gov neurofilament light chain NfL neurotoxicity safety endpoint drug trial protocol 2024 2025
https://www.frontiersin.org/journals/neuroscience/articles/1…
"neurofilament" AND "gene therapy" AND "dorsal root ganglia" AND "toxicity" AND "biomarker"
Clinical Protocols Using Oxidative Neuronal Injury Biomarkers in Ongoing Drug Trials
1. Phase 1 First-in-Human Trials - Establishing Reference Thresholds
Serum NfL as a Safety Sentinel in Phase 1 (2025)
- Cohort: 270 normal healthy volunteers (NHVs) in Phase 1 trials (cross-sectional) + 80 NHVs with longitudinal sampling over 2-4 weeks
- Key protocol output: NfL 1.64-fold change from baseline = the ULN threshold for detecting drug-induced nervous system (NS) injury in Phase 1 settings
- NfL and GFAP showed age-dependence (must be age-adjusted); Tau was age-independent but ~1/3 of samples fell below the lower limit of quantification (LLOQ)
- UCH-L1 (another candidate marker) was mostly undetectable at serum levels - not recommended for Phase 1 use
- Technology used: Quanterix SIMOA (Single Molecule Array) ultrasensitive immunoassay
2. CAR-T Cell Therapy Trials - ICANS Monitoring (Most Active Area)
NfL as Pre-Treatment Risk Stratification Tool for ICANS (2024)
- 28% developed ICANS of any grade; 15.3% grade 2-4
- NfL >75 pg/mL at leukapheresis → OR 4.2 (95% CI 1.2-14.2) for grade 2-4 ICANS
- NfL >58 pg/mL at infusion → OR 4.3 (95% CI 1.3-13.7) for grade 2-4 ICANS
- CD28 domain CAR constructs (vs 4-1BB) were the strongest predictor overall, but NfL was independently significant in multivariate models
- Guide CAR product selection (CD28 vs. 4-1BB constructs) based on individual neurotoxicity risk
- Initiate prophylactic corticosteroid protocols for high-NfL patients
- Flag patients for enhanced post-infusion neurological monitoring
Severity-Graded sNfL Protocol Post-CAR-T Infusion (2025)
- Baseline NfL was similarly elevated in both ICANS and non-ICANS groups (pre-existing neuroaxonal stress from prior chemo)
- Day 7 sNfL z-score ≥ 2.14 optimally differentiated moderate-severe ICANS (grade ≥2) from mild/no ICANS (p = 0.004)
- Day 7 monitoring window is the critical protocol timepoint - captures early neuroaxonal injury before clinical deterioration solidifies
GFAP + NfL + Endothelial Dysfunction Panel (2026)
- Baseline GFAP and NfL both significantly associated with ICANS development AND corticosteroid requirement
- Day 7 elevated NfL correlated with DIC, prolonged clotting time, and CRP - suggesting a systemic coagulopathy-neurotoxicity link
- GFAP elevation linked to BBB disruption; NfL to axonal injury - the two markers provide complementary, mechanistically distinct information
| Biomarker | Purpose |
|---|---|
| NfL (baseline) | Pre-existing neuroaxonal integrity, ICANS risk |
| GFAP (baseline) | BBB integrity, CNS ICANS risk |
| mEASIX score | Endothelial dysfunction risk |
| NfL + GFAP (day 7) | Severity grading, DIC/coagulopathy overlap |
3. ALS (Amyotrophic Lateral Sclerosis) Trials - Pharmacodynamic Monitoring
| Trial Name | Drug/Intervention | NfL/pNFH Role in Protocol |
|---|---|---|
| RESCUE-ALS | AMX0035 (sodium phenylbutyrate + ursodiol) | NfL as surrogate neuronal injury endpoint, measured longitudinally |
| CENTAUR | AMX0035 | NFL + pNFH as secondary endpoints; correlated with functional decline (ALSFRS-R) |
| MND-SMART | Multiple arms (multiple drugs) | NFL + pNFH as pharmacodynamic secondary endpoints |
| Lighthouse-II | Adaptive design trial | NfL used for adaptive interim analysis - triggers real-time protocol adjustments (sample size, dose arm reallocation) |
| Verdiperstat trial | Myeloperoxidase inhibitor | CSF TDP-43 measured alongside NfL to monitor target engagement |
4. Immune Checkpoint Inhibitor (ICI) Trials - neurologic irAE Monitoring
- Measure NfL + GFAP: before ICI initiation (baseline), then at each treatment cycle, and at symptom onset
- NfL elevation → peripheral neurologic irAE (PNirAE: neuropathy, radiculopathy) - prompts neurology referral + EMG/NCS workup
- GFAP elevation → CNS irAE (encephalitis, meningitis) - prompts MRI brain + LP
- Combined NfL + GFAP elevation + severity grade → predicts outcome (elevated NfL = worse prognosis at p = 0.0199)
5. AAV Gene Therapy Trials - Dorsal Root Ganglia Safety Monitoring
- Recombinant AAV gene therapy trials (rat and non-human primate models → now translating to human Phase 1)
- High-dose AAV9 and other serotypes used for spinal muscular atrophy (SMA), Duchenne muscular dystrophy, and other neurological conditions
6. IMI NeuroDeRisk / TransBioLine Consortium Framework
- Validated NfL, GFAP, NSE, and Tau across 15 rat in vivo studies and multiple human Phase 1 cohorts
- Proposed a tiered biomarker protocol:
- Tier 1 (plasma NfL): First-line, non-invasive screen for any CNS/PNS injury
- Tier 2 (plasma GFAP + NSE): CNS-specific confirmation
- Tier 3 (CSF Tau): CNS injury localization and severity quantification
- This framework is being adopted by pharmaceutical companies for preclinical-to-clinical safety translation in new drug applications (NDAs/INDs)
7. Oxidative Stress Biomarkers in Trial Protocols
| Biomarker | Context | Trial Application |
|---|---|---|
| 8-OHdG | DNA oxidative damage | AD trials (Phase 2 primary outcome in some oxidative stress-targeted trials - PMID: 41716297) |
| MDA / isoprostanes | Lipid peroxidation | Neuroprotectant drug trials (e.g., antioxidant co-treatment studies with chemotherapy) |
| GSH/GSSG ratio | Redox balance | Organophosphate exposure studies; proposed for pesticide-worker biomonitoring |
| Nrf2 pathway genes | Transcriptomic | Emerging in multi-omics sub-studies of neurodegenerative disease trials |
Summary: Where Each Biomarker is in the Trial Lifecycle
| Biomarker | Trial Readiness | Active Trial Settings | Protocol Role |
|---|---|---|---|
| NfL (serum/plasma) | Most advanced - Phase 1 thresholds established | CAR-T, ALS trials, Phase 1 FIH, AAV gene therapy, ICI | Safety stopping rule, secondary endpoint, adaptive design trigger |
| GFAP (serum) | Clinically deployed in several studies | CAR-T, ICI, isolated limb perfusion | CNS irAE detection, BBB integrity monitoring |
| Tau (serum/CSF) | Validated preclinically, selective clinical use | Phase 1 FIH, ALS, regional chemotherapy | CNS localization, severity grading |
| NSE | Established, less sensitive than NfL | Phase 1 panels | CNS injury confirmation tier 2 |
| 8-OHdG | Mechanistic sub-studies | AD trials, neuroprotectant studies | Oxidative stress primary/secondary endpoint |
| MDA, GSH-Px, CAT | Preclinical/translational | Chemotherapy neuroprotection studies | Mechanistic biomarker, tissue-level only |