Cardiac temponads
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cardiac tamponade" diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I have comprehensive information now. Let me compile the full, detailed answer on cardiac tamponade.
Cardiac Tamponade
Cardiac tamponade is a life-threatening condition where fluid accumulation within the pericardial sac compresses the heart chambers, impairs diastolic filling, and reduces cardiac output. It represents a medical emergency requiring prompt recognition and drainage.
Definition
Tamponade is "a constellation of hemodynamic derangements secondary to elevated intrapericardial pressure and resultant compression of cardiac chambers." The condition exists on a physiologic continuum - it is not simply the presence of a pericardial effusion, but rather the hemodynamic consequence of that effusion.
- Fuster and Hurst's The Heart, 15th Edition
- ROSEN's Emergency Medicine
Etiology
| Category | Examples | Frequency |
|---|---|---|
| Malignancy | Lung, breast, lymphoma, GI cancers | 32% |
| Infection | Staph, Strep, TB, HIV | 24% |
| Idiopathic | Unknown | 16% |
| Iatrogenic | Post-cardiac cath, post-cardiac surgery, anticoagulants | 15% |
| Post-MI | Cardiac wall rupture (44% of post-MI cases) | 7% |
| Uremic | Pericarditis from renal failure | 4% |
- ROSEN's Emergency Medicine
Pathophysiology
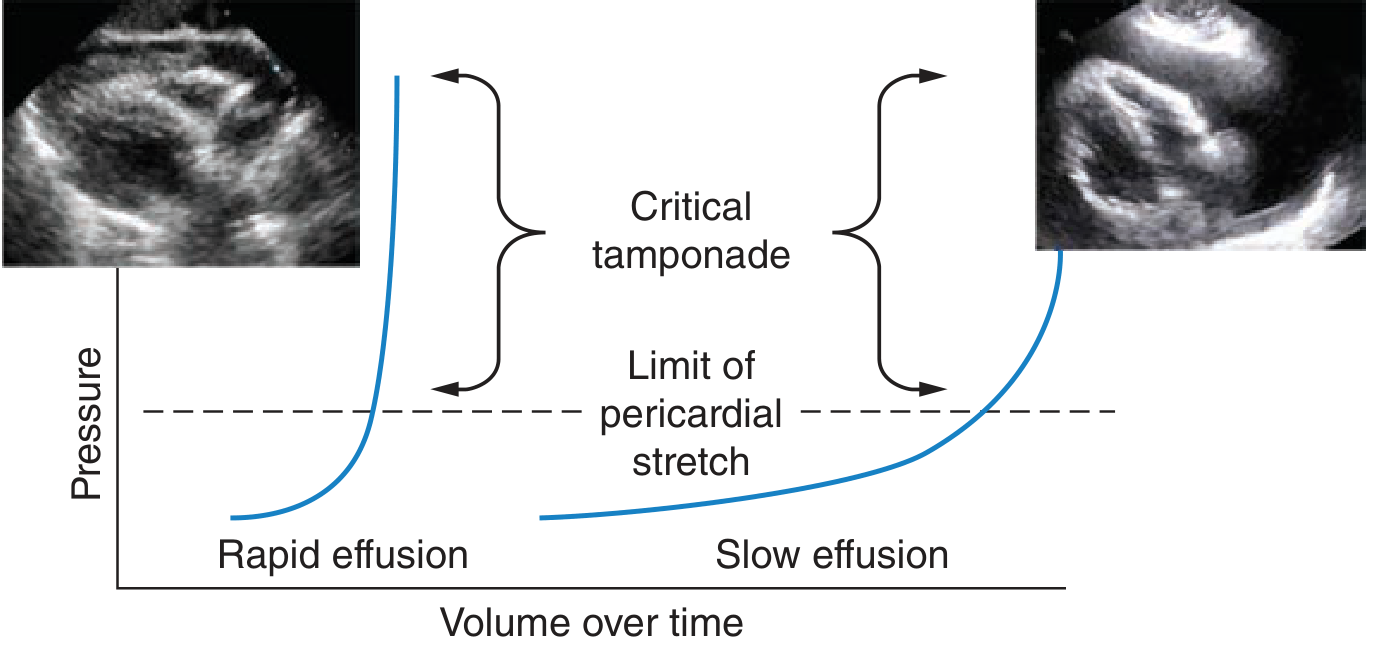
The Key Concept: Rate of Accumulation > Volume
The pericardial pressure-volume relationship is non-linear. In rapid effusion (e.g., trauma, aortic dissection), as little as 150 mL of blood can cause tamponade because the stiff pericardium cannot accommodate sudden volume. In slow, chronic effusion, the pericardium stretches and can accommodate liters of fluid with minimal hemodynamic effect.
Three-Stage Mechanism (Rosen's):
- Fluid fills the recesses of the parietal pericardium
- Fluid accumulates faster than the pericardium can stretch
- Accumulation exceeds the body's compensatory ability to increase right ventricular filling pressure
Hemodynamic Cascade:
-
Rising intrapericardial pressure reduces transmural filling pressure (intracavitary minus intrapericardial pressure)
-
Diastolic filling pressures become elevated and equalized across all chambers
-
Ventricular interdependence: total intrapericardial volume is fixed, so when RV volume increases (inspiration), LV volume decreases - this is the origin of pulsus paradoxus
-
Tachycardia and peripheral vasoconstriction initially compensate
-
Eventually: stroke volume falls, cardiac output drops, hypotension, shock, and death
-
Fuster and Hurst's The Heart, 15th Edition
Clinical Features
Beck's Triad
The classic triad is:
- Hypotension
- Distended neck veins (elevated JVP)
- Muffled/distant heart sounds
Important caveat: Beck's triad is present in less than half of patients with tamponade. Its absence does not exclude the diagnosis.
Features by Frequency (more common)
- Tachycardia (HR >100 bpm) - secondary to adrenergic stimulation, early compensatory mechanism
- Pulsus paradoxus - inspiratory drop in systolic BP >10 mmHg (in severe tamponade, may become undetectable as BP/stroke volume fall too low)
- Elevated JVP - with absence or blunting of the y descent (impaired diastolic filling)
- Dyspnea - most common symptom
- Other symptoms: chest pain, cough, fatigue
Important Physical Exam Points:
-
No pulmonary edema - lungs are clear on auscultation (unique to tamponade, distinguishes it from heart failure)
-
No S3 - early diastolic filling is impaired; an S3 suggests an alternative diagnosis
-
JVP will fall with restoration of y descent after pericardiocentesis; persistent elevation suggests effusive-constrictive pericarditis
-
Fuster and Hurst's The Heart, 15th Edition
Differential Diagnosis
Cardiac tamponade must be distinguished from:
- Tension pneumothorax
- Massive pulmonary embolism (obstructive shock)
- Right ventricular infarction
- Acute decompensated heart failure
- Dilated cardiomyopathy
- Superior vena cava syndrome
- Simple large pericardial effusion (without tamponade physiology)
Diagnostic Investigations
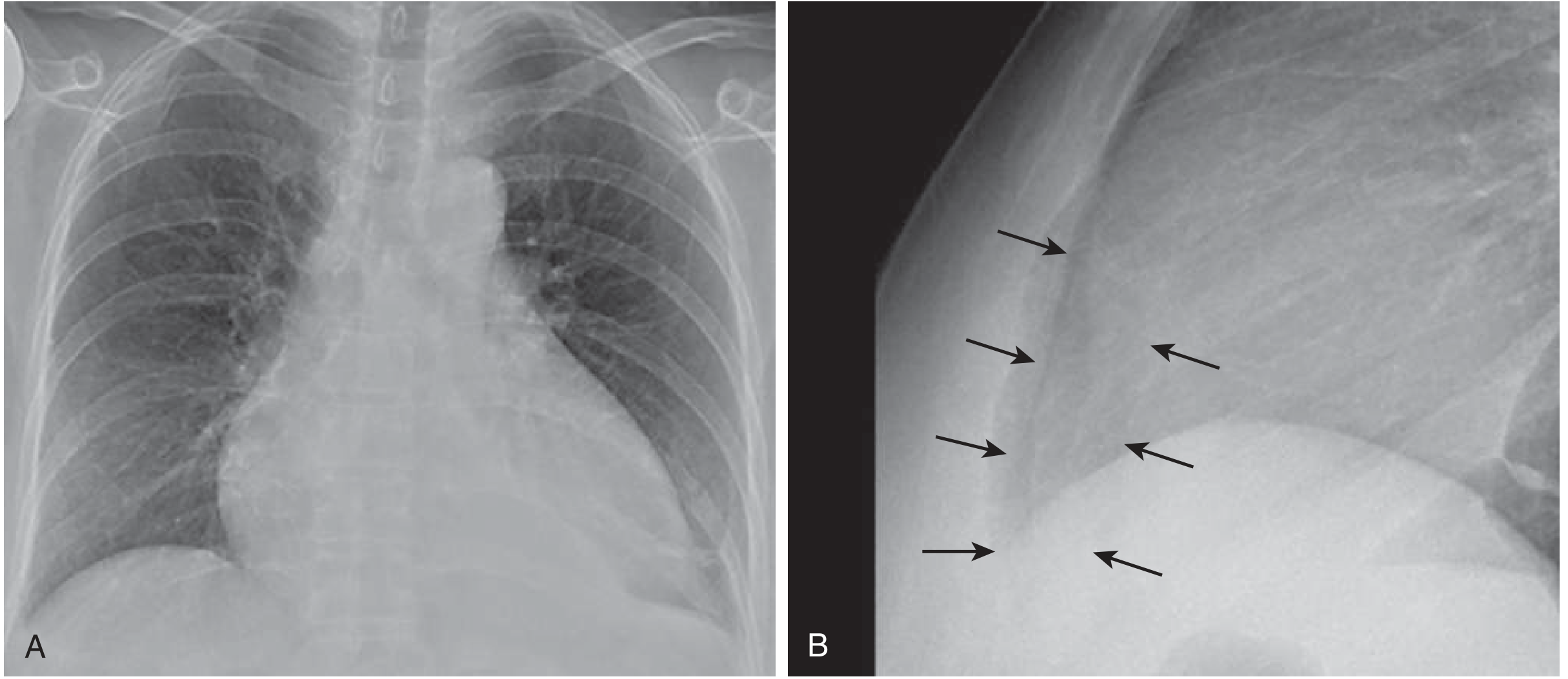
1. Chest X-Ray
Cardiomegaly is present only if >250 mL of pericardial fluid has accumulated. The classic finding is an enlarged cardiac silhouette with a "water bottle" or "flask" configuration. The lateral view may show separation between the pericardial and epicardial fat stripes.
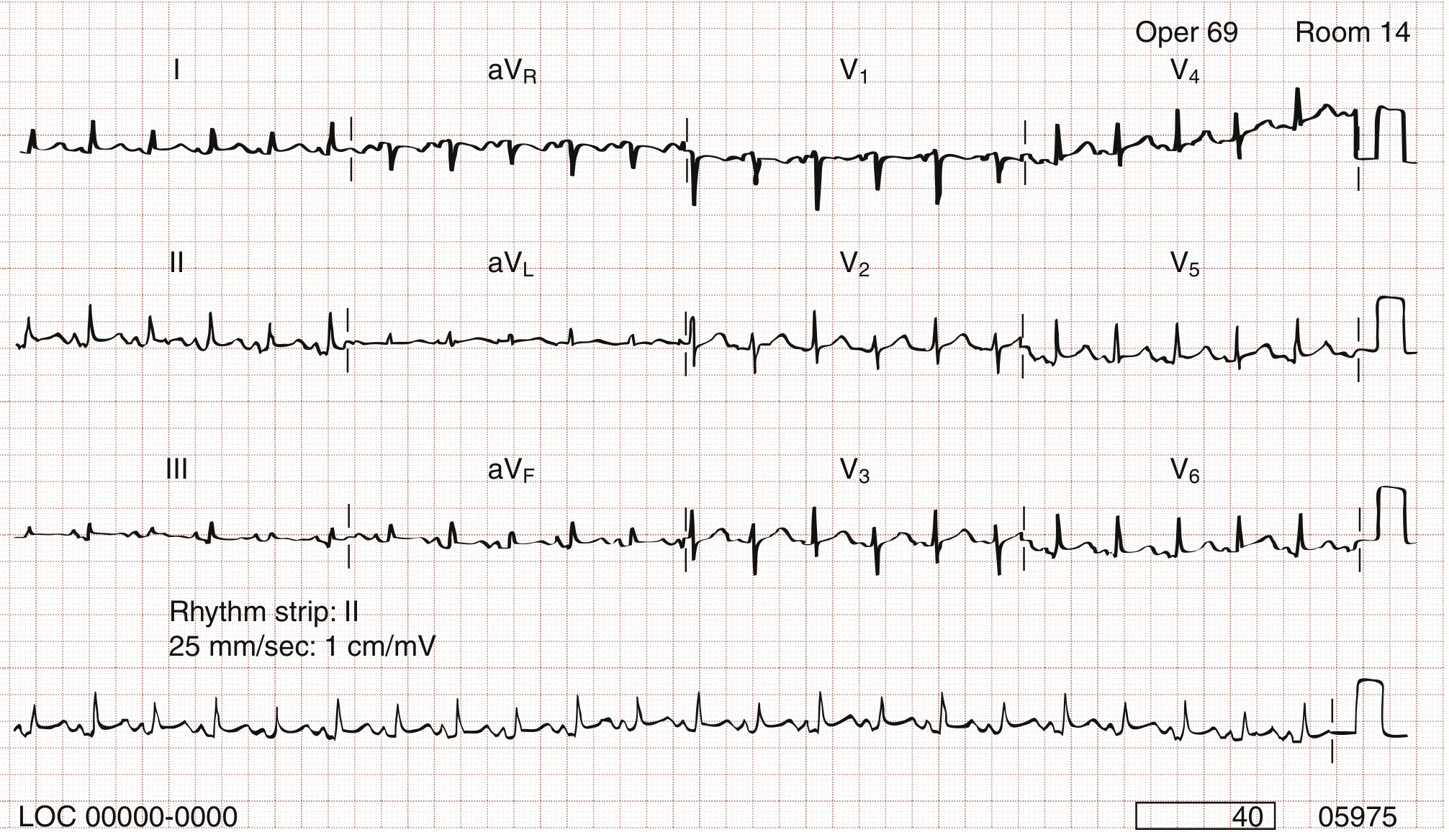
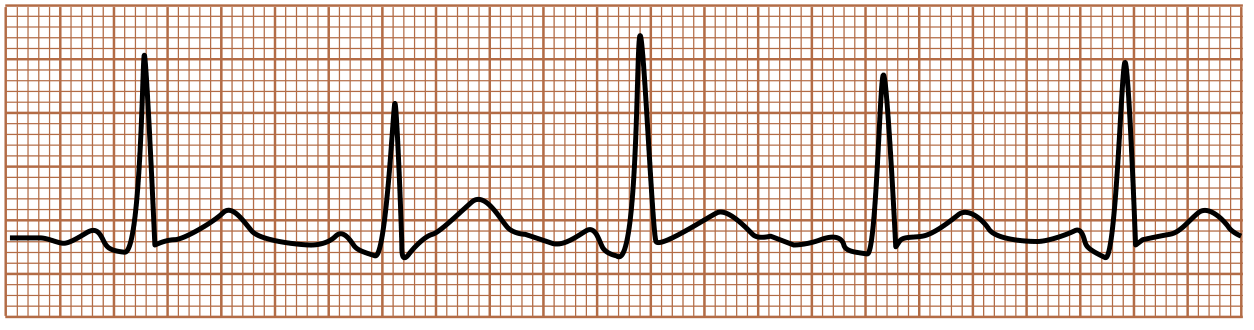
2. ECG
- Low voltage complexes
- Electrical alternans - alternating QRS axis/amplitude beat-to-beat (the heart swings within the effusion). Helpful but uncommon.
- Sinus tachycardia - almost universal
3. Echocardiography (Gold Standard)
Point-of-care ultrasound (POCUS) is the primary diagnostic modality. Key findings:
- Pericardial effusion visualized
- Diastolic collapse of the right atrium (earliest sign) - RA free wall inversion persisting >1/3 of the cardiac cycle
- Diastolic collapse of the right ventricle - high specificity
- Abnormal respirophasic variation in mitral and tricuspid inflow velocities (>25% variation on Doppler)
- IVC plethora - dilated, non-collapsing inferior vena cava
- Hepatic venous flow: marked reduction in diastolic forward flow with expiration, with increased atrial reversal
4. Cardiac Catheterization (Invasive Hemodynamics)
Rarely needed for initial diagnosis, but if Swan-Ganz catheter is in place:
- Elevation and equalization of right- and left-sided filling pressures (RA, RV diastolic, PCW all equalizing)
- Falling cardiac index
- Contour of right atrial pressure tracing: absent or blunted y descent
Special Variants
Low-Pressure Tamponade
Small effusion in a hypovolemic patient. Hemodynamic compromise occurs despite only minimally elevated intrapericardial pressure. Clinical signs of elevated CVP are absent. Careful volume replacement may help; echocardiography shows chamber collapse.
Regional (Loculated) Tamponade
Common post-cardiac surgery - hematoma collects in loculated pericardial spaces causing selective chamber compression (usually behind the right atrium). Transthoracic echo is often inadequate; transesophageal echocardiography (TEE) is the modality of choice.
- Fuster and Hurst's The Heart, 15th Edition
Management
Immediate Stabilization
- IV fluids - to increase right-sided filling pressure (only if patient is volume-depleted; has limited and transient benefit)
- Inotropic agents are usually ineffective because intense endogenous adrenergic stimulation is already present
- Avoid mechanical ventilation if possible - positive intrathoracic pressure from ventilation further impairs cardiac filling and can cause sudden cardiovascular collapse
- Avoid diuretics and vasodilators - dangerous
Definitive Treatment: Pericardial Drainage
Echocardiographic-guided pericardiocentesis is the treatment of choice:
- Indicated when ≥1 cm of fluid is seen anterior to the mid-right ventricular free wall throughout diastole
- Ideal entry site defined by echo as the shortest path from skin to pericardial fluid without intervening structures (usually near the apex or subcostal approach)
- Insert needle, enter pericardial space, drain via catheter
- An indwelling catheter left for continued drainage minimizes risk of recurrence
Pericardial fluid analysis should include: LDH, protein, cell count, cytology, PCR for TB, culture for bacteria and TB.
When Surgical Drainage is Preferred
- Organized, multiloculated, or focal effusions <1 cm
- Pericardial tissue needed for histologic diagnosis
- Recurrent effusions (especially malignant) - surgical pericardial window creation to allow drainage into the pleural space
- Bacterial (purulent) pericarditis
Hemodynamically Significant Small Effusions (<1 cm)
Requires surgical drainage (limited thoracotomy/mediastinoscopy with pericardial window creation) rather than percutaneous pericardiocentesis.
- Goldman-Cecil Medicine, ROSEN's Emergency Medicine, Fuster and Hurst's The Heart
Prognosis
- In-hospital mortality with tamponade and pericardiocentesis: <10%
- Subsequent mortality: ~75% if malignant effusion
- Subsequent annual mortality: 3-5% for non-malignant causes
Long-term prognosis is primarily determined by the underlying etiology.
Summary Table
| Feature | Finding |
|---|---|
| Classic triad | Hypotension + elevated JVP + muffled heart sounds (present in <50%) |
| Most common symptom | Dyspnea |
| ECG hallmark | Electrical alternans + low voltage |
| CXR finding | Water bottle heart (>250 mL needed) |
| Echo - earliest sign | RA diastolic collapse |
| High specificity echo sign | RV diastolic collapse |
| JVP waveform | Absent y descent |
| Unique feature | Clear lungs (no pulmonary edema), no S3 |
| Pulsus paradoxus | >10 mmHg inspiratory drop in SBP |
| Hemodynamics | Equalization of diastolic pressures |
| Treatment of choice | Echo-guided pericardiocentesis |
| Avoid | Mechanical ventilation, diuretics, vasodilators |
Sources: Fuster and Hurst's The Heart, 15th Ed | Goldman-Cecil Medicine | ROSEN's Emergency Medicine | Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.