Hii help me understand pain management in detail with all the conversation factor calculation and all
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
opioid equianalgesic conversion table morphine equivalents 2024 clinical guide
I now have comprehensive data from multiple authoritative textbooks. Let me compile the full, detailed response:
Pain Management — A Comprehensive Guide
1. Understanding Pain: Types & Classification
Pain is broadly classified into three types based on mechanism:
| Type | Mechanism | Example Conditions |
|---|---|---|
| Nociceptive | Activation of nociceptors by tissue damage | Post-surgical pain, osteoarthritis, fractures |
| Neuropathic | Damage/dysfunction of the nervous system | Diabetic neuropathy, post-herpetic neuralgia, cancer nerve invasion |
| Nociplastic | Altered nociception without clear tissue/nerve damage | Fibromyalgia, central sensitization |
Most clinical pain — including cancer pain — is multifactorial, combining nociceptive and neuropathic components, which is why multimodal analgesia is the modern standard.
2. Pain Assessment Tools
Before any treatment, quantify pain objectively:
| Scale | Description | When to Use |
|---|---|---|
| NRS (Numeric Rating Scale) | 0–10, patient self-reports | Most clinical settings; standard for adults |
| VAS (Visual Analog Scale) | 100 mm line; patient marks intensity | Research, acute/chronic pain |
| Wong-Baker FACES | Cartoon faces 0–10 | Children, cognitively impaired |
| FLACC | Observer scale: Face, Legs, Activity, Cry, Consolability | Non-verbal/unconscious patients |
The NRS and VAS are the most widely used. The VAS is more common in research settings.
3. The WHO Analgesic Ladder
The World Health Organization developed a three-step analgesic ladder for systematic pain escalation, originally for cancer pain but now widely applied:
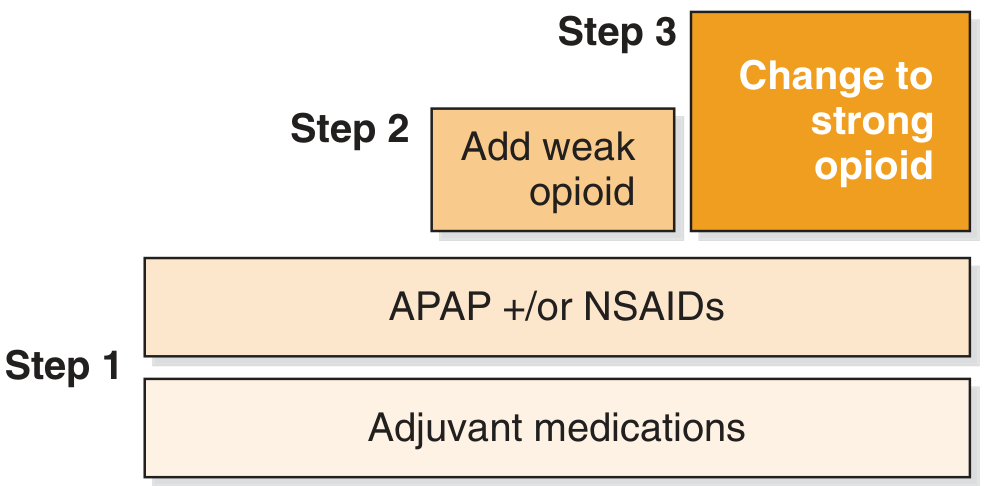
| Step | Pain Level | Medications |
|---|---|---|
| Step 1 | Mild (NRS 1–3) | Acetaminophen (APAP), NSAIDs + adjuvants |
| Step 2 | Moderate (NRS 4–6) | Weak opioids (tramadol, codeine, hydrocodone) ± APAP/NSAIDs + adjuvants |
| Step 3 | Severe (NRS 7–10) | Strong opioids (morphine, oxycodone, fentanyl, hydromorphone, buprenorphine, methadone) ± adjuvants |
Adjuvant medications (antidepressants, anticonvulsants, corticosteroids) are added at every step as needed.
WHO 5-Point Administration Framework
| Principle | Meaning |
|---|---|
| By mouth | Prefer oral route whenever feasible — effective, cheap, flexible |
| By the clock | Regular scheduled dosing to maintain steady analgesia (not PRN alone) |
| By the ladder | Select drug based on pain severity |
| For the individual | Titrate dose to each patient's needs |
| Attention to detail | Reassess frequently; monitor side effects |
Source: Cummings Otolaryngology; Goldman-Cecil Medicine
4. Pharmacological Agents
A. Step 1 — Nonopioid Analgesics
Acetaminophen (APAP)
- Acts centrally (CNS); no significant anti-inflammatory effect
- First-line for mild pain, fever, multimodal analgesia
- Max daily dose: 4 g/day (2 g/day in liver disease/elderly)
- Lacks GI/cardiovascular/renal risks of NSAIDs
NSAIDs (ibuprofen, naproxen, ketorolac, diclofenac, celecoxib)
- Inhibit COX enzymes → ↓ prostaglandins → peripheral and central antinociception
- Highly effective for inflammatory and bone pain
- Risks: GI ulceration/bleeding, renal toxicity, cardiovascular events, platelet dysfunction
- COX-2 selective agents (celecoxib) reduce GI risk but not renal/cardiovascular risk
- Topical NSAIDs (e.g., diclofenac gel) useful for focal conditions with fewer systemic effects
B. Step 2 — Weak Opioids
| Drug | Mechanism/Notes | Caution |
|---|---|---|
| Tramadol | Weak μ-opioid agonist + SNRI; active metabolite (O-desmethyltramadol) is 700× more potent at μ-receptors | Serotonin syndrome with SSRIs; seizures; false-positive PCP urine screen; CYP2D6 variability |
| Codeine | Prodrug — converted to morphine by CYP2D6; 0.15 MME/mg | 10% of US population are poor metabolizers (no effect); ultra-rapid metabolizers at risk of overdose; high GI side effects |
| Hydrocodone | Semisynthetic, direct-acting; Schedule II | Previously combined with APAP (dose-limited); now available as ER alone |
C. Step 3 — Strong Opioids
| Drug | Initial Adult Dose | Onset | Duration | Notes |
|---|---|---|---|---|
| Morphine | 2–6 mg IV; 10 mg IM/SC; 10–30 mg PO IR | 1–2 min IV; 30 min PO | 3–5 h PO | Gold standard; active metabolite (morphine-6-glucuronide) accumulates in renal failure |
| Hydromorphone | 0.5–2 mg IV; 1–2 mg IM | 5–15 min IV | 2–4 h IV | More euphoria than morphine; 4× more potent than morphine |
| Fentanyl | 50–100 mcg IV; 100 mcg nasal/buccal | <1 min IV | 30–60 min IV; 72 h transdermal | No histamine release; chest wall rigidity with high IV doses (>5 mcg/kg); transdermal for chronic pain |
| Oxycodone | 5–10 mg PO | 10–15 min PO | 3–6 h | CR oxycodone ~2× as potent as CR morphine orally; lower nausea than morphine |
| Methadone | Individualized | Variable | 24–36 h | Complex pharmacokinetics; dose-dependent MME (see table below); QT prolongation risk |
| Buprenorphine | Partial μ-agonist/κ-antagonist | 15 min IM | 6 h IM | Ceiling effect on respiratory depression; useful in OUD |
Oxycodone note: Controlled-release oxycodone 20 mg ≈ CR morphine 45 mg; 40 mg ≈ CR morphine 90 mg.
5. Opioid Conversion & MME Calculations
What is MME?
Morphine Milligram Equivalents (MME) is the standard unit for comparing opioid doses across drugs and routes. Morphine oral = 1 MME/mg.
Formula:
MME = Dose (mg/day) × MME Conversion Factor
Full MME Conversion Table (from CMS/CDC)
| Opioid | MME Conversion Factor |
|---|---|
| Morphine (mg) | 1 |
| Hydrocodone (mg) | 1 |
| Codeine (mg) | 0.15 |
| Tramadol (mg) | 0.1 |
| Tapentadol (mg) | 0.4 |
| Meperidine (mg) | 0.1 |
| Oxycodone (mg) | 1.5 |
| Oxymorphone (mg) | 3 |
| Hydromorphone (mg) | 4 |
| Levorphanol (mg) | 11 |
| Buprenorphine film/tablet (mg) | 30 |
| Buprenorphine patch (mcg/h) | 12.6 |
| Buprenorphine film (mcg) | 0.03 |
| Fentanyl patch (mcg/h) | 7.2 |
| Fentanyl buccal/SL tablets (mcg) | 0.13 |
| Fentanyl nasal spray (mcg) | 0.16 |
| Fentanyl film/oral spray (mcg) | 0.18 |
| Butorphanol (mg) | 7 |
| Pentazocine (mg) | 0.37 |
| Dihydrocodeine (mg) | 0.25 |
| Methadone | Dose-dependent (see below) |
Methadone MME (dose-dependent)
| Daily Methadone Dose | MME Factor |
|---|---|
| 0–20 mg | 4 |
| >20–40 mg | 8 |
| >40–60 mg | 10 |
| >60 mg | 12 |
⚠️ Methadone conversion is particularly complex due to incomplete cross-tolerance. Always reduce the calculated equianalgesic dose by 25–50% when switching TO methadone.
Worked Examples
Example 1: Patient on oxycodone 10 mg PO 4× daily (40 mg/day)
MME = 40 mg × 1.5 = 60 MME/day
Example 2: Patient on transdermal fentanyl 25 mcg/h patch
MME = 25 mcg/h × 7.2 = 180 MME/day
Example 3: Patient on tramadol 50 mg 3× daily (150 mg/day)
MME = 150 × 0.1 = 15 MME/day
Example 4: Patient on codeine 30 mg PO 4× daily (120 mg/day)
MME = 120 × 0.15 = 18 MME/day
6. Equianalgesic Dosing (Between Opioids)
When rotating opioids (switching due to inadequate analgesia or intolerable side effects):
Key Equianalgesic Doses (IV/IM)
| Drug | Parenteral Equianalgesic Dose | Oral Equianalgesic Dose |
|---|---|---|
| Morphine | 10 mg | 30 mg |
| Hydromorphone | 1.5 mg | 7.5 mg |
| Oxycodone | — | 20 mg |
| Fentanyl | 0.1 mg (100 mcg) | — |
| Meperidine | 75–100 mg | 300 mg |
| Codeine | 130 mg | 200 mg |
Opioid Rotation Rules
- Calculate total 24-hour MME of current opioid
- Find equianalgesic dose of new opioid
- Reduce by 25–50% to account for incomplete cross-tolerance
- Provide breakthrough (rescue) dosing = 10–15% of 24-hour scheduled dose, q1–2h PRN
- Reassess frequently and titrate to effect
⚠️ MME tables are approximations only. Wide interpatient variability exists. Always individualize and titrate gradually. CDC guidelines note that MME calculations should only be used from an opioid to morphine — not from morphine to another opioid.
7. Routes of Opioid Administration
| Route | Notes |
|---|---|
| Oral (PO) | Preferred; effective, cheap, flexible |
| IV | Fastest onset; use for acute/severe pain or PCA |
| IM/SC | Slower than IV; painful; avoided when possible |
| Transdermal | For chronic pain (fentanyl, buprenorphine); NOT for acute pain (delayed onset/offset) |
| Transmucosal/Buccal/SL | Fast onset; used for breakthrough cancer pain |
| Neuraxial (epidural/intrathecal) | Superior analgesia; useful in opioid-tolerant patients; risk of respiratory depression |
| Patient-Controlled Analgesia (PCA) | Allows IV self-dosing within set limits; standard for post-op pain |
8. Adjuvant (Co-analgesic) Medications
Used at all steps of the WHO ladder to enhance analgesia and reduce opioid requirements:
For Neuropathic Pain
| Drug Class | Examples | Mechanism | Use |
|---|---|---|---|
| Gabapentinoids | Gabapentin, Pregabalin | Ca²⁺ channel α2δ ligands → ↓ excitatory neurotransmitter release | First-line for neuropathic pain, lancinating type; also used perioperatively |
| TCAs | Amitriptyline, Nortriptyline, Imipramine | ↑ serotonin & norepinephrine; lower doses used vs. antidepressant doses | Neuropathic pain, headaches, insomnia; nortriptyline/imipramine preferred (fewer side effects than amitriptyline) |
| SNRIs | Duloxetine, Venlafaxine | SNRI | Neuropathic pain, fibromyalgia; less efficacious than TCAs but better tolerated |
| Anticonvulsants | Carbamazepine, Oxcarbazepine | Na⁺ channel blockade | Trigeminal neuralgia (carbamazepine = first choice) |
Efficacy hierarchy for neuropathic pain:
TCAs > SNRIs > SSRIs (in terms of analgesic potency) Gabapentin/pregabalin may be superior for lancinating/shooting pain
Other Adjuvants
| Agent | Use |
|---|---|
| Corticosteroids | Bone pain, nerve compression, raised ICP in cancer |
| Bisphosphonates | Bone metastases pain |
| Ketamine (sub-anesthetic) | Refractory neuropathic pain, NMDA antagonism |
| Lidocaine IV | Neuropathic pain, post-op pain |
| Muscle relaxants | Musculoskeletal spasm |
| Antidepressants | Comorbid depression + chronic pain |
9. Opioid Side Effects & Management
| Side Effect | Management |
|---|---|
| Constipation | Prophylactic stimulant laxatives (senna/bisacodyl) — does NOT resolve with tolerance |
| Nausea/Vomiting | Antiemetics PRN; usually improves with tolerance in days |
| Pruritus | Antihistamines; naloxone low-dose; more common with neuraxial route |
| Urinary retention | Bladder scan; catheterization if needed; more common with neuraxial |
| Sedation | Dose reduction; opioid rotation; avoid CNS depressants |
| Respiratory depression | Naloxone 0.4 mg IV (dilute and titrate); highest risk with neuraxial, IV, transmucosal |
10. Special Considerations
Opioid Tolerant Patients (Post-Surgical)
- Replace baseline opioid requirement (50–100% of baseline via IV PCA)
- Add a demand dose to cover incisional pain above baseline
- Maximize adjuvants (NSAIDs, gabapentinoids scheduled)
- Plan early transition to oral regimen
- Never use PRN-only regimen — will trigger withdrawal
- Be prepared to recognize and treat opioid withdrawal
Meperidine (Pethidine) — Largely Avoided
- Removed from WHO essential medicines list (2003)
- Active metabolite normeperidine accumulates → seizures (especially with >48 h use, >600 mg/day, or renal failure)
- Higher delirium risk in elderly; multiple serotonin syndrome interactions
- Avoid in most clinical settings
Codeine — Use with Caution
- ~10% of US population (30% of Asians) = poor CYP2D6 metabolizers → zero analgesia
- Ultra-rapid metabolizers at risk of life-threatening morphine toxicity
- Standard PO dose (30–60 mg) gives little analgesic benefit beyond APAP alone
- Neonatal deaths reported from breastfeeding mothers who are ultra-rapid metabolizers
Methadone — Special Drug
- Very long and unpredictable half-life (up to 150 h)
- Significant risk of QT prolongation → torsades de pointes
- Dose escalation must be slow (every 5–7 days minimum)
- Conversion FROM other opioids to methadone is complex; always reduce by 25–50%
11. Multimodal Analgesia Approach (Modern Standard)
The modern approach replaces unimodal opioid therapy with a multimodal combination to improve analgesia while minimizing opioid use:
MULTIMODAL ANALGESIA =
Acetaminophen (scheduled)
+ NSAIDs/COX-2 inhibitors (scheduled, if no contraindication)
+ Gabapentinoids (if neuropathic component)
+ Regional analgesia (nerve blocks, epidural — where applicable)
+ Low-dose opioids (PRN or scheduled, minimal effective dose)
+ Non-pharmacological (PT, ice/heat, TENS, psychological support)
12. Quick Reference: MME Thresholds
| MME/day | Clinical Significance |
|---|---|
| <50 MME | Lower risk; still requires monitoring |
| 50–90 MME | CDC recommends reassessment of risks/benefits |
| ≥90 MME | High-risk threshold; CDC recommends avoiding or carefully justifying |
| >200 MME | Very high risk; specialist involvement recommended |
Summary Flowchart
Assess Pain (NRS/VAS)
|
Mild (1-3) ─────────── APAP ± NSAID + Adjuvant
|
Moderate (4-6) ─────── Weak Opioid + APAP/NSAID + Adjuvant
|
Severe (7-10) ──────── Strong Opioid ± APAP/NSAID + Adjuvant
|
Calculate MME → Monitor → Titrate → Rotate if needed
Sources:
- Cummings Otolaryngology Head and Neck Surgery (Pain Management, Ch. 14)
- Miller's Anesthesia, 10e (Opioid equianalgesic conversion, Table 77.7)
- Tintinalli's Emergency Medicine (Opioid dosing tables 35-4, 35-5)
- Current Surgical Therapy, 14e (MME Conversion Table 4)
- Goldman-Cecil Medicine (Adjuvant analgesics, neuropathic pain)
- Barash Clinical Anesthesia, 9e (Opioid pharmacokinetics, Table 55-11)
- Goodman & Gilman's Pharmacological Basis of Therapeutics (Opioid dosing routes)
This is a shared conversation. Sign in to Orris to start your own chat.