Imaging in cardiomyopathies for nd radiology theory exam
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the material needed. Let me compile the comprehensive exam answer.
Imaging in Cardiomyopathies
Source: Grainger & Allison's Diagnostic Radiology, Braunwald's Heart Disease
Classification Overview
Cardiomyopathies are classified by phenotype (ESC approach) into:
| Phenotype | Main Types |
|---|---|
| Hypertrophic | HCM, Fabry disease, amyloidosis, athlete's heart |
| Dilated | DCM (ischaemic vs non-ischaemic), myocarditis |
| Restrictive | Amyloidosis, sarcoidosis, haemochromatosis, endomyocardial fibrosis |
| Arrhythmogenic | ARVC/ARVD |
| Unclassified | Takotsubo, LVNC (non-compaction) |
Imaging Modalities: Role Summary
| Modality | Key Roles |
|---|---|
| Chest X-ray | First-line; shows cardiomegaly, pulmonary congestion |
| Echocardiography | Workhorse; structure, function, wall thickness, Doppler |
| Cardiac MRI (CMR) | Gold standard for tissue characterisation; LGE fibrosis mapping |
| Cardiac CT | Wall thickness, coronary anatomy (rule out ischaemia), ARVC |
| Nuclear (MUGA/PET) | LV function, amyloid (pyrophosphate scan) |
1. Hypertrophic Cardiomyopathy (HCM)
Definition: Autosomal dominant sarcomere disease; septal thickness >15 mm in a non-dilated LV, unexplained by other causes.
Chest X-ray
- Often unhelpful in early disease
- Concentric hypertrophy may produce a rounded third left cardiac contour (different from aortic stenosis/hypertension which cause similar but distinguishable appearance)
Echocardiography (Primary Modality)
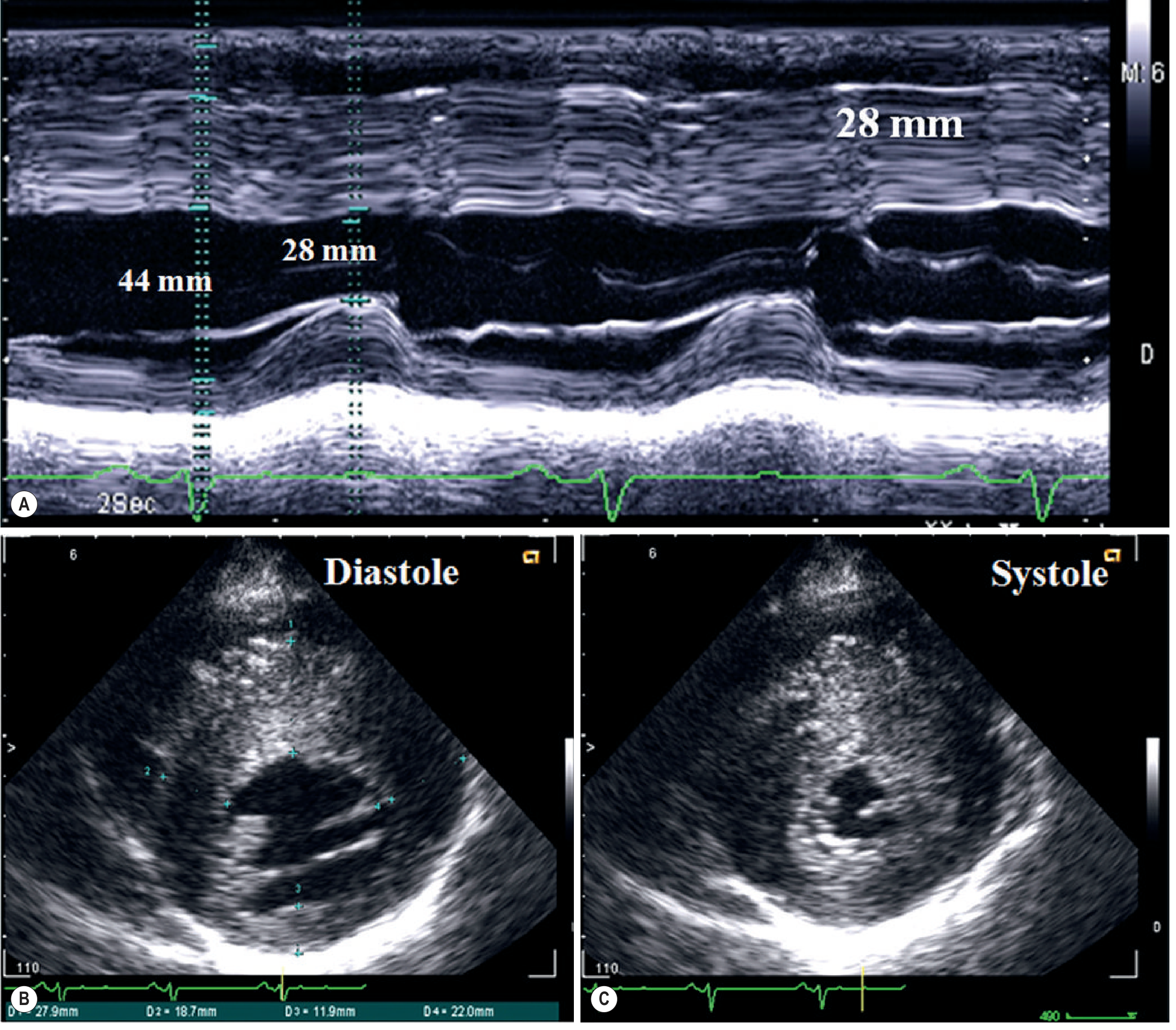
- M-mode: measures IVS and posterior wall thickness; IVS:posterior wall ratio >1.3 is diagnostic
- B-mode: asymmetric septal hypertrophy (ASH); apical/midventricular/mass-like variants
- Doppler: LVOT obstruction in 25% due to systolic anterior motion (SAM) of mitral valve (Venturi effect); rest gradient or provokable gradient; impaired diastolic function (reduced E wave, E/A equalisation)
- Limitation: apical forms near the low-frequency probe, poor acoustic window
Cardiac MRI (Gold Standard for Tissue Characterisation)
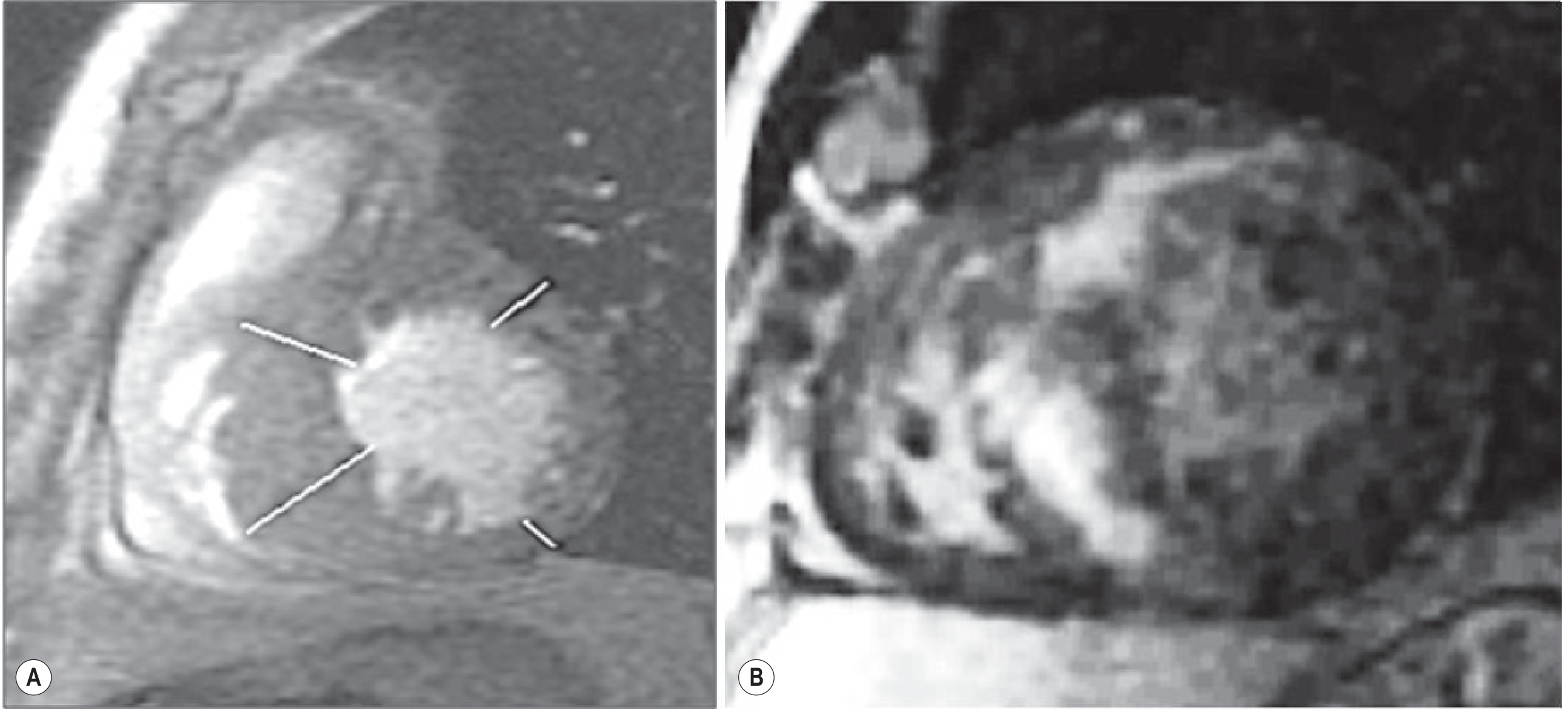
Key MRI features:
- Cine MRI: precise wall thickness measurement; all hypertrophy patterns visible; accurate LV mass quantification; RV involvement quantified
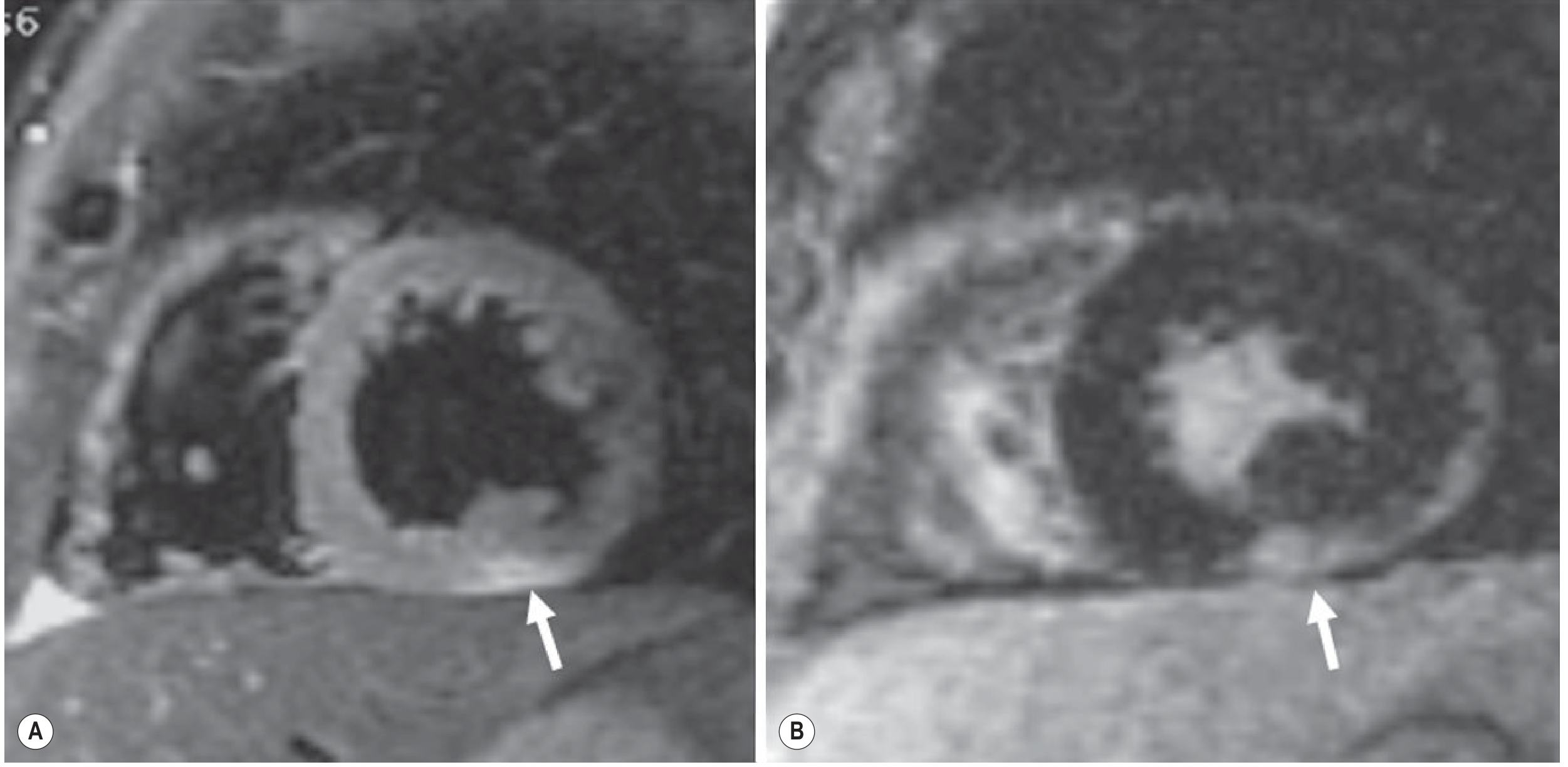
- Late gadolinium enhancement (LGE): PATHOGNOMONIC pattern = intramural fibrosis with selective septal enhancement and relative sparing of the subendocardial layer (distinguishes from MI where enhancement is subendocardial/transmural)
- Also: enhancement at anterior and inferior septal insertion points (RV insertion sites)
- Patchy large intramural foci in severe cases
- Prognostic value of LGE: Fibrosis on MRI predicts ventricular arrhythmias, sudden cardiac death (<40 years), and progression to HF (>40 years)
- T1/T2 mapping: quantitative tissue characterisation; can detect diffuse fibrosis not seen on LGE
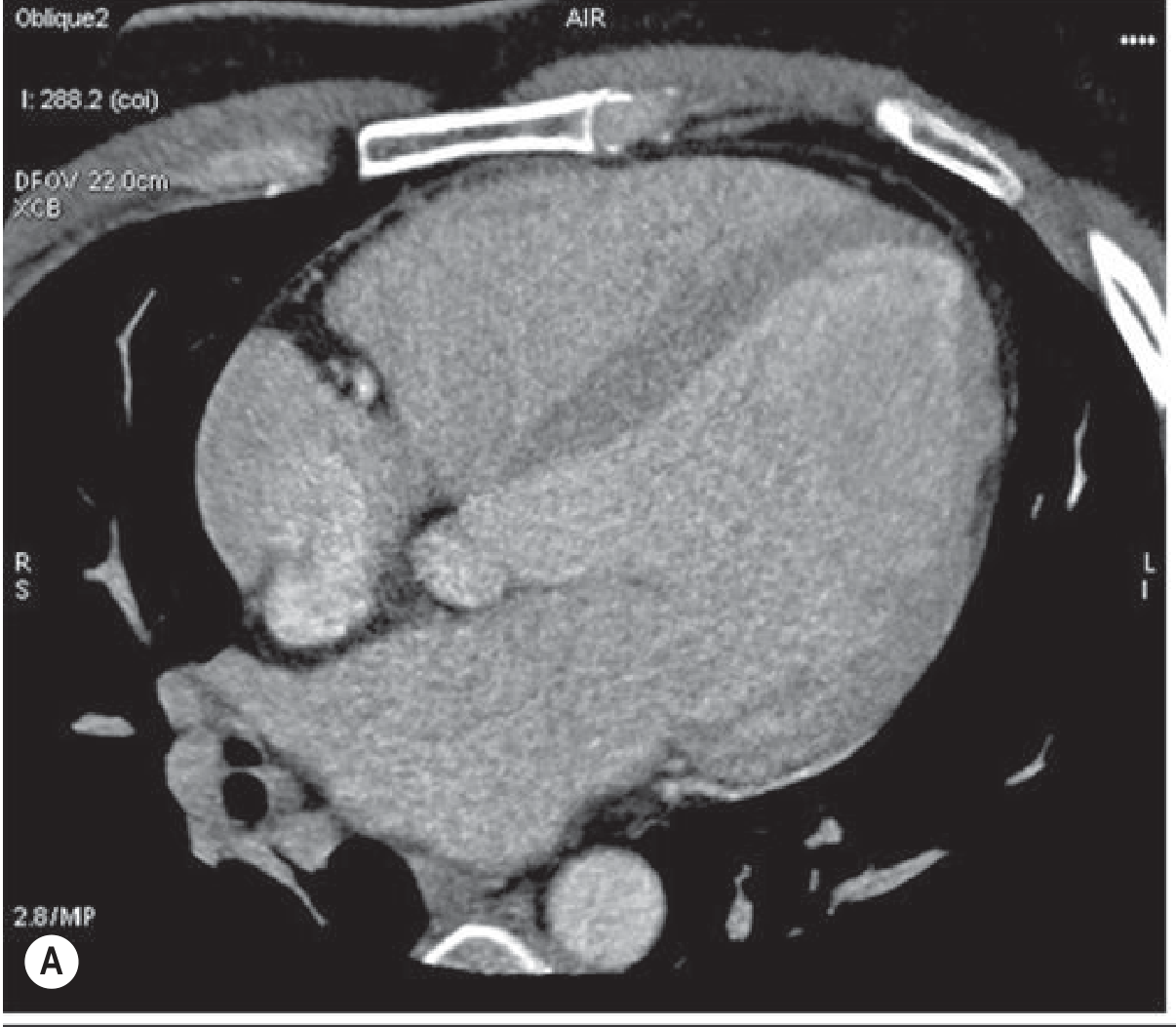
Cardiac CT
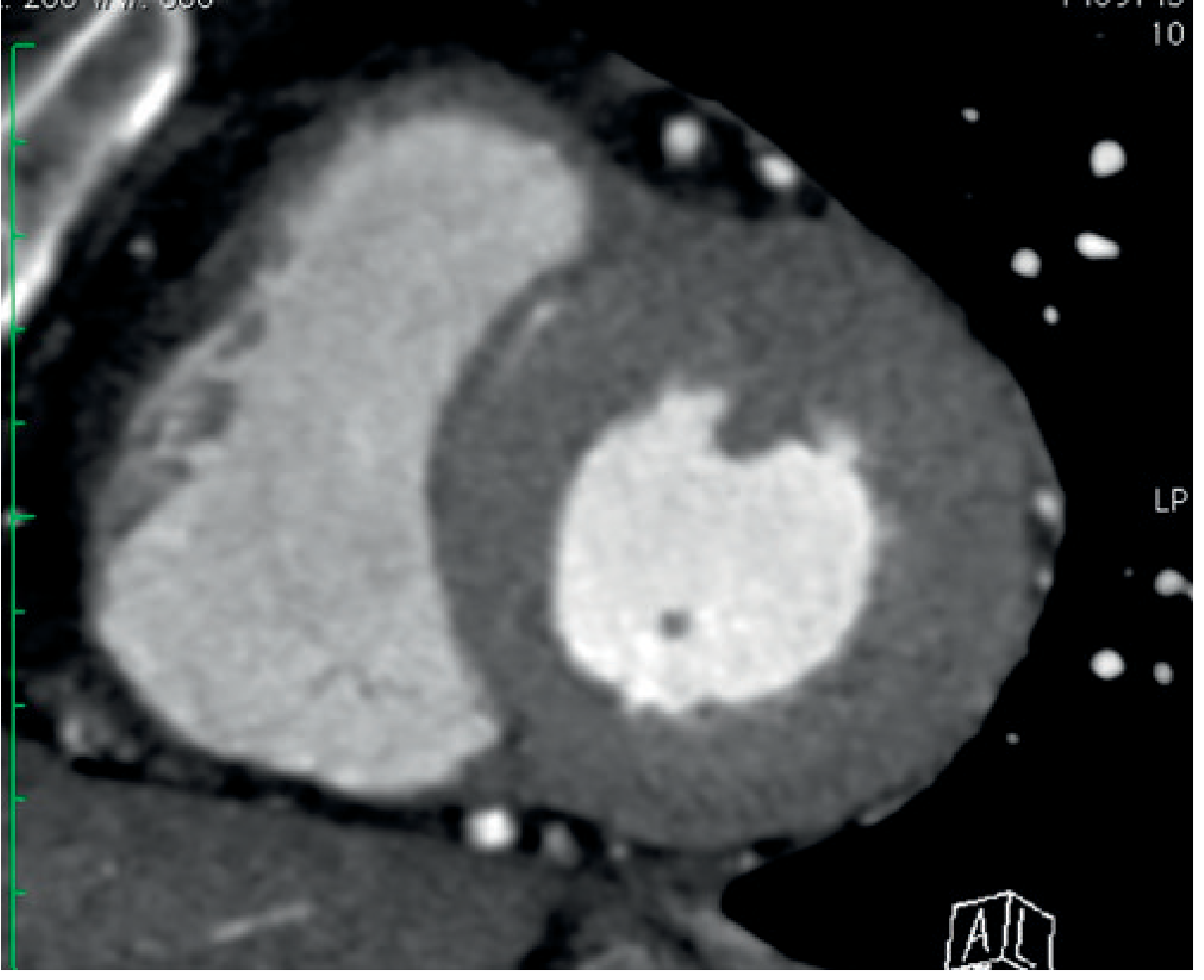
- Accurate wall thickness information at very low dose (1-3 mSv)
- Useful when MRI is contraindicated (pacemaker, claustrophobia)
- Can exclude coronary artery disease simultaneously
Special Variants of Hypertrophic Phenotype
| Disease | Imaging Pearl |
|---|---|
| Anderson-Fabry disease (AFD) | T1 mapping shows markedly LOW native T1; LGE at infero-lateral wall |
| Amyloidosis | "Sparkling" appearance on echo; LGE shows diffuse global subendocardial enhancement ("zebra pattern"); T1 mapping shows high native T1 |
| Athlete's heart | Symmetric hypertrophy; normal diastolic function; LGE absent; regresses with detraining |
| Hypertension | Concentric LVH; no LGE in pure hypertensive disease |
2. Dilated Cardiomyopathy (DCM)
Definition: Dilated, poorly contracting LV (or both ventricles) in the absence of abnormal loading conditions or coronary artery disease sufficient to cause global dysfunction.
Chest X-ray
- Cardiomegaly - cardiothoracic ratio >0.5
- Pulmonary venous congestion / pulmonary oedema in advanced disease
- Pleural effusions
Echocardiography
- Dilated LV with reduced EF (globally hypokinetic)
- Spherical LV shape
- Functional mitral regurgitation (dilated annulus)
- Diastolic dysfunction pattern
- LV thrombus detection (especially at apex)
Cardiac MRI
Key feature: Differentiating ischaemic from non-ischaemic DCM by LGE pattern
| Parameter | Ischaemic DCM | Non-ischaemic DCM |
|---|---|---|
| LGE pattern | Subendocardial or transmural; coronary territory distribution | Mid-wall/intramural striae (patchy fibrosis); subepicardial; may be absent |
| LGE distribution | Follows coronary artery territory | Non-territorial, often septal mid-wall |
| Coronaries on CTA | Atherosclerosis/occlusion | Normal |
| Clinical relevance | Guides revascularisation | Predicts arrhythmia risk |
Cardiac CT
- Coronary CT angiography to exclude ischaemic cause (now first-line in many centres)
- LV dilatation on 4-chamber views
- Myocardial thinning at infero-apical segments in ischaemic DCM
3. Restrictive Cardiomyopathy (RCM)
Definition: Increased wall stiffness causing rapid pressure rise with small volume increase; both ventricles normal/reduced in size with normal wall thickness (usually); diastolic dysfunction predominates.
Causes: Amyloidosis, sarcoidosis, haemochromatosis, Anderson-Fabry disease, endomyocardial fibrosis (Loeffler syndrome), radiation, carcinoid.
Chest X-ray
- Frequently unremarkable in early stages
- Advanced: left atrial enlargement, signs of elevated pulmonary venous pressure (similar to mitral stenosis)
Echocardiography
- Normal-sized or minimally enlarged ventricles with enlarged atria
- Normal or mildly decreased EF
- In Loeffler/endomyocardial fibroelastosis/carcinoid: endocardial thickening visible
- Doppler: elevated early diastolic velocity (E wave), short deceleration time, low atrial velocity (A wave) = restrictive filling pattern
- KEY challenge: must differentiate from constrictive pericarditis - similar Doppler findings
Key differentiating features (RCM vs Constrictive Pericarditis):
| Feature | RCM | Constrictive Pericarditis |
|---|---|---|
| Pericardial thickness | Normal (<4 mm) | Thickened (>4 mm) |
| IVS kinetics | Normal | Septal bounce |
| IVC on inspiration | No significant change | Collapses (>50%) |
| Myocardial LGE | Present (amyloid, sarcoid) | Absent |
| Pericardial enhancement | Absent | May be present |
Cardiac MRI
- Gold standard for pericardial thickness measurement: >4 mm predicts constriction
- T1 and T2 weighted: tissue characterisation of infiltrative diseases
- LGE patterns by specific diseases:
- Amyloidosis: diffuse global subendocardial enhancement; classic "zebra" or "leopard" pattern; rest T1 elevated; early blood-pool nulling
- Sarcoidosis: patchy, non-coronary territory LGE; predilection for basal septum and lateral wall; T2 high in active disease
- Haemochromatosis: LOW T2* signal (iron deposition causes susceptibility effect - myocardium appears dark on T2*)
- T1/T2 mapping: promising for differential diagnosis of infiltrative forms
4. Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)
Definition: Progressive replacement of RV myocardium by fibrofatty tissue; leads to RV dysfunction, ventricular arrhythmias, and sudden death in young athletes.
Chest X-ray
- May be normal or show mild cardiomegaly
- RV enlargement in advanced disease
Echocardiography
- RV dilatation and dysfunction (reduced RVEF)
- RV wall motion abnormalities (focal akinesis, dyskinesis)
- RVOT dilatation
- Limitation: poor RV acoustic window
Cardiac MRI (Modality of Choice)
- Gold standard for ARVC diagnosis
- Key findings:
- RV fatty infiltration: T1 high signal (fat) in RV free wall; however fat is also present in normal subjects, so presence alone is non-specific
- RV dilatation and dysfunction: reduced RVEF, increased RVEDV
- Regional wall motion abnormalities: focal akinesia, dyskinesia, or aneurysm of the RV free wall (triangle of dysplasia: RV inflow, outflow, and apex)
- LGE: fibrosis in RV wall; LV involvement in advanced cases
- Task Force Criteria (2010): structural/functional abnormalities on MRI are part of major and minor diagnostic criteria
Cardiac CT
- Can detect fatty infiltration in RV wall
- Structural assessment if MRI contraindicated
5. Myocarditis (Inflammatory Cardiomyopathy)
Echocardiography
- LV systolic dysfunction (regional or global)
- Pericardial effusion suggests inflammatory process
- Non-specific; cannot provide tissue diagnosis
Cardiac MRI - Lake Louise Criteria (Cornerstone)
Three-sequence protocol (must meet ≥2 criteria for diagnosis):
| Sequence | Finding | Meaning |
|---|---|---|
| T2-weighted (STIR) | Regional/global T2 signal increase | Myocardial oedema |
| Early gadolinium enhancement (EGE) | Global relative enhancement ratio >4 (blood pool vs myocardium) | Inflammatory hyperaemia/capillary leak |
| Late gadolinium enhancement (LGE) | Non-ischaemic distribution enhancement | Myocyte necrosis/fibrosis |
LGE pattern in myocarditis: classically subepicardial, most frequently in lateral and/or inferior wall.
- Easily distinguishable from MI (subendocardial/transmural, follows coronary territory)
- In Takotsubo CMP: LGE is typically absent - key differentiator
Important: Negative LGE does NOT exclude myocarditis - early/hyperaemic phase may show abnormality only on T2 and EGE without LGE.
6. Takotsubo (Stress) Cardiomyopathy
- Echo/CMR: Apical LV ballooning with hypercontractile basal segments (reverse apical ballooning pattern in atypical forms)
- LGE: Characteristically absent (no necrosis - distinguishes from STEMI and myocarditis)
- CMR: T2 elevation in apical segments (oedema); resolves with recovery
- Coronary angiography: normal coronaries
7. LV Non-Compaction (LVNC)
- Echo/CMR: Excessive trabeculation in LV; ratio of non-compacted to compacted layer >2.3 (MRI criterion); typically apical
- CMR is superior for trabeculation quantification
- LGE may be present in trabeculated segments
LGE Pattern Summary Table (High-Yield for Exam)
| Disease | LGE Location | Pattern |
|---|---|---|
| MI (ischaemic) | Subendocardial → transmural | Coronary territory |
| HCM | Intramural septum; RV insertion | Patchy, spares subendocardium |
| DCM (non-ischaemic) | Mid-wall septum | Linear/striae |
| Myocarditis | Subepicardial lateral/inferior | Non-territorial |
| Amyloidosis | Global subendocardial | "Zebra/leopard" pattern |
| Sarcoidosis | Basal septum, lateral wall | Patchy, non-territorial |
| ARVC | RV free wall | Fibrofatty |
| Haemochromatosis | Low T2* (dark) | Not LGE; T2* mapping |
| Takotsubo | Absent | - |
Key MRI Sequences and What They Show
| Sequence | Information |
|---|---|
| Cine (SSFP) | Morphology, function, volumes, EF, wall motion |
| T1-weighted | Anatomy; fat (bright); delayed enhancement (fibrosis) |
| T2-weighted (STIR) | Oedema detection; active inflammation |
| LGE (10-15 min post Gd) | Fibrosis, necrosis, infiltration |
| T1 mapping (native) | Elevated in amyloid/oedema; low in haemochromatosis/fat |
| T2 mapping | Oedema quantification |
| T2 mapping* | Iron overload (haemochromatosis - low T2*) |
| EGE (early gadolinium) | Hyperaemia/capillary leak (myocarditis) |
Exam Pearls
- CMR is the gold standard for tissue characterisation in all cardiomyopathies
- LGE spares subendocardium in HCM - key distinction from MI
- Myocarditis = subepicardial LGE laterally; Takotsubo = no LGE
- Amyloidosis: global subendocardial LGE + high native T1 + early blood-pool nulling + "sparkling" echo
- Haemochromatosis: low T2* (iron causes susceptibility artefact making myocardium dark)
- ARVC: RV fatty infiltration + RV dilatation/dysfunction + CMR Task Force Criteria
- Constrictive pericarditis vs RCM: pericardial thickness >4 mm on CT/MRI favours constriction
- DCM ischaemic vs non-ischaemic: subendocardial LGE in coronary territory = ischaemic; mid-wall septal LGE = non-ischaemic
- Cardiac CT provides coronary anatomy + wall thickness at low dose; used when MRI contraindicated or to exclude ischaemic cause in DCM
- Lake Louise Criteria require ≥2 of 3 (T2, EGE, LGE) for CMR diagnosis of myocarditis
Sources: Grainger & Allison's Diagnostic Radiology, Chapter 14 (Cardiomyopathies) | Braunwald's Heart Disease, 12th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.