Thyroglossal cyst case
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"thyroglossal duct cyst"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all I need for a thorough, well-illustrated clinical case discussion. Here is the complete breakdown:
Thyroglossal Duct Cyst (TDC) - Full Clinical Case Discussion
1. Embryology & Pathogenesis
The thyroid gland originates as a median endodermal thickening (thyroid diverticulum) at the foramen cecum at the base of the tongue. It descends through the midline of the neck to its final pretracheal position, remaining tethered to the tongue by the thyroglossal duct. During this descent, the duct passes through - and becomes intimately related to - the central portion of the hyoid bone, which forms from the 2nd and 3rd branchial arch cartilages simultaneously.
The duct normally involutes and disappears by the 8th-10th week of gestation. If any portion persists, secretions from its epithelial lining accumulate, forming a cyst. This explains the critical anatomic relationship: the cyst is almost always connected to the hyoid bone via a tract.
"An upper midline cystic neck lesion in toddlers is a thyroglossal duct cyst until proven otherwise." - Sabiston Textbook of Surgery
2. Epidemiology
- Most common congenital cystic neck mass in children
- Second most common benign neck mass after benign lymphadenopathy
- Predominantly pediatric, but can present at any age
- 75% occur in the midline; the rest occur up to 2 cm off the midline
- 65% are infrahyoid (below hyoid bone), 15% at the level of hyoid, 20% suprahyoid or intralingual
3. Clinical Presentation
Typical features:
| Feature | Detail |
|---|---|
| Location | Midline anterior neck, most often just below the hyoid bone |
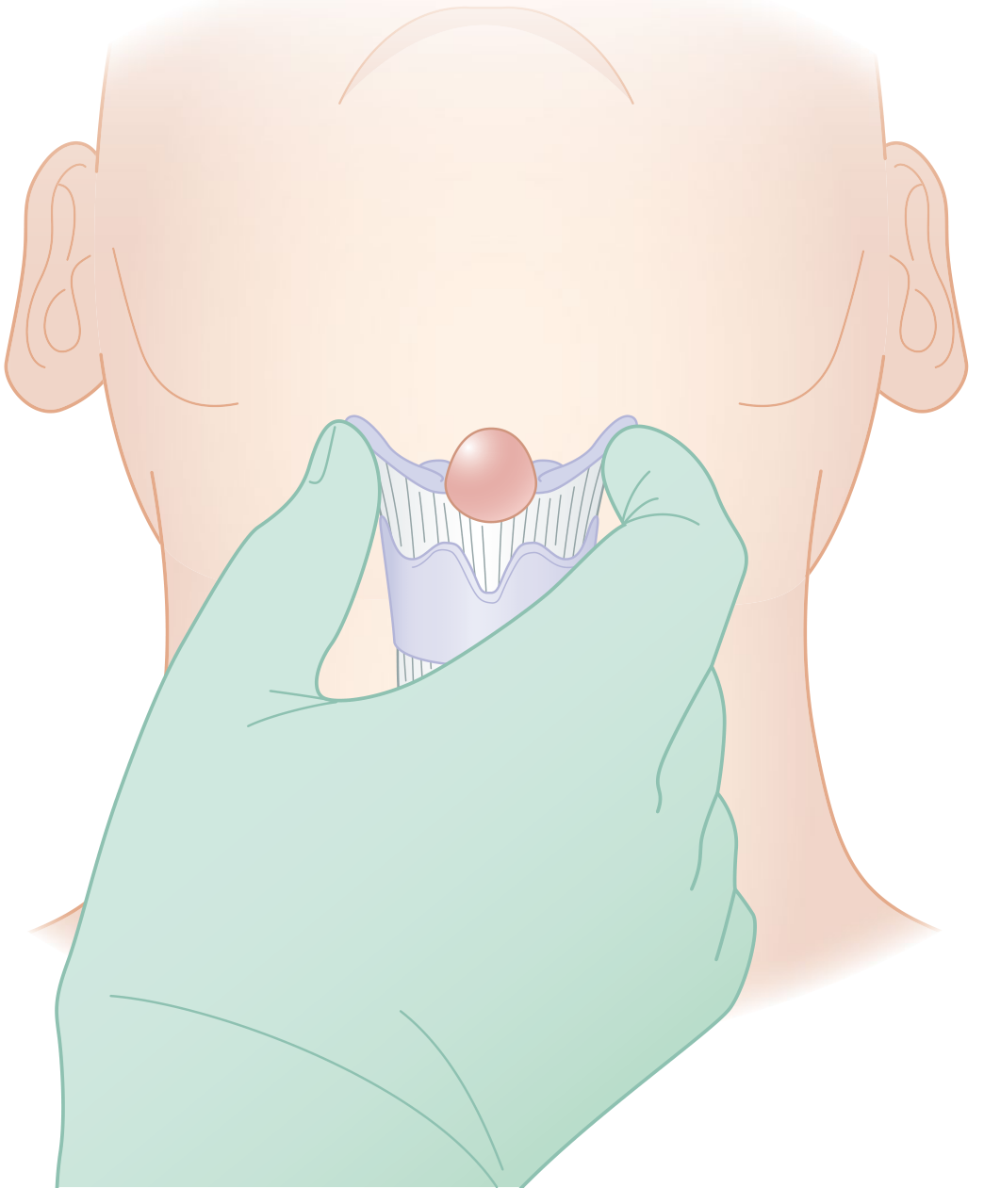
| Character | Smooth, fluctuant, non-tender cystic swelling |
| Pathognomonic sign | Moves upward with tongue protrusion AND swallowing (due to attachment via tract to foramen cecum) |
| Age | Most common in children; second peak in adults |
| Size | Typically 1-4 cm |
Complications that alter the presentation:
- Infection - the cyst becomes acutely painful, red, tender, and fluctuant; may discharge spontaneously creating a thyroglossal fistula
- Dysphagia or dyspnea - rare, with very large cysts
- Lingual thyroid - if the thyroid failed to descend fully, the only thyroid tissue may be at the base of the tongue; a thyroglossal mass in this setting may represent the patient's sole functioning thyroid
4. Investigations
Clinical Diagnosis
Primarily clinical - based on characteristic midline mobile mass that rises with tongue protrusion.
Imaging
Ultrasound (first-line):
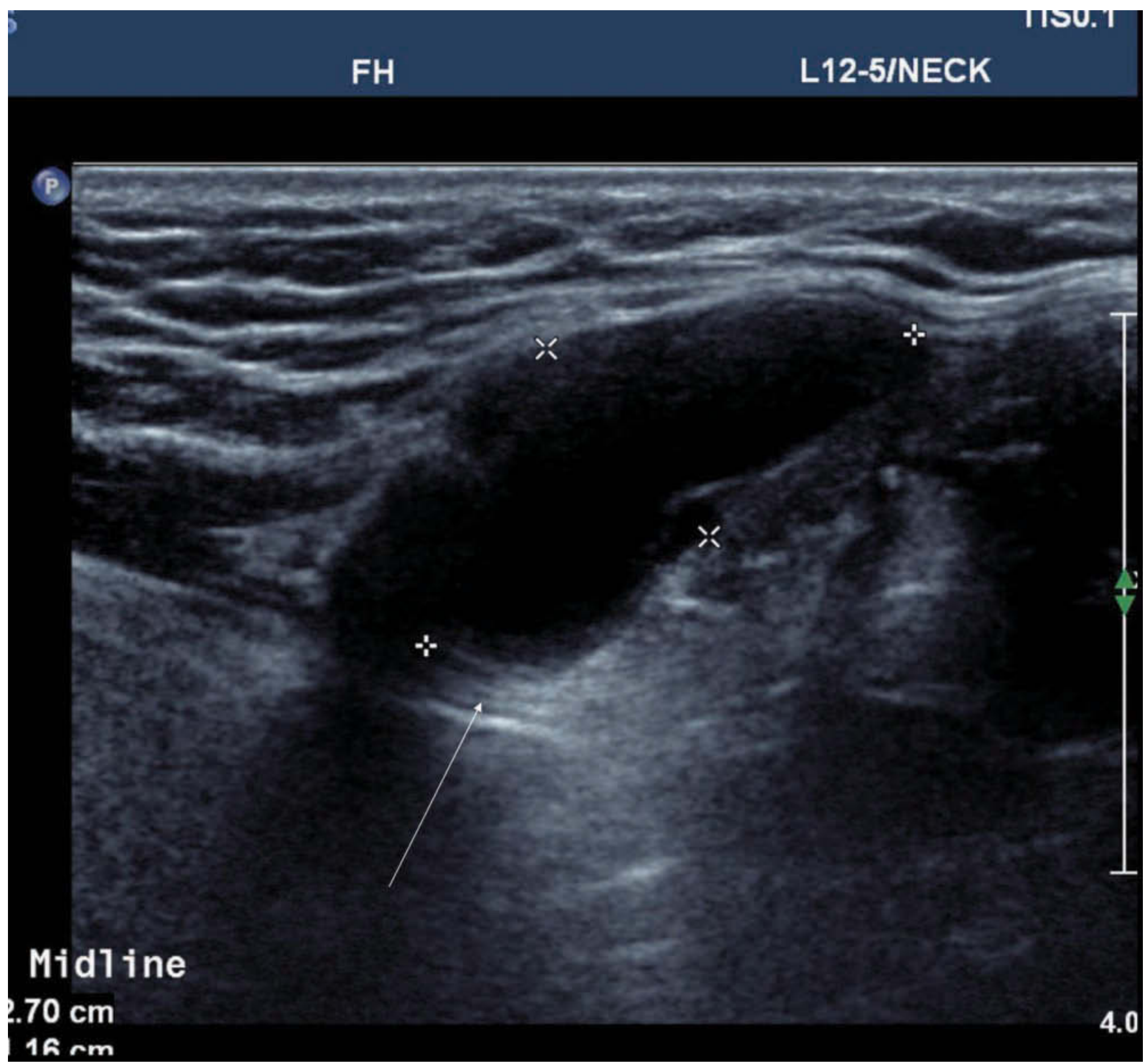
Ultrasound showing a midline infrahyoid homogenous anechoic cystic mass with posterior wall enhancement (arrow) - classic TDC appearance. (Scott-Brown's Otorhinolaryngology)
Ultrasound appearances vary:
- Classic: homogenous anechoic with posterior wall enhancement
- Pseudosolid: due to proteinaceous secretions
- Heterogeneous: from previous haemorrhage or infection
CT/MRI: Used when ultrasound is inconclusive or when the anatomy is complex. MRI shows invariably high T2 signal, with variable T1 depending on protein content.
Key imaging objectives:
- Confirm the cyst's relationship to the hyoid bone
- Confirm presence of normal thyroid tissue in the neck (to exclude ectopic/lingual thyroid as sole thyroid)
- Identify any solid component within the cyst - there is a ~1% incidence of carcinoma (classically papillary thyroid carcinoma) within TDCs
FNA/Biopsy: Used selectively to exclude malignancy or rule out other neck masses when diagnosis is uncertain.
5. Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Dermoid/epidermoid cyst | Midline, but does NOT move with tongue protrusion; usually suprahyoid |
| Lipoma | Soft, non-cystic, does not move with tongue |
| Enlarged submental lymph node | Reactive tenderness, may enlarge with URTI |
| Branchial cleft cyst | Lateral neck, angle of mandible/anterior SCM border |
| Lingual thyroid | Mass at base of tongue; confirm absence of normal thyroid |
| Sebaceous cyst | Superficial, attached to skin, punctum visible |
| Median ectopic thyroid | No movement with tongue, rule out with radionuclide scan |
6. Pathology (Histology)
From Robbins Pathologic Basis of Disease:
- Cysts lined by stratified squamous epithelium when near the tongue base, or pseudostratified columnar (respiratory) epithelium in lower locations; transitional patterns also occur
- Fibrous cyst wall often contains lymphoid aggregates and thyroid follicular remnants
- Malignant transformation of the lining is exceedingly rare (~1%), most commonly papillary thyroid carcinoma
7. Treatment
The Sistrunk Procedure (Gold Standard)
First described in 1928, this is the standard operation. Simple cystectomy alone is associated with 40-50% recurrence because residual duct tissue, particularly within the hyoid bone, seeds new cyst formation.
The Sistrunk procedure - the cyst and its tract run intimately through the central portion of the hyoid bone up to the foramen cecum at the tongue base. (Sabiston Textbook of Surgery)
What the Sistrunk procedure includes:
- Complete excision of the cyst
- Resection of the central portion of the hyoid bone (central ~1 cm)
- Removal of the tract above the hyoid bone continuing all the way to the base of the tongue (foramen cecum)
This removes all potential remnant duct tissue and dramatically reduces recurrence rates.
If infection is present: The infected cyst should first be treated with antibiotics and/or I&D. Definitive Sistrunk procedure is deferred to 6-8 weeks after the infection has fully resolved, to allow tissue planes to become clear.
8. Pre-operative Checklist
Before surgery, always confirm:
- Normal thyroid gland is present in the neck on imaging (US)
- No solid component within cyst suggesting malignancy (if present, plan for more extensive surgery)
- Active infection has resolved
- Thyroid function tests if ectopic/lingual thyroid is a concern
9. Complications of Surgery
- Recurrence (most common cause: inadequate resection of tract/hyoid)
- Wound infection
- Haematoma
- Injury to adjacent structures (uncommon)
- Hypothyroidism (if inadvertent removal of ectopic thyroid tissue that was the sole thyroid)
10. Malignancy in TDC
- ~1% incidence of carcinoma within the cyst
- Overwhelmingly papillary thyroid carcinoma (PTC)
- Management involves total thyroidectomy in addition to Sistrunk procedure, followed by radioiodine ablation if indicated
- Prognosis is generally good when managed appropriately
Sources: Sabiston Textbook of Surgery (p. 1343, p. 2674); Scott-Brown's Otorhinolaryngology Head & Neck Surgery (p. 627); Robbins & Cotran Pathologic Basis of Disease (p. 694)
This is a shared conversation. Sign in to Orris to start your own chat.