hernia
Reading File
Asking for Preferences
Finding Sources
Searching the Web
hernia types classification anatomy surgical management overview
Reading File
Reading File
Searching Images
hernia types anatomy inguinal femoral umbilical diagram
Finding Sources
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of hernias.
Hernia — Clinical Overview
Definition
A hernia is the protrusion of an organ or tissue through an abnormal opening in the wall that normally contains it. Most abdominal hernias consist of a sac (peritoneal outpouching), a neck (the opening through which content protrudes), and contents (bowel, omentum, or other viscera).
Classification
By Reducibility
| State | Definition |
|---|---|
| Reducible | Contents can be returned to their normal position spontaneously or manually |
| Incarcerated | Contents cannot be reduced; does not imply ischemia |
| Strangulated | Blood supply is compromised — a surgical emergency |
Smaller hernial necks carry a disproportionately higher risk of strangulation. Up to 40% of femoral hernias are strangulated at initial presentation, compared with only 2% of incisional hernias. — Sleisenger & Fordtran's GI and Liver Disease
By Origin
- Congenital — patent processus vaginalis (indirect inguinal), omphalocele, umbilical
- Acquired — direct inguinal, incisional, hiatal (from raised intra-abdominal pressure, aging, obesity)
Anatomical Locations
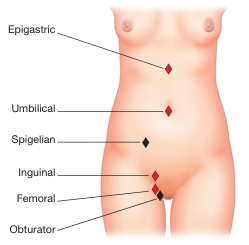
Anterior abdominal wall hernia locations — Bailey & Love's Surgery, 28th ed., p. 1086
Major Types
1. Indirect Inguinal Hernia ← Most common overall
- Passes through the deep (internal) inguinal ring, travels the inguinal canal, and may descend into the scrotum
- Located lateral to the inferior epigastric vessels
- Caused by a patent processus vaginalis (congenital); ~5% of full-term neonates, ~30% of preterm infants are affected
- Predominates in males and is most commonly diagnosed in children and young adults
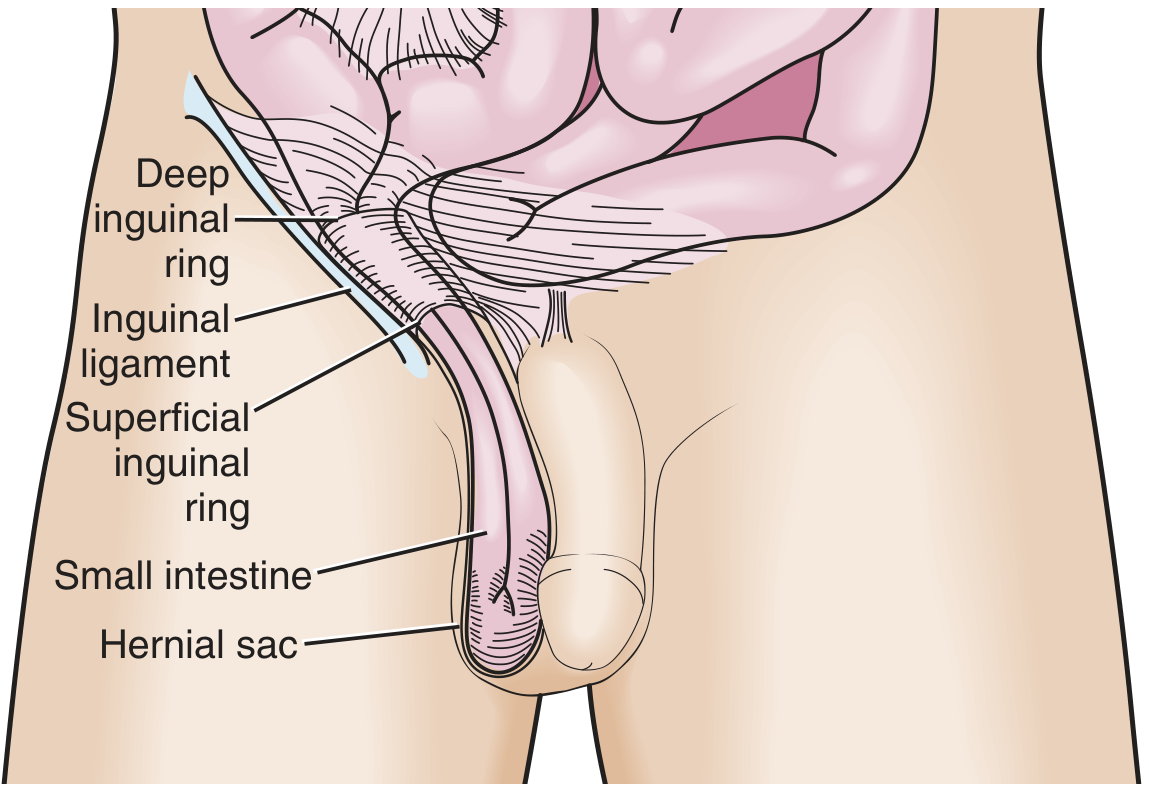
Indirect inguinal hernia — Roberts & Hedges' Clinical Procedures in Emergency Medicine
2. Direct Inguinal Hernia
- Protrudes directly through the posterior wall of the inguinal canal (Hesselbach's triangle), medial to the inferior epigastric vessels
- Acquired — caused by progressive weakening from aging and repetitive increases in intra-abdominal pressure
- Wide neck → lower risk of incarceration than indirect hernias
3. Pantaloon Hernia
- A combination of both direct and indirect components straddling the inferior epigastric vessels
- Often only discovered at surgery; difficult to sustain reduction in the ED
4. Femoral Hernia
- Passes through the femoral canal, below and lateral to the pubic tubercle, medial to the femoral vessels
- More common in females (especially multiparous)
- High risk of strangulation (up to 40% at presentation) due to the rigid, narrow femoral ring
5. Umbilical Hernia
- Protrusion through the umbilical ring
- Common in neonates (usually closes spontaneously by age 3–5); in adults it is acquired (obesity, ascites, pregnancy)
- Accounts for ~15% of emergency hernia surgery; up to 60% of these show strangulation at operation
6. Epigastric Hernia
- Protrusion through the linea alba between the xiphoid and umbilicus
- Usually contains pre-peritoneal fat; may be painful out of proportion to size
7. Spigelian Hernia
- Occurs along the semilunar line (lateral edge of the rectus sheath), typically below the arcuate line
- Interparietal — lies beneath the external oblique → may be occult on examination but symptomatic
8. Incisional Hernia
- Through a prior surgical wound; lifetime risk after laparotomy ~10–15%
- Wide neck → low rate of strangulation (~2%), but large size can cause morbidity
9. Hiatal Hernia
- Stomach herniates through the diaphragmatic hiatus into the chest
- Type I (sliding): GEJ migrates superiorly — most common (~95%), associated with GERD
- Type II (paraesophageal): fundus herniates with GEJ in normal position
- Types III & IV: mixed / giant, with other organs (colon, spleen) involved
10. Internal Hernias
- Herniation into a peritoneal recess or through a mesenteric defect; most commonly paraduodenal (congenital) or iatrogenic (after Roux-en-Y bypass, colectomy, Whipple procedure)
Clinical Presentation
| Feature | Classic finding |
|---|---|
| Groin/abdominal bulge | Worse on standing/straining; reduces on lying down |
| Pain/discomfort | Dragging ache; sharp pain suggests incarceration |
| Nausea/vomiting | Suggests obstruction from incarcerated bowel |
| Skin erythema, fever | Suggests strangulation — emergency |
Cough impulse (visible or palpable expansion on coughing) is a classic sign. Absence does not exclude hernia.
In obese patients, incarceration can be difficult to identify clinically; CT is often required.
Complications
- Incarceration → bowel obstruction — hernia accounts for up to 44.5% of small bowel obstruction operations in some series
- Strangulation → ischemia (in up to 75% of hernia-related SBO surgeries) → necrosis (>25%) → perforation → peritonitis
- Obstruction of other structures: bladder (inguinal), ovary/fallopian tube (inguinal in females), ureter
Management
Watchful Waiting
Appropriate for minimally symptomatic or asymptomatic inguinal hernias in adults. Evidence shows increased morbidity with emergency vs. elective repair, so timely referral remains important.
Surgery — Indications
- Symptomatic hernias
- Incarcerated hernia (urgent)
- Strangulation (emergency)
- Femoral hernias (always repair given high strangulation risk)
Surgical Approaches
| Technique | Key features |
|---|---|
| Open Lichtenstein (tension-free mesh) | Gold standard for inguinal; low recurrence (~1%) |
| Laparoscopic TAPP (Transabdominal Preperitoneal) | Mesh via laparoscope; good for bilateral/recurrent |
| Laparoscopic TEP (Totally Extraperitoneal) | No peritoneal entry; reduced intraperitoneal risk |
| Open tissue repair (Shouldice, Bassini) | Reserved where mesh is contraindicated (infection) |
| Emergency repair | Bowel resection may be required if strangulated |
Manual reduction of an incarcerated hernia may be attempted when strangulation is not suspected; contraindicated if there is severe tenderness, skin erythema, or systemic signs — these mandate urgent operative exploration.
Key Risk Factors
- Male sex (inguinal), female sex (femoral)
- Prematurity (indirect inguinal)
- Obesity, chronic straining (constipation, COPD, heavy lifting)
- Prior abdominal surgery (incisional)
- Ascites, pregnancy (umbilical)
- Connective tissue disorders (Marfan, Ehlers-Danlos)
Sources: Roberts & Hedges' Clinical Procedures in Emergency Medicine; Sleisenger & Fordtran's GI and Liver Disease; Bailey & Love's Short Practice of Surgery, 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.