Best definition of hernia
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Here is the best definition of hernia, drawn from multiple authoritative surgical and medical textbooks:
Definition of Hernia
"A hernia is defined as a protrusion of any viscus from its normal cavity through an abnormal opening."
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
This is the classic, most concise surgical definition. Several other major textbooks expand on it:
"A hernia is defined as protrusion of whole or a part of a viscus through the wall that contains it."
- S. Das: A Manual on Clinical Surgery, 13th Ed.
"A hernia is defined as an abnormal bulge, protrusion, or projection of an organ, or part of an organ, through the wall of a cavity within which it is usually contained."
- Yamada's Textbook of Gastroenterology, 7th Ed.
"Hernias are generally defined as an abnormal bulge or protrusion of an organ through a cavity wall."
- Fischer's Mastery of Surgery, 8th Ed.
Breaking It Down
A complete hernia has three components:
| Component | Description |
|---|---|
| Hernial sac | A pouch of peritoneum pushed through the defect |
| Hernial contents | The structures inside the sac (bowel, omentum, etc.) |
| Hernial defect | The abnormal opening or weakness in the containing wall |
Note from Maingot's Abdominal Operations: "the term hernia refers to the actual anatomic weakness or defect, and hernia contents describe those structures that pass through the defect."
Clinical Classification
Once defined, hernias are further classified by reducibility:
- Reducible - contents can be returned through the defect manually
- Incarcerated (irreducible) - contents cannot be returned without surgery; often due to swelling of sac contents
- Strangulated - an incarcerated hernia where blood supply to the herniated structure is compromised - a surgical emergency
Common Locations
Abdominal hernias (75% occur in the groin) can arise:
- Along a congenital tract that fails to close (e.g., indirect inguinal, umbilical)
- Along an area of weakness in muscle/fascia (e.g., direct inguinal, ventral, incisional)
Weakness may result from aging, increased intra-abdominal pressure, poor wound healing, or trauma.
Search for clinical images showing different hernia presentations
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Loading Image
Here is a comprehensive visual tour of different hernia presentations from authoritative surgical and emergency medicine textbooks:
Clinical Images: Different Hernia Presentations
1. Inguinal Hernia - Clinical Photograph
(Schwartz's Principles of Surgery, 11th Ed.)
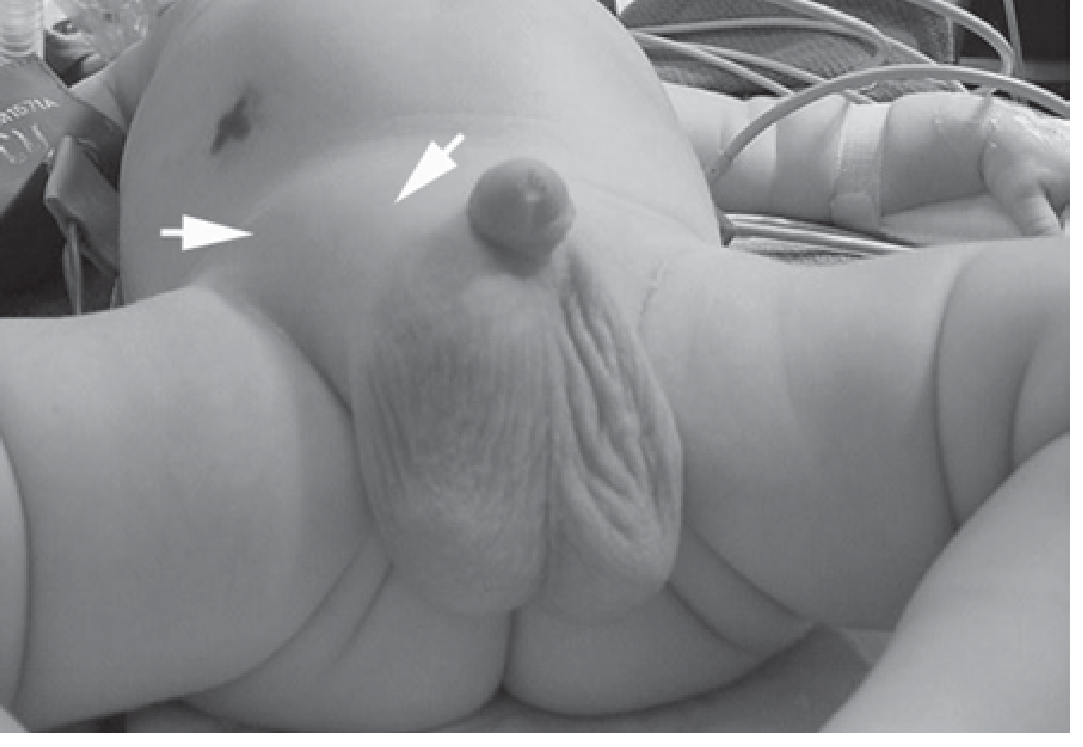
A right inguinal hernia in an infant - the classic presentation is a visible, palpable groin bulge extending into the scrotum. The two arrows mark the hernia and the contralateral umbilical region for comparison.
2. Indirect Inguinal Hernia - Anatomical Diagram
(Roberts and Hedges' Clinical Procedures in Emergency Medicine)
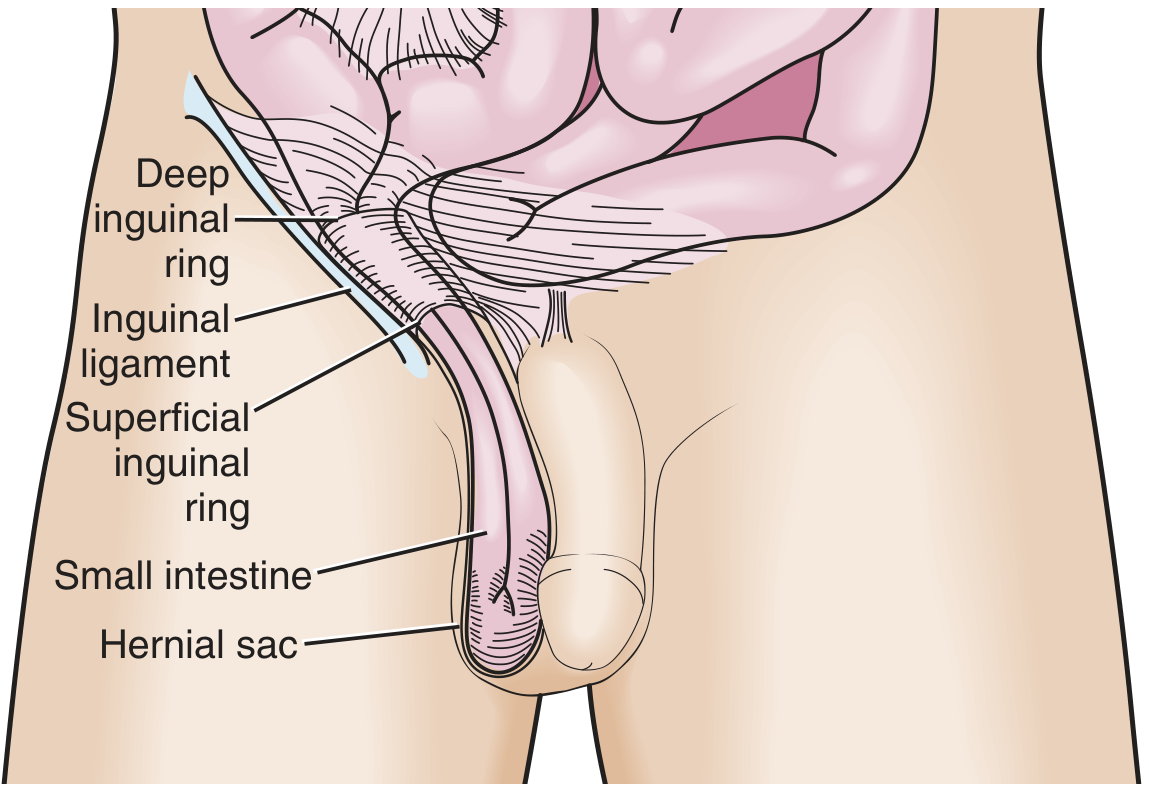
Small intestine passes through the deep inguinal ring, travels the full length of the inguinal canal, and descends into the hernial sac in the scrotum. This is the most common hernia type overall.
3. Direct Inguinal Hernia - Anatomical Diagram
(Roberts and Hedges' Clinical Procedures in Emergency Medicine)
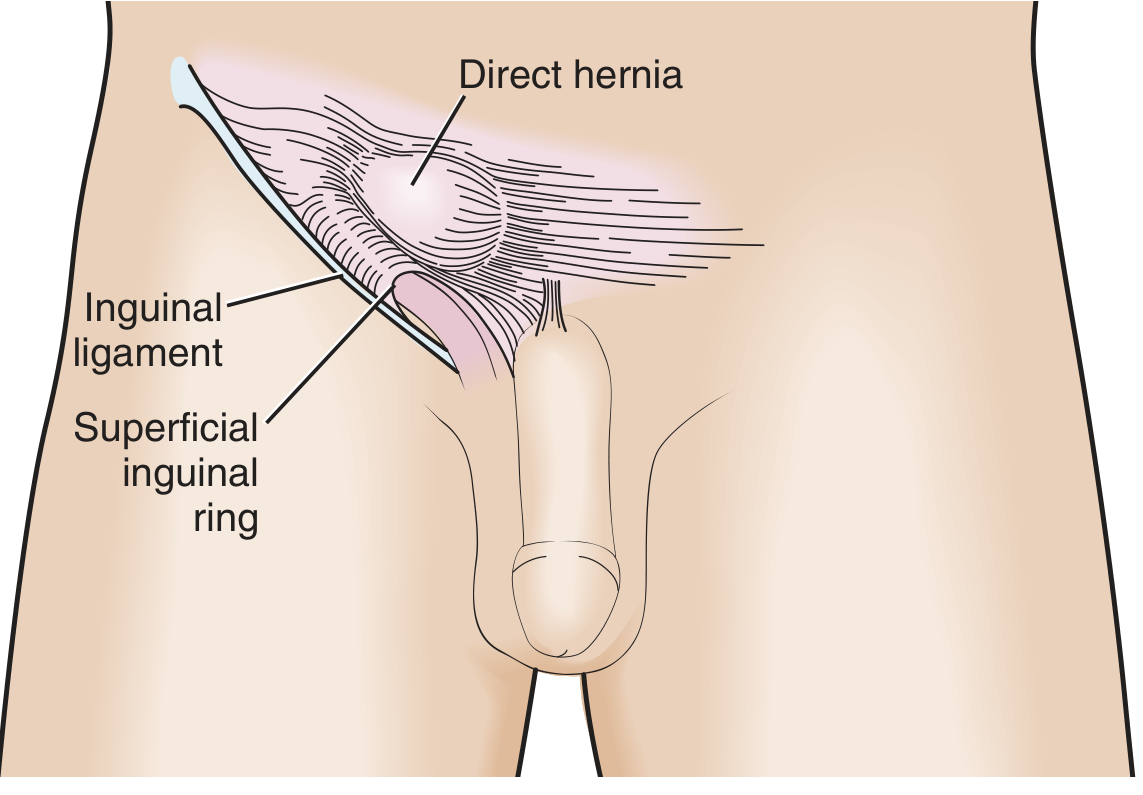
The hernia pushes directly through the posterior wall of the inguinal canal, medial to the inferior epigastric vessels. It does NOT descend into the scrotum. Acquired in older adults due to muscle weakness.
4. Ventral Hernias - Overview Diagram (Incisional, Umbilical, Epigastric, Spigelian)
(Roberts and Hedges' Clinical Procedures in Emergency Medicine)
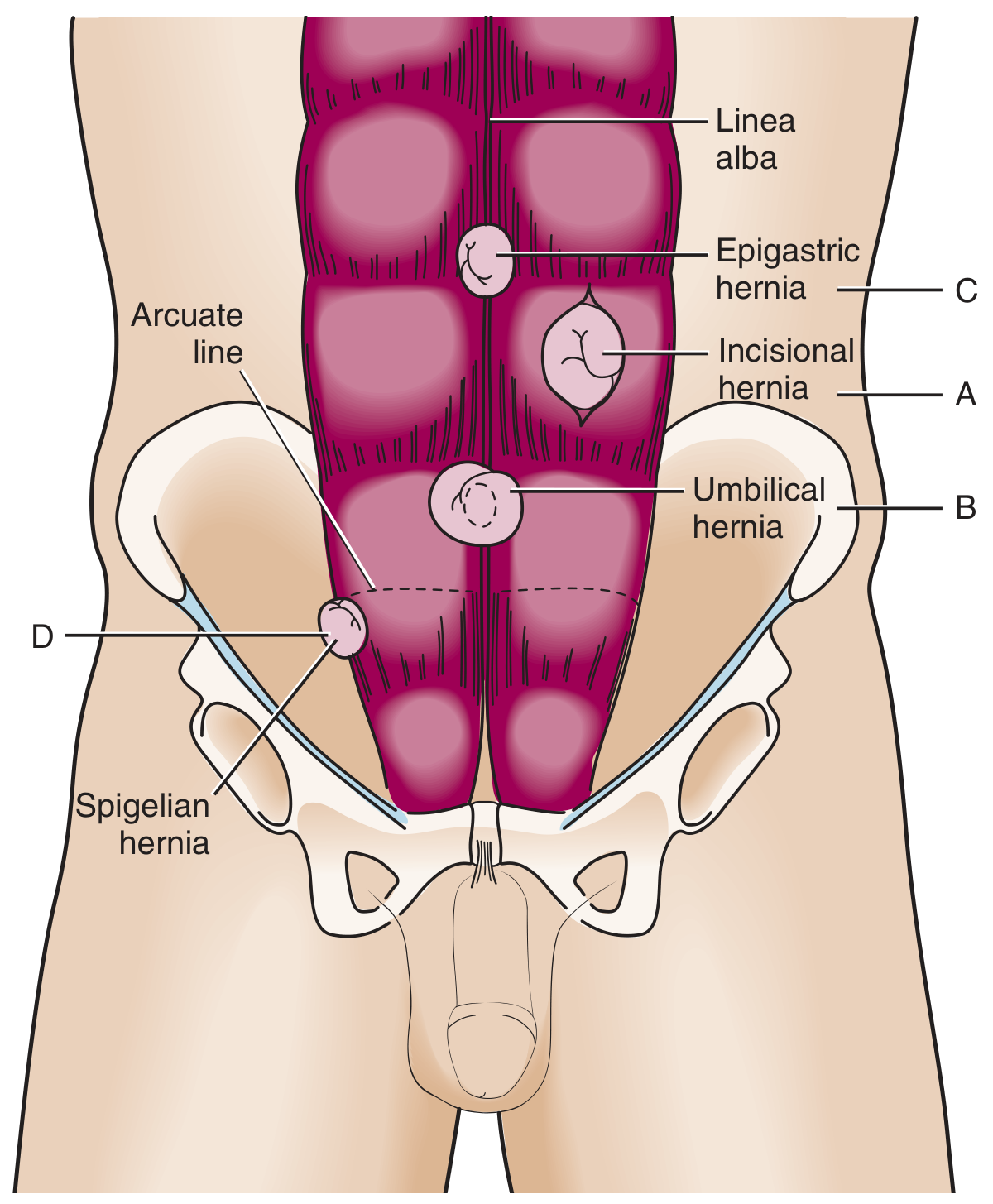
This single diagram neatly maps all four major ventral hernia sites:
- A - Incisional hernia: through a prior surgical scar
- B - Umbilical hernia: through the umbilical ring
- C - Epigastric hernia: through the linea alba, above the umbilicus
- D - Spigelian hernia: lateral to the rectus abdominis, at the arcuate line - often occult (under the skin)
5. Incarcerated Spigelian Hernia - CT Scan
(Fischer's Mastery of Surgery, 8th Ed.)
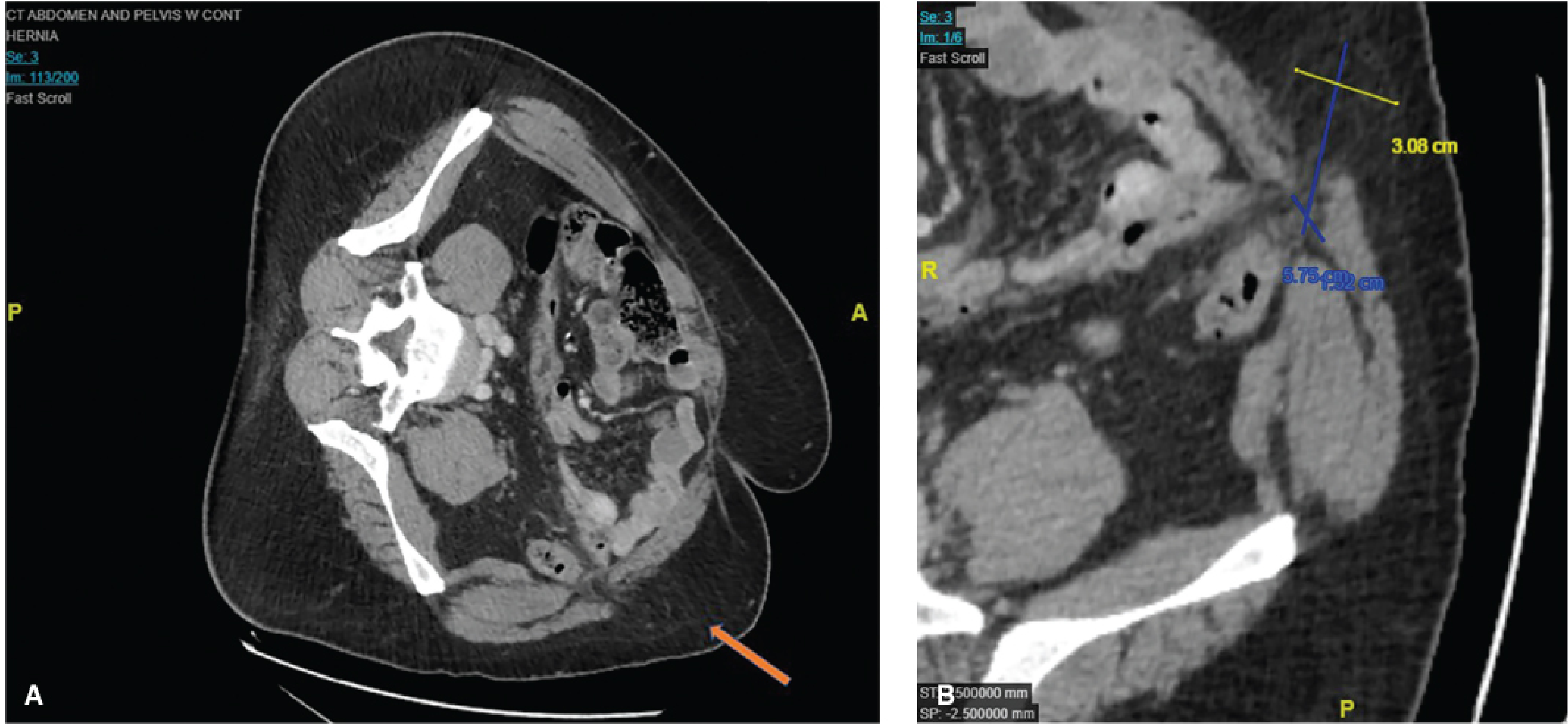
CT abdomen (axial + sagittal) of a 50-year-old man with an incarcerated spigelian hernia. The orange arrow marks the hernia defect. Sagittal view shows the defect measures approximately 3.08 x 5.75 cm. Spigelian hernias are rare and often clinically occult - CT is the investigation of choice.
6. Hiatal Hernia - Barium Studies + Endoscopy
(Sleisenger & Fordtran's Gastrointestinal and Liver Disease)
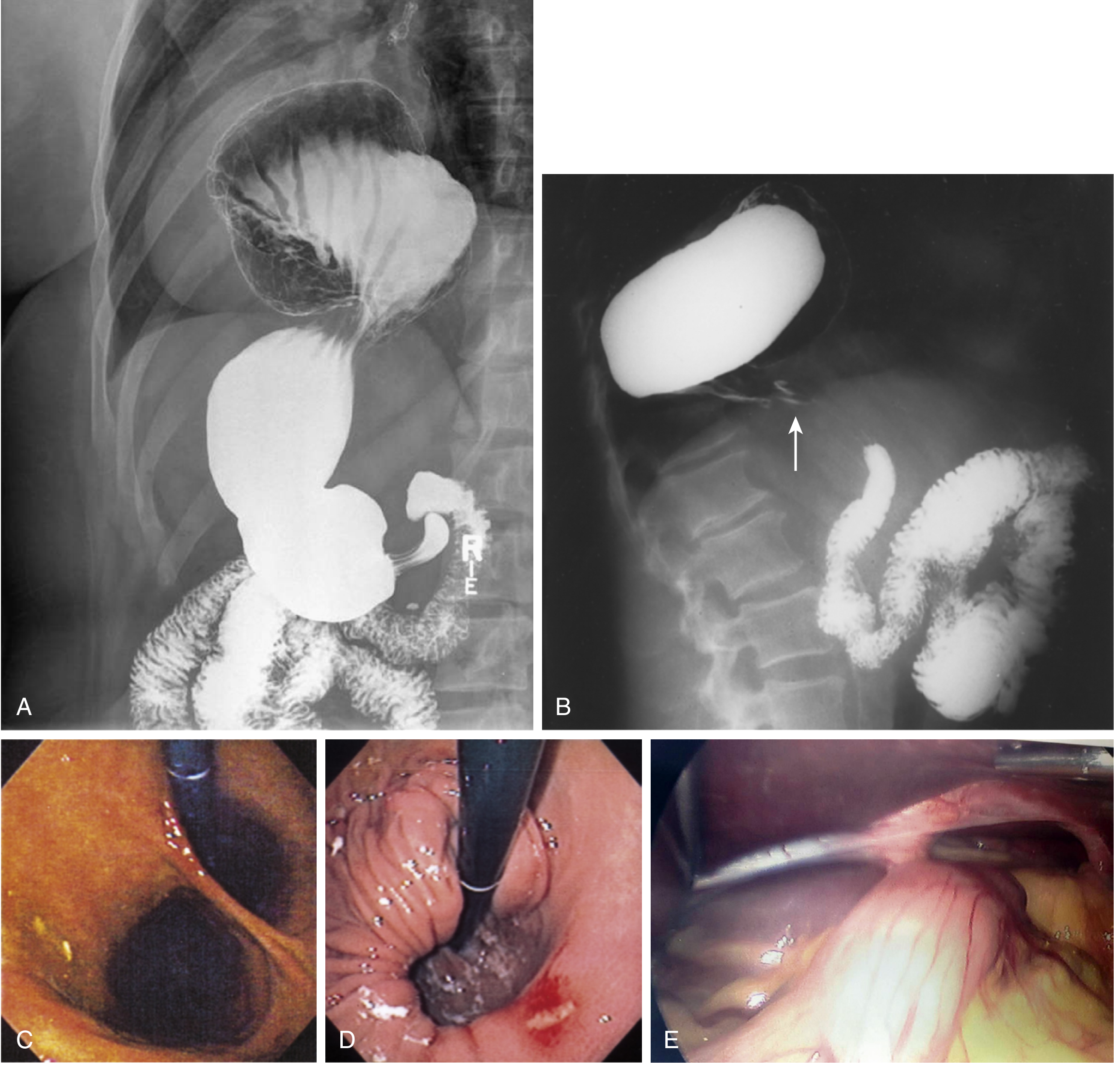
A multimodal panel showing hiatal hernia:
- A - Barium swallow: gastric folds visible above the diaphragm (sliding hiatal hernia)
- B - Barium: paraesophageal hernia with gastric volvulus (arrow = diaphragmatic hiatus)
- C/D - Endoscopy: gastric folds at the cardia; erosive changes from acid exposure
- E - Laparoscopic view: stomach herniating through the hiatus
Summary Table
| Hernia Type | Location | Key Feature |
|---|---|---|
| Indirect inguinal | Lateral to epigastrics, through inguinal canal | Most common; congenital; may reach scrotum |
| Direct inguinal | Medial to epigastrics, through posterior wall | Acquired; older men; rarely incarcerates |
| Umbilical | Through umbilical ring | Common in infants and multiparous women |
| Epigastric | Linea alba, above umbilicus | Small fat-containing defects |
| Incisional | Along prior surgical scar | Occurs in ~20% of laparotomies |
| Spigelian | Lateral rectus edge, arcuate line | Occult; CT needed to diagnose |
| Hiatal | Gastroesophageal junction / diaphragm | Stomach herniates into chest |
Exact location of deep inguinal ring and superficial inguinal ring, and from which they are made up of.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Here is a detailed, textbook-sourced breakdown of both inguinal rings:
The Inguinal Rings - Exact Location and Composition
Overview: The Inguinal Canal
The inguinal canal is a ~4 cm oblique passage running downward and medially, just above and parallel to the lower half of the inguinal ligament. It has two openings - the deep ring at its start and the superficial ring at its end.
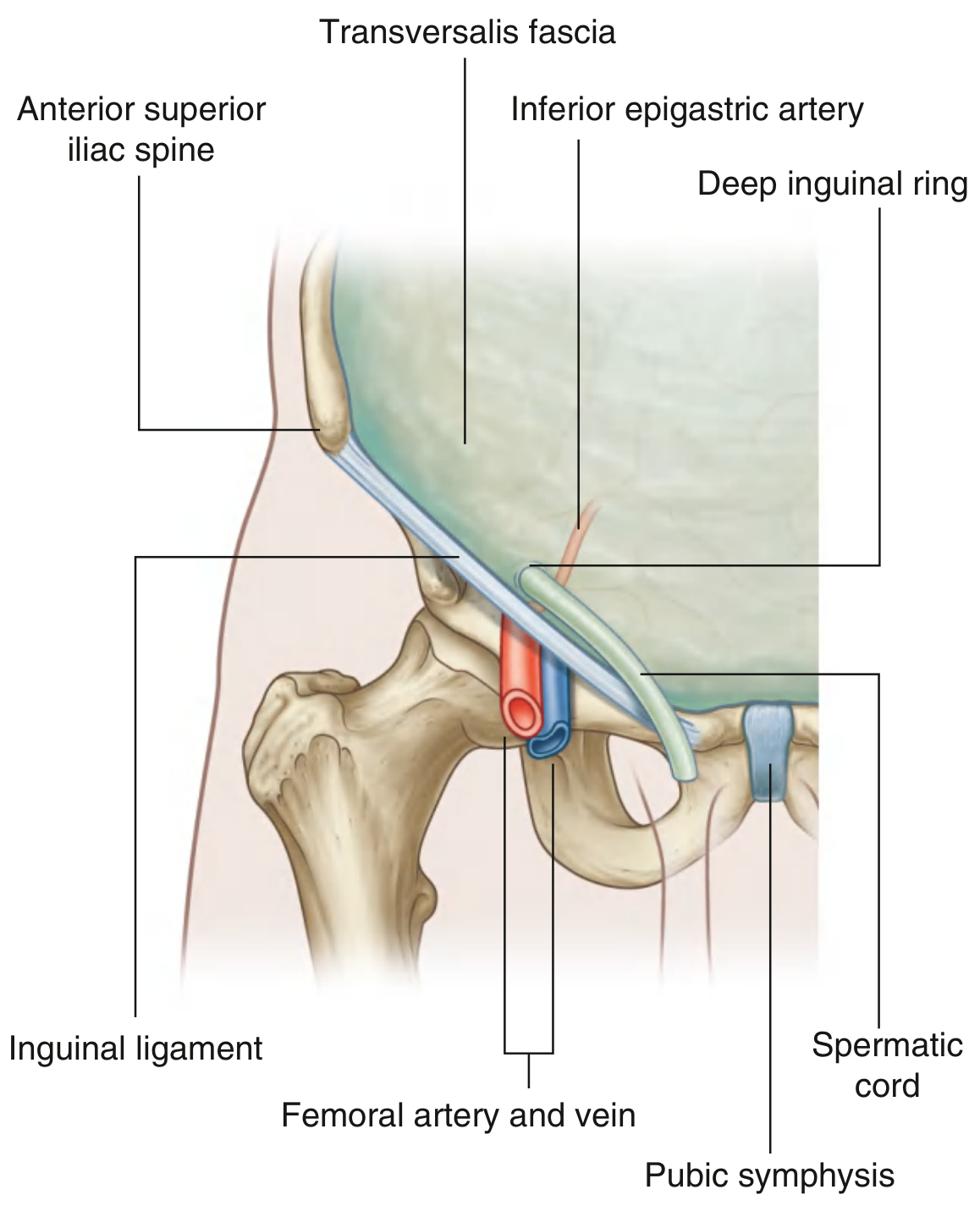
1. Deep Inguinal Ring (Internal Inguinal Ring)
Exact Location
"At a point midway between the anterior superior iliac spine (ASIS) and the pubic symphysis, just above the inguinal ligament, immediately lateral to the inferior epigastric vessels."
- Gray's Anatomy for Students
"Midway between the anterior superior iliac spine and the pubic tubercle, approximately 2-3 cm above and marginally lateral to the femoral artery pulse in the groin."
- Bailey and Love's Short Practice of Surgery, 28th Ed.
Note the landmark difference: Gray's uses ASIS to pubic symphysis (mid-inguinal point), while Bailey & Love uses ASIS to pubic tubercle (midpoint of inguinal ligament). Both place it just lateral to the inferior epigastric vessels.
What It Is Made Of
"An outpouching of the transversalis fascia (becomes the internal spermatic fascia)."
- Thieme Atlas of Anatomy
"Although sometimes referred to as a defect or opening in the transversalis fascia, it is actually the beginning of the tubular evagination of transversalis fascia that forms one of the coverings (the internal spermatic fascia) of the spermatic cord in men, or the round ligament of the uterus in women."
- Gray's Anatomy for Students
It is bounded by:
- Medially: the inferior epigastric vessels (the key surgical landmark separating direct from indirect hernias)
- Inferiorly: the inguinal ligament
- Superolaterally: the interfoveolar ligament (thickening of transversalis fascia)
- Muscle fibres of transversus abdominis and internal oblique arch over it from lateral to medial, descending to form the conjoint tendon at the pubic tubercle
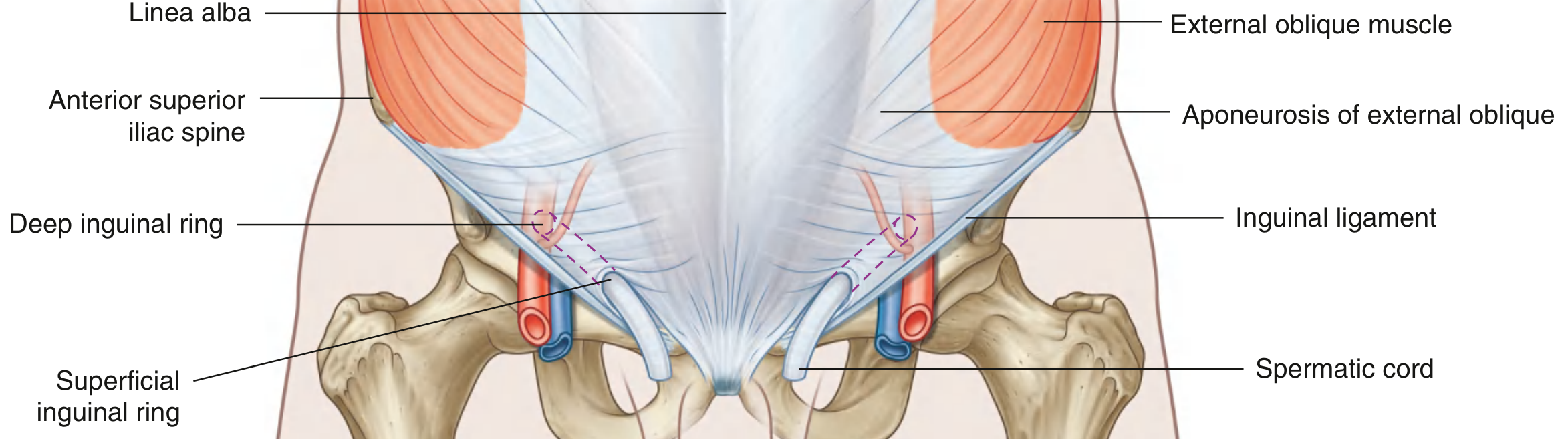
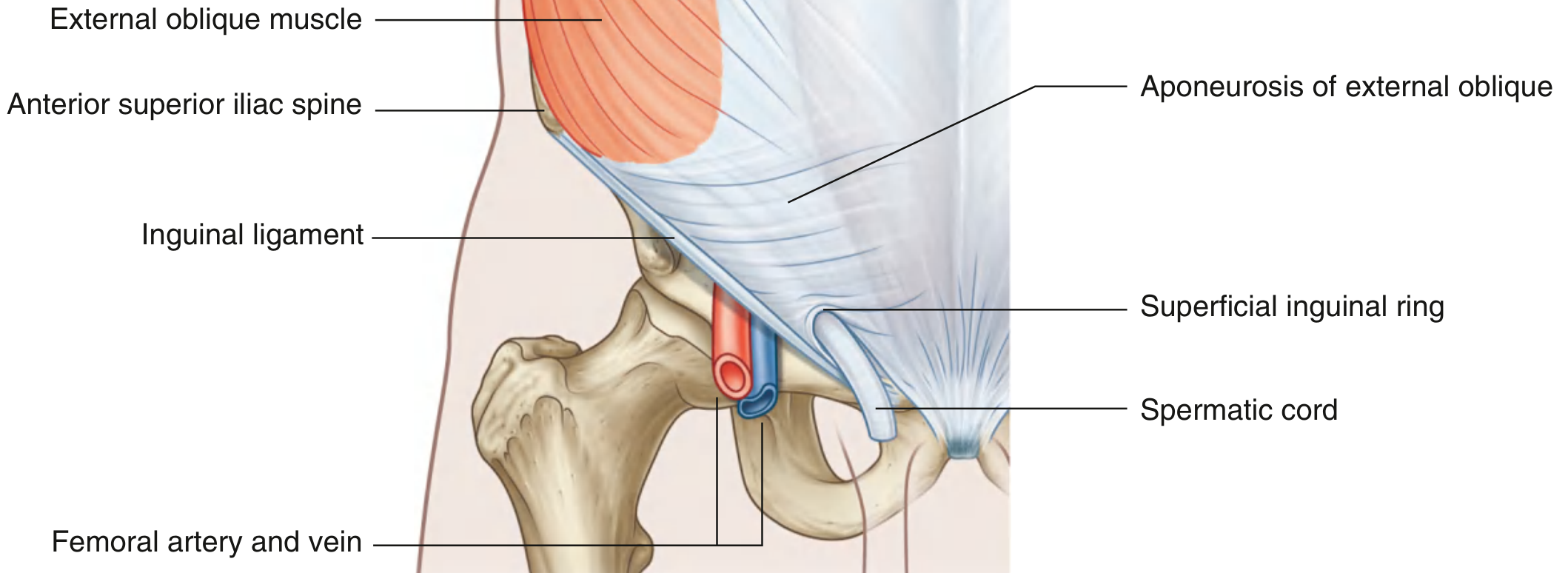
2. Superficial Inguinal Ring (External Inguinal Ring)
Exact Location
"Superior to the pubic tubercle - it is the end of the inguinal canal."
- Gray's Anatomy for Students
"An inverted V-shaped defect in the aponeurosis of the external oblique, lateral to the pubic tubercle."
- Bailey and Love's Short Practice of Surgery, 28th Ed.
(Note: it sits just above AND lateral to the pubic tubercle - the pubic tubercle itself is the key landmark to find it clinically.)
What It Is Made Of
"A triangular opening in the aponeurosis of the external oblique, with its apex pointing superolaterally and its base formed by the pubic crest."
- Gray's Anatomy for Students
Its three sides are:
| Structure | Role |
|---|---|
| Medial crus | Attaches to the pubic symphysis |
| Lateral crus | Attaches to the pubic tubercle |
| Intercrural fibers | Arch across the apex, preventing further widening of the ring |
| Reflected inguinal ligament | Completes the ring internally/inferiorly |
Just like the deep ring, the superficial ring is not merely a hole - it is the start of the tubular evagination of the external oblique aponeurosis over the spermatic cord, forming the external spermatic fascia.
Summary Table
| Feature | Deep (Internal) Ring | Superficial (External) Ring |
|---|---|---|
| Location | Midway between ASIS and pubic symphysis, just above inguinal ligament | Above and lateral to pubic tubercle |
| Made of | Outpouching of transversalis fascia | Triangular gap in external oblique aponeurosis |
| Relation | Immediately lateral to inferior epigastric vessels | Apex held by intercrural fibres; base = pubic crest |
| Gives rise to | Internal spermatic fascia | External spermatic fascia |
| Position in canal | Lateral (entrance) | Medial (exit) |
| Hernia relevance | Indirect inguinal hernia enters here | Hernia or spermatic cord exits here |
Clinical Tip (Bailey & Love)
When examining a suspected hernia, the deep ring is located by finding the ASIS and pubic tubercle, then pressing at the midpoint of the line between them. If pressure at this point controls the hernia on coughing, it is an indirect inguinal hernia (entering through the deep ring). If it is not controlled, it is a direct hernia (bulging medially through the posterior wall, not through the deep ring).

Exact location of femoral ring and what is it made up of?
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Loading Image
Finding Sources
Excellent - all the detail needed is gathered. Here is the complete answer:
The Femoral Ring - Exact Location and Composition
What Is the Femoral Ring?
The femoral ring is the superior (abdominal/extraperitoneal) opening of the femoral canal - the "mouth" through which a femoral hernia protrudes. It is about 1 cm in diameter and is normally plugged by Cloquet's node (a deep inguinal lymph node), fat, and areolar tissue. The ring sits at the upper end of a short cone-shaped funnel (the femoral canal), which extends ~2 cm inferiorly to end at the saphenous opening (fossa ovalis) in the thigh.
Exact Location
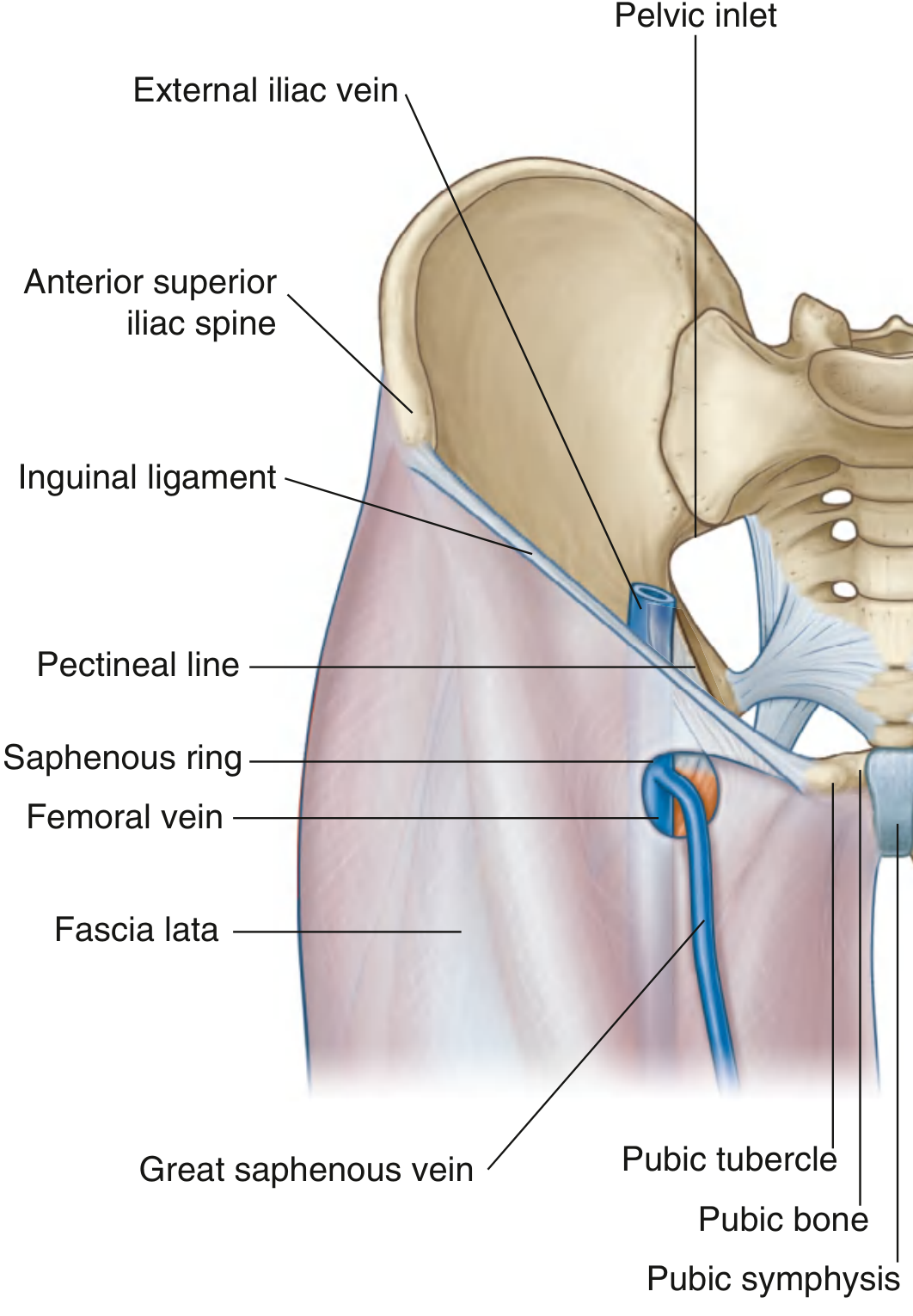
The femoral ring is located:
- Inferior to the inguinal ligament (not above it, unlike inguinal hernias)
- Medial to the femoral vein
- Lateral to the lacunar ligament / pubic tubercle
- At the superomedial corner of the femoral sheath, within the vascular compartment (lacuna vasorum)
The femoral sheath (from lateral to medial) contains: femoral artery | femoral vein | femoral canal (with the ring at its top). The femoral nerve lies lateral to the sheath and is outside it.
Boundaries (What It Is Made Of)
Different authoritative texts converge on this description, with slight variation on the medial wall:
| Wall | Structure |
|---|---|
| Anterior | Inguinal ligament + iliopubic tract |
| Posterior | Pectineal ligament (Cooper's ligament) - a condensation of periosteum on the superior pubic ramus, reinforced by the iliopubic tract |
| Medial | Lacunar ligament (Gimbernat's ligament) - the fan-shaped medial reflection of the inguinal ligament onto the pectineal line |
| Lateral | Femoral vein (separated by the connective tissue septum of the femoral sheath) |
Schwartz's Principles of Surgery, 11th Ed. states: "The borders of the femoral ring include the iliopubic tract and inguinal ligament anteriorly, Cooper's ligament posteriorly, the lacunar ligament medially, and the femoral vein laterally."
Mulholland and Greenfield's Surgery adds a nuance: "The boundaries of the ring are formed medially by the curved edge of the transversus abdominis aponeurosis, not the lacunar ligament, which inserts more medially."
Diagram: Femoral Sheath, Canal and Ring
(Mulholland and Greenfield's Surgery)
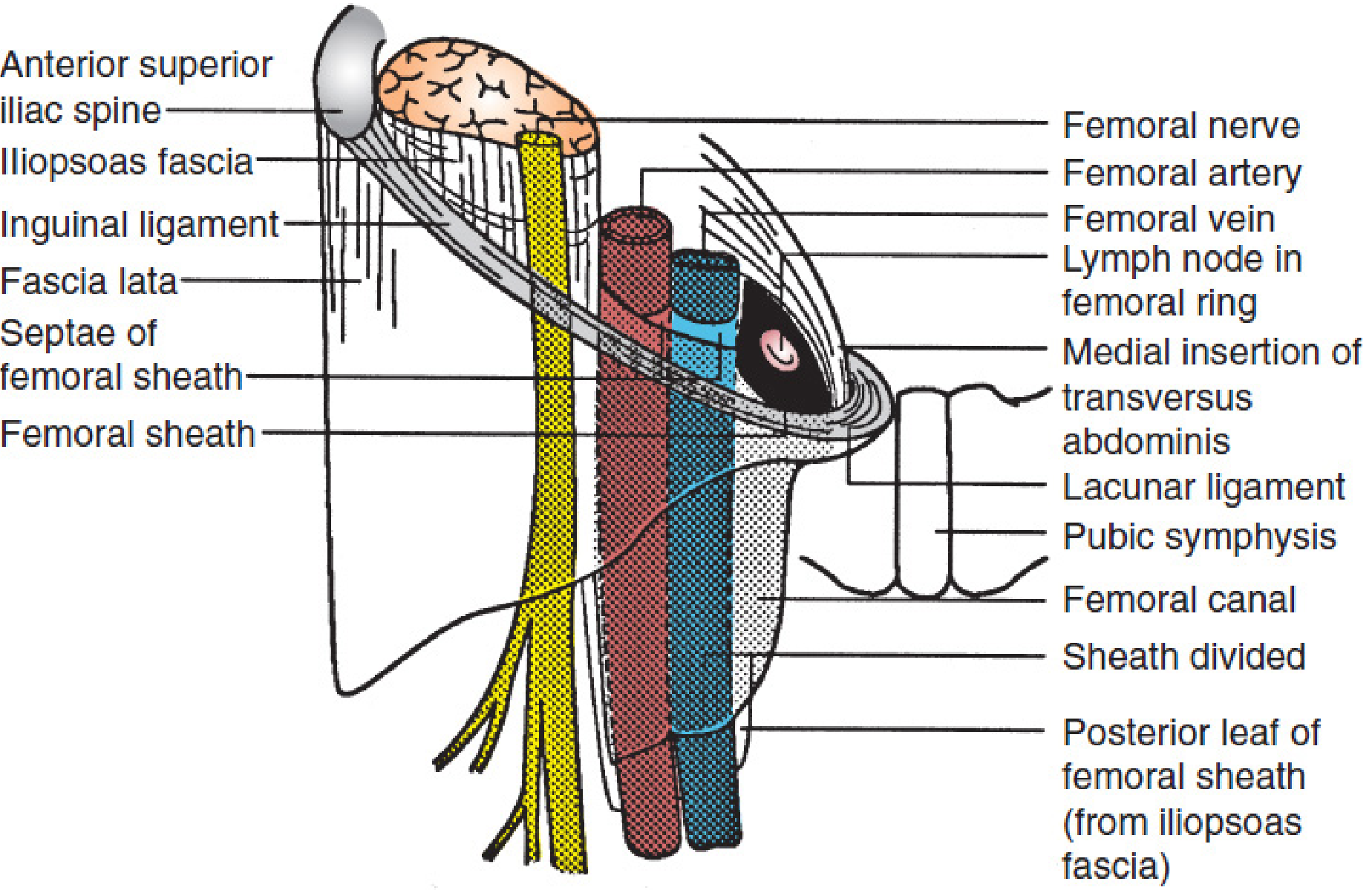
Diagram: Femoral Vein and Ring in Context - Anterior View
(Gray's Anatomy for Students)
Why the Femoral Ring Is Clinically Dangerous
The ring is small and rigid - its walls are unyielding fibrous/ligamentous structures. This means a femoral hernia:
- Has a high risk of incarceration and strangulation
- Cannot be safely enlarged at the time of reduction (especially on the medial side) without risking injury to an anomalous obturator artery - in ~30% of individuals, the obturator artery passes close to or across the lacunar ligament - this variant is historically called the "corona mortis" (crown of death)
- The femoral vein laterally is equally at risk of compression or laceration if sutures are placed incorrectly during repair
Summary
| Feature | Detail |
|---|---|
| Location | Below inguinal ligament, medial to femoral vein, lateral to pubic tubercle |
| Anterior wall | Inguinal ligament + iliopubic tract |
| Posterior wall | Cooper's (pectineal) ligament |
| Medial wall | Lacunar ligament (Gimbernat's) |
| Lateral wall | Femoral vein (connective tissue septum) |
| Normal contents | Cloquet's lymph node, fat, areolar tissue |
| Size | ~1 cm - narrow and rigid |
| Danger | High strangulation risk; anomalous obturator artery medially |
What is patent processus vaginalis?
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Excellent - all key information and images are in hand. Here is the full answer:
Patent Processus Vaginalis (PPV)
1. Embryology - What Is the Processus Vaginalis?
During the third trimester of fetal development, the testis descends from its retroperitoneal position toward the scrotum, guided by the gubernaculum. As it does so, it drags with it a finger-like outpouching of peritoneum - this is the processus vaginalis.
"The peritoneal extension that descends alongside the chorda gubernaculum of the testis is called the processus vaginalis. As the testis descends into the scrotum, the processus vaginalis forms a serous covering around the testis known as the tunica vaginalis."
- Mulholland and Greenfield's Surgery, 7th Ed.
The tunica vaginalis (the double-layered serous covering of the adult testis) is therefore simply the remnant of the lower end of the processus vaginalis, retained around the testis.
Normally, after descent is complete, the processus vaginalis obliterates - the lumen collapses and becomes fibrous, sealing off the peritoneal cavity from the inguinal canal and scrotum.
2. Patent Processus Vaginalis - Definition
When this obliteration fails to occur, the processus vaginalis remains open (patent), creating a persistent communication between the peritoneal cavity and the scrotum/inguinal canal. This is a patent processus vaginalis (PPV).
"If the communication between the tunica vaginalis and the peritoneal cavity fails to close, a persistent processus vaginalis exists."
- The Developing Human: Clinically Oriented Embryology
3. Incidence
| Age | Incidence of PPV |
|---|---|
| Newborn (at autopsy) | 80-94% |
| Adulthood | 20-30% |
| Infants with unilateral hernia, contralateral PPV | ~60% in first months of life |
Importantly:
"A patent processus vaginalis by itself does not constitute a clinical inguinal hernia."
- Mulholland and Greenfield's Surgery
PPV is an anatomical finding; it becomes clinically significant only when peritoneal contents (bowel, fluid, omentum) enter it.
4. Clinical Consequences - What PPV Causes
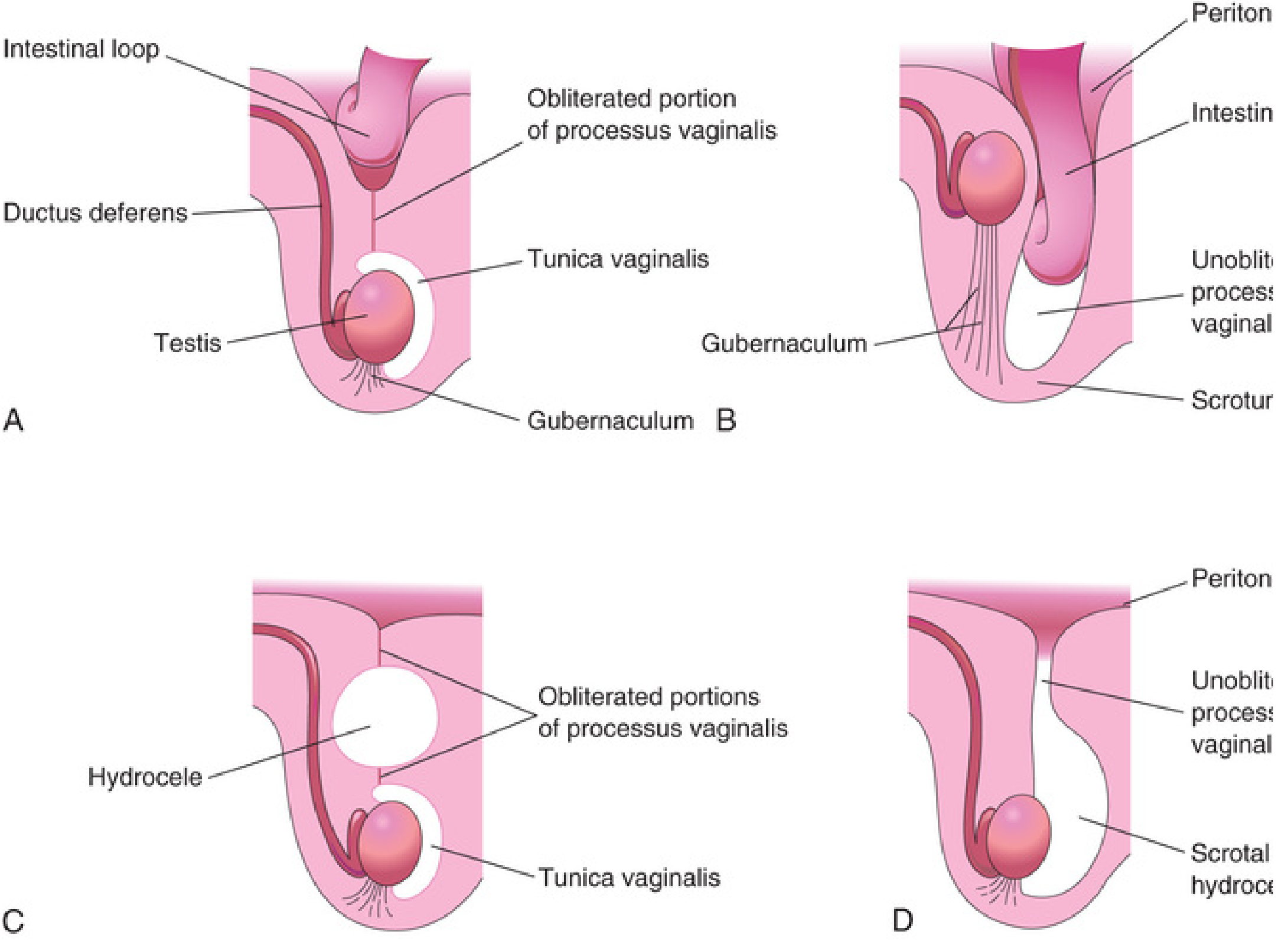
The degree and location of patency determines which condition results:
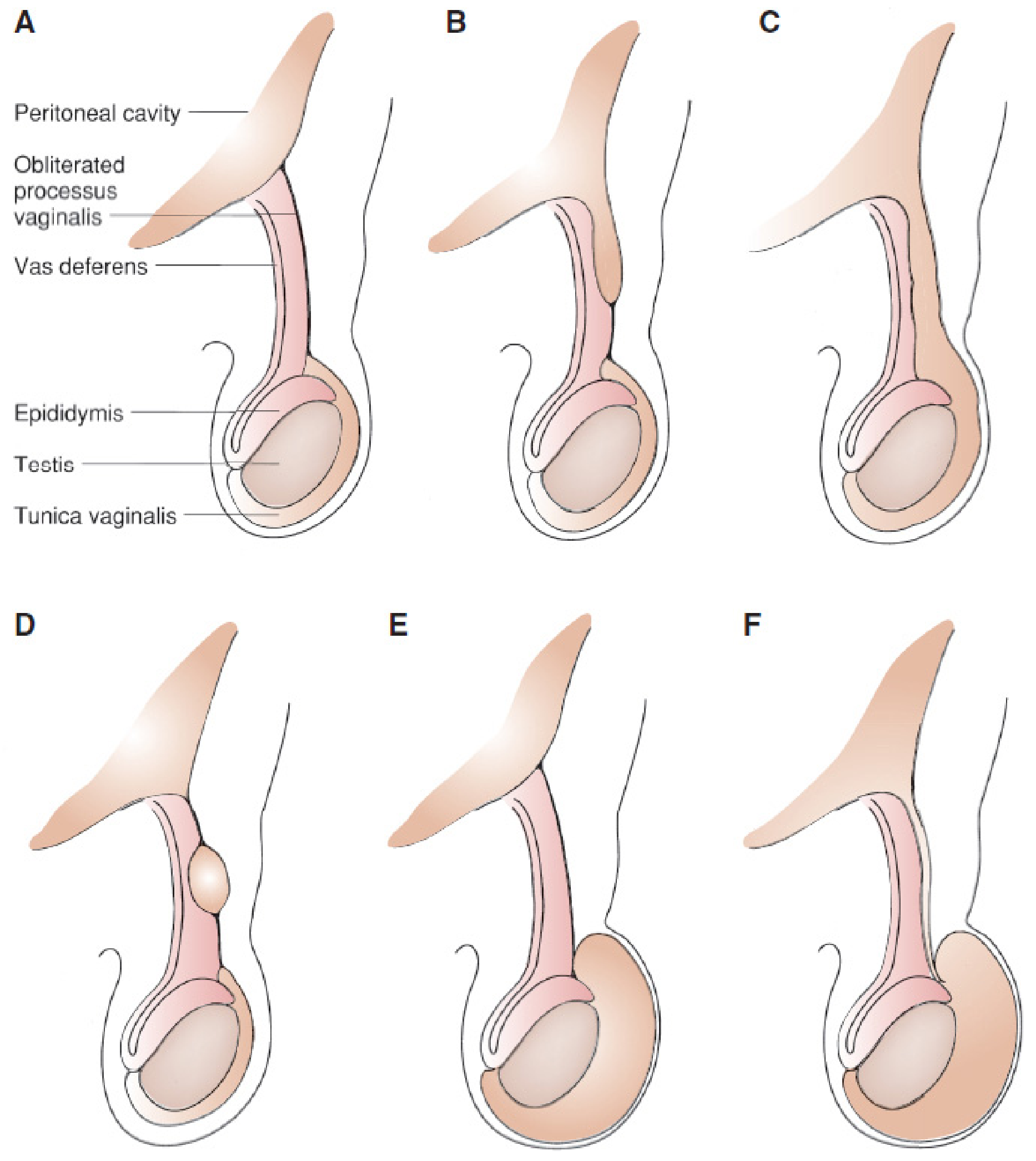
| Panel | Condition | Mechanism |
|---|---|---|
| A | Normal | Processus fully obliterated; tunica vaginalis isolated |
| B | Incomplete indirect inguinal hernia | Proximal part patent (hernia sac within canal only); distal obliterated |
| C | Complete indirect inguinal hernia | Entire processus patent; bowel descends into scrotum |
| D | Hydrocele of the cord | Middle segment patent only; fluid traps in isolated mid-segment |
| E | Non-communicating scrotal hydrocele | Distal end patent but proximal obliterated; fluid pools around testis |
| F | Communicating hydrocele | Full-length PPV, too narrow for bowel but allows peritoneal fluid to flow in/out; size changes with position |
5. The Classic Embryological Diagram
(The Developing Human: Clinically Oriented Embryology)
6. In Females
The processus vaginalis exists in females as the canal of Nuck - a peritoneal diverticulum that accompanies the round ligament through the inguinal canal toward the labia majora. PPV in females leads to:
- Indirect inguinal hernia (often containing ovary + fallopian tube)
- Cyst of the canal of Nuck (analogous to hydrocele of the cord in males)
7. Key Clinical Points
- PPV is the anatomical basis for ALL indirect inguinal hernias in children (99% of pediatric inguinal hernias are indirect)
- More common on the right side (3:1) - because the right testis descends later, delayed by the developing IVC
- Male:female ratio = 6:1 for clinical inguinal hernia
- Premature infants have higher rates (~13% at <32 weeks, ~30% at <1 kg birth weight)
- Surgical treatment is high ligation of the hernia sac (processus vaginalis) at the internal ring - not tissue repair, because the posterior wall is normal in children
Anterior abdominal wall muscles and their fibres direction and role in surgery
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Finding Sources
Loading Image
Loading Image
All the key anatomy and surgical diagrams are collected. Here is the complete answer:
Anterior Abdominal Wall Muscles: Fibre Directions and Surgical Relevance
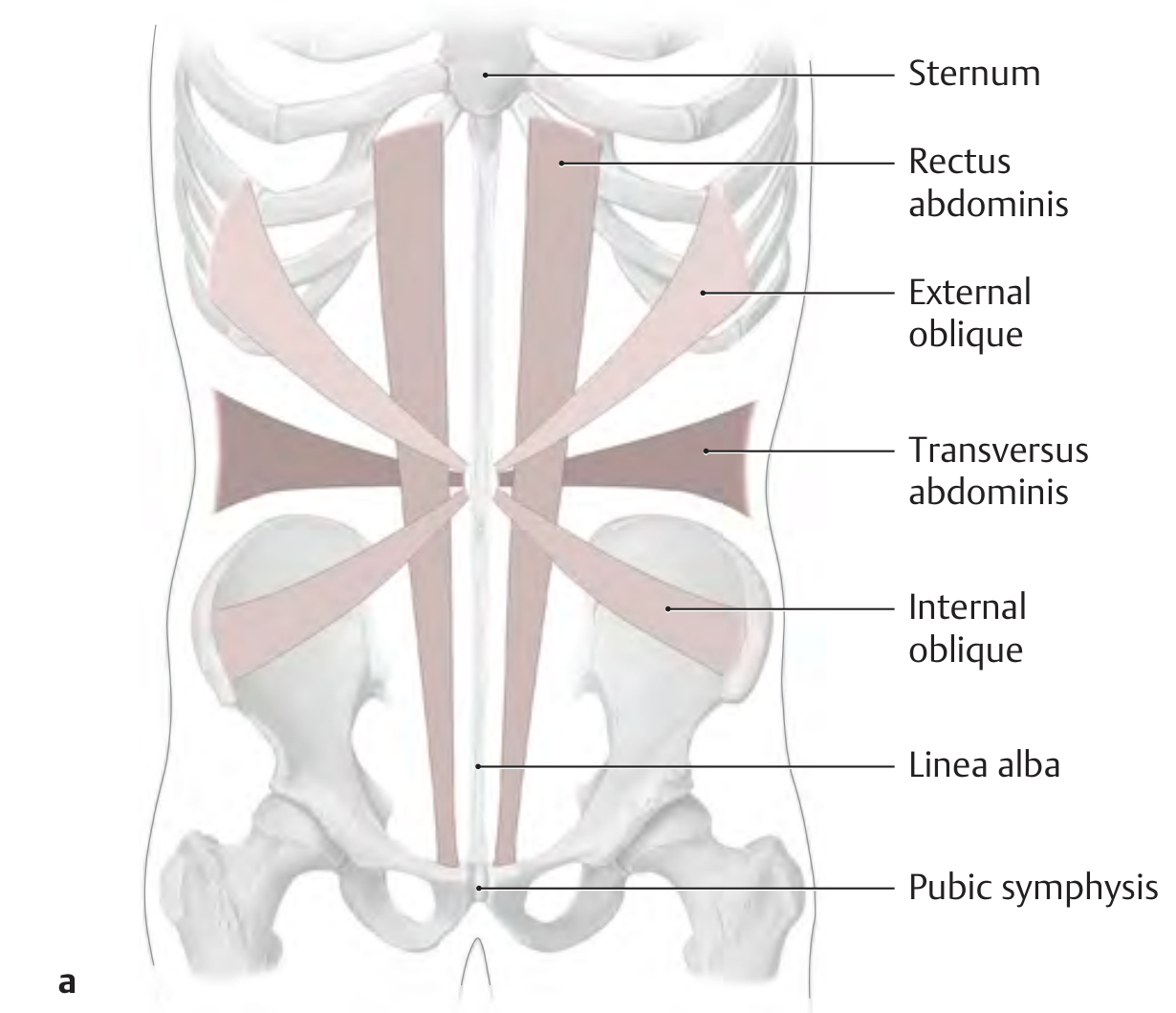
Overview Diagrams
Fibre directions of all 4 muscle groups - anterior view:
(Thieme Atlas of Anatomy)
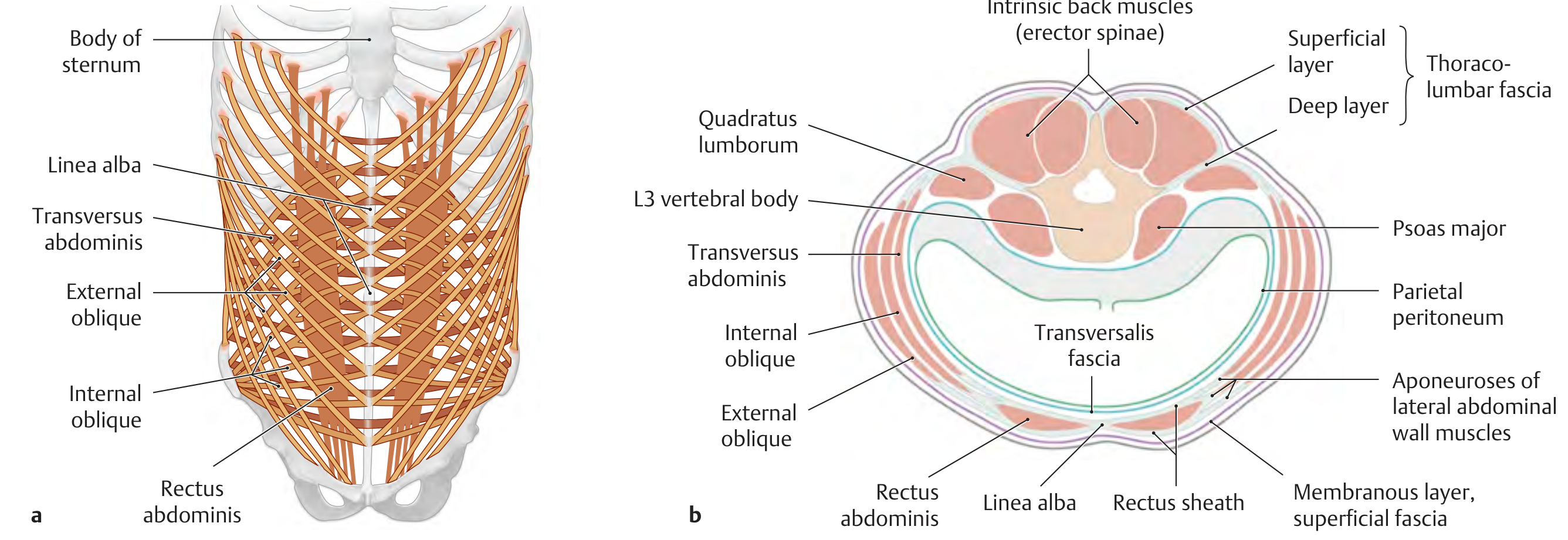
Layered anatomy with rectus sheath - transverse section at L3:
(Thieme Atlas of Anatomy)
The Five Muscles
1. External Oblique (EO)
| Feature | Detail |
|---|---|
| Layer | Most superficial flat muscle |
| Origin | Outer surfaces of ribs 5-12 |
| Insertion | Linea alba, inguinal ligament, pubic tubercle, iliac crest |
| Fibre direction | Downward and medially - "hands in pockets" direction |
| Aponeurosis | Broad, fused below inguinal ligament; forms the superficial inguinal ring at its gap above pubic tubercle |
| Innervation | T5-T12 (intercostal nerves) |
Surgical relevance:
- The inguinal ligament is the rolled-over free inferior edge of the EO aponeurosis
- The superficial inguinal ring is a V-shaped gap in the EO aponeurosis
- In a gridiron (muscle-splitting) incision for appendicectomy, the EO aponeurosis is split in the line of its fibres (obliquely downward-medial)
- In a Pfannenstiel incision, the EO aponeurosis is incised transversely, then reflected off the rectus
- Cutting against fibre direction risks denervation of the underlying internal oblique
2. Internal Oblique (IO)
| Feature | Detail |
|---|---|
| Layer | Middle flat muscle |
| Origin | Thoracolumbar fascia, iliac crest, lateral inguinal ligament |
| Insertion | Ribs 10-12, linea alba (via anterior + posterior rectus sheath), pubic crest |
| Fibre direction | Upward and medially - roughly perpendicular to EO, at ~90° to it |
| Innervation | T7-T12, L1 (iliohypogastric, ilioinguinal) |
Surgical relevance:
- Lower fibres of IO arch over the deep inguinal ring together with transversus abdominis, descending to form the conjoint tendon (inguinal falx) at the pubic tubercle
- The cremaster muscle is a continuation of IO fibres over the spermatic cord
- In gridiron incision, IO is split along its fibres (upward-medially); the two muscles (EO and IO) are split in different directions, which is the basis of the self-retaining nature of the incision
- Damage to L1 branches here causes chronic groin pain post-inguinal hernia repair
3. Transversus Abdominis (TA)
| Feature | Detail |
|---|---|
| Layer | Deepest flat muscle |
| Origin | Inner surfaces of ribs 7-12, thoracolumbar fascia, iliac crest, lateral inguinal ligament |
| Insertion | Linea alba, pubic crest, pectineal line |
| Fibre direction | Horizontal (transverse) - runs directly across the abdomen |
| Innervation | T7-T12, L1 |
Surgical relevance:
- Aponeurosis contributes to the posterior rectus sheath above the arcuate line
- Below the arcuate line its aponeurosis swings to the anterior rectus sheath (all three aponeuroses are anterior to rectus below this line)
- Forms the transversalis fascia where it continues as a fascial layer medially - this is the direct investing layer of the peritoneum and the layer the deep inguinal ring passes through
- In the transversus abdominis release (TAR) procedure for complex hernia repair, this muscle's posterior sheath is divided laterally to allow fascial advancement and tension-free midline closure
- Splitting TA in the line of its fibres gives access to the retroperitoneal/preperitoneal space (used in laparoscopic hernia repair - TEP, TAPP)
4. Rectus Abdominis
| Feature | Detail |
|---|---|
| Layer | Paired vertical strap muscles flanking the midline |
| Origin | Pubic symphysis and pubic crest |
| Insertion | Costal cartilages of ribs 5-7 and xiphoid process |
| Fibre direction | Vertical |
| Special features | 3 tendinous intersections (at xiphoid, umbilicus, midway) firmly adherent to anterior sheath but NOT posterior sheath |
| Innervation | T5-T12 (segmental intercostal nerves entering laterally) |
Surgical relevance:
- Midline (median) laparotomy - incision through the avascular linea alba avoids cutting any muscle
- Paramedian incision - incises the anterior rectus sheath longitudinally, retracts the rectus laterally, and enters through the posterior sheath; good strength on closure
- The rectus can be split longitudinally (not preferred - devascularises and denervates medial segment)
- A TRAM/DIEP flap uses rectus abdominis (with its superior/inferior epigastric blood supply) for breast reconstruction
- Tendinous intersections explain why haematomas within the rectus sheath are limited to one segment above the umbilicus
5. Pyramidalis
| Feature | Detail |
|---|---|
| Origin | Pubis (anterior to rectus insertion) |
| Insertion | Linea alba |
| Fibre direction | Vertical - runs within the rectus sheath inferior to umbilicus |
| Innervation | Subcostal nerve T12 |
| Note | Absent in 10-25% of people |
Surgical relevance: Identifies the midline (linea alba) during lower abdominal incisions - the muscle runs toward it like a pointer. Absent in some patients, which is not pathological.
The Rectus Sheath - Key Surgical Structure
Formed by the aponeuroses of all three flat muscles splitting and reuniting around the rectus abdominis. Its composition changes at the arcuate line (halfway between umbilicus and pubis):
(Fischer's Mastery of Surgery - transverse and sagittal sections)
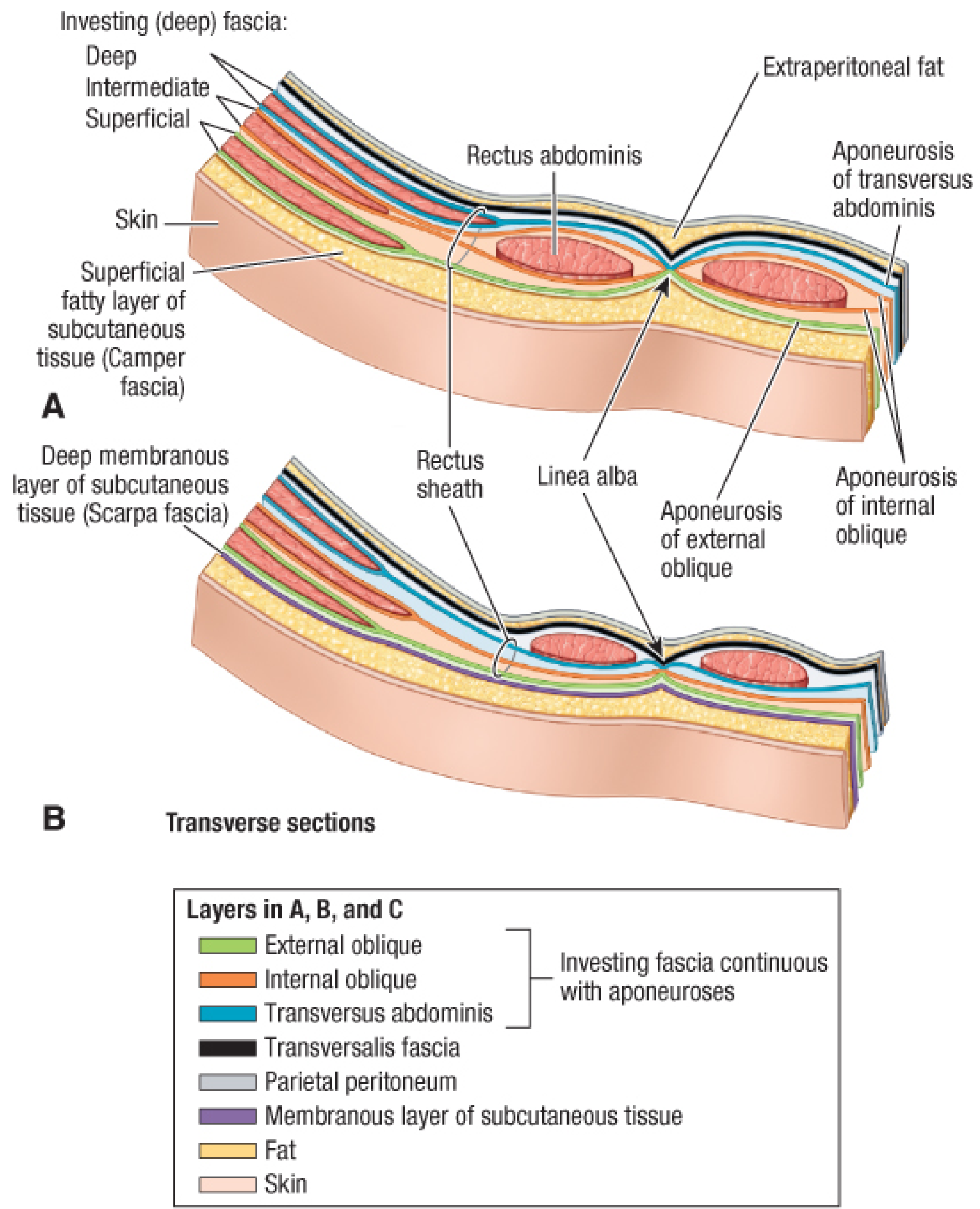
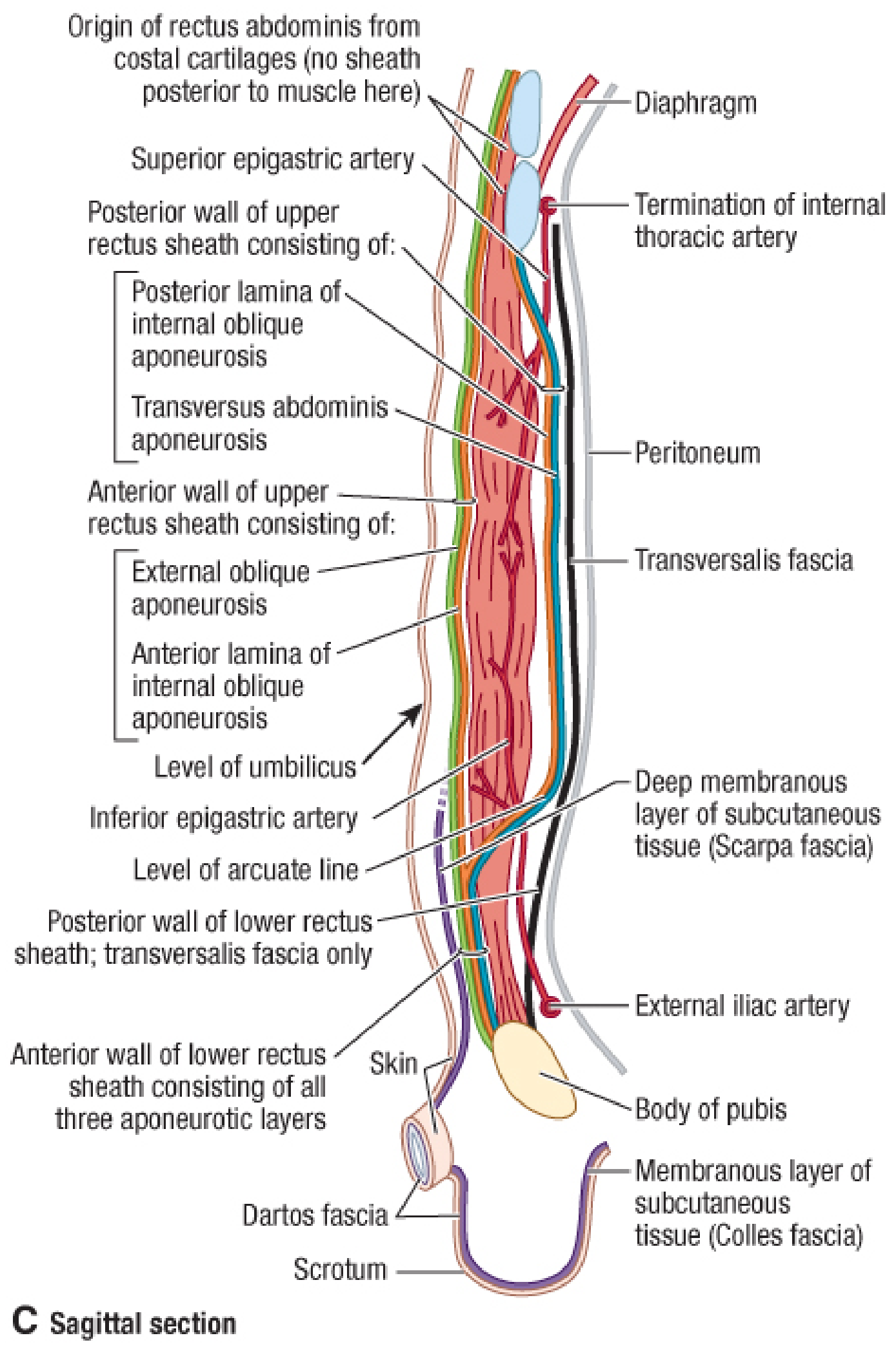
| Level | Anterior Rectus Sheath | Posterior Rectus Sheath |
|---|---|---|
| Above arcuate line | EO aponeurosis + anterior lamina of IO | Posterior lamina of IO + TA aponeurosis |
| Below arcuate line (arcuate to pubis) | All three aponeuroses (EO + IO + TA) | Transversalis fascia only |
Clinical pearl: Below the arcuate line, the posterior rectus sheath is absent. A haematoma or abscess below this level can spread freely in the preperitoneal space. This is also why incisional hernias below the arcuate line are more difficult to repair with direct tissue closure.
Surgical Incisions and Their Muscle Relationship

| Incision | Muscles Encountered | Technique | Advantage |
|---|---|---|---|
| Midline laparotomy | None (linea alba only) | Cut avascular linea alba | Fast; minimal bleeding; excellent exposure |
| Paramedian | Anterior rectus sheath incised; rectus retracted | Posterior sheath + peritoneum opened | Strong closure; nerve supply preserved |
| Gridiron (McBurney) | EO, IO, TA split in line of fibres | Each split in different directions | Self-retaining; low hernia risk |
| Pfannenstiel | EO aponeurosis cut transversely; rectus separated | Peritoneum opened vertically | Cosmetic; low hernia; used in Caesarean |
| Kocher (subcostal) | EO, IO, TA divided transversely | Cuts across fibres | Good liver/biliary access |
| Lanz | Transverse skin; EO split obliquely, IO + TA split | Fibre-splitting lateral muscles | Better cosmesis for appendicectomy |
This is a shared conversation. Sign in to Orris to start your own chat.