Neonatal sepsis
Reading File
Finding Sources
Searching PubMed
"neonatal sepsis" diagnosis management
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full response.
Neonatal Sepsis
Definition & Overview
Neonatal sepsis is the most common cause of neonatal cardiorespiratory distress and refers to a systemic bacterial infection in the first 28 days of life. Neonates have approximately twice the risk of serious bacterial infection compared to infants 4-8 weeks of age, owing to developmental immunologic deficiencies - depressed cell-mediated immunity, diminished B-cell function, and low immunoglobulin levels (maternal IgG reaches its nadir at 2-3 months of age).
- Tintinalli's Emergency Medicine, p. 773
- Miller's Anesthesia, p. 11455
Classification: Early-Onset vs. Late-Onset
| Feature | Early-Onset Sepsis (EOS) | Late-Onset Sepsis (LOS) |
|---|---|---|
| Timing | First 7 days of life (typically <48h) | After 1 week of age |
| Onset | Fulminant | More gradual |
| Associations | Maternal fever, GBS-positive vaginal swabs, prolonged ROM, fetal distress | Less linked to maternal risk factors |
| Complications | Septic shock, neutropenia | Meningitis (more common) |
| Pathogenesis | In utero infection | Acquired at or soon after birth |
- Tintinalli's Emergency Medicine, p. 773
Causative Organisms
The pathogens reflect organisms colonizing the female genital tract and caregiver nasal mucosa:
-
Group B Streptococcus (GBS) - most common bacterial pathogen; causes severe cardiorespiratory instability and meningitis in 30% of cases. By 2-3 weeks of age, more commonly associated with meningitis than pulmonary disease.
-
Escherichia coli - second most common, especially in preterm neonates
-
Listeria monocytogenes - causes early-onset sepsis (in utero infection, diagnosed within 48h) and late-onset meningitis (~2 weeks of age, full-term infants)
-
Klebsiella spp., Enterobacter spp., Haemophilus influenzae
-
Gram-positive cocci (beta-hemolytic streptococci)
-
Herpes simplex virus - particularly fulminant; active lesions in the birth canal are an indication for caesarean section
-
TORCH pathogens - can mimic bacterial sepsis when CNS depression, circulatory collapse, or thrombocytopenia occurs
-
Miller's Anesthesia, p. 11455
-
Rosen's Emergency Medicine, p. 1714
Clinical Features
Clinical signs are non-specific and localizing signs may be absent (e.g., nuchal rigidity and Kernig/Brudzinski signs are present in only a minority of neonates with meningitis).
Key signs (Table 116-3, Tintinalli's):
- Temperature instability - fever (rectal ≥38°C/100.4°F) or hypothermia (<36.5°C/97.7°F)
- CNS dysfunction - lethargy, irritability, seizures
- Respiratory distress - apnea, tachypnea, grunting
- Feeding disturbance - vomiting, poor feeding, gastric distension, diarrhea
- Jaundice
- Rashes or petechiae
- Metabolic - hypoglycemia, metabolic acidosis
- Circulatory - poor cutaneous perfusion, hypotension
Note: Tachypnea and respiratory distress can be a sign of sepsis, meningitis, or UTI alone. The threshold for a full sepsis workup is lower in neonates than older infants.
Differential Diagnosis
Other causes of critical illness in neonates that can mimic sepsis include:
-
Congenital heart disease (ductal-dependent lesions presenting in the first week with shock as the duct closes - easily mistaken for sepsis)
-
Inborn errors of metabolism
-
Congenital adrenal hyperplasia
-
Intracranial hemorrhage
-
Abdominal catastrophe (malrotation/volvulus, NEC)
-
Tintinalli's Emergency Medicine, p. 773
Risk Factors for EOS
Maternal/perinatal risk factors:
- Maternal GBS colonization (positive vaginal swabs)
- Maternal fever / chorioamnionitis
- Prolonged rupture of membranes
- Fetal distress
- Prematurity (≤34 weeks especially high risk)
- Preterm labor, cervical insufficiency, prelabor ROM
- Inadequate intrapartum antibiotic prophylaxis (IAP)
Infants at lower EOS risk (if all present): delivery for maternal indications (pre-eclampsia, placental insufficiency), mother not in labor, no labor induction, no ROM prior to delivery, and delivery by caesarean section.
- Red Book 2021, p. 1103-1104
Investigations
A full sepsis workup includes:
- Blood cultures (only ~50% of suspected septic neonates have positive cultures)
- Urine culture
- CSF analysis and culture - lumbar puncture is part of the standard workup; should be considered in clinically ill infants when GBS EOS is highly suspected (unless procedure would compromise clinical condition)
- CBC with differential (neutropenia is a marker of early-onset disease)
- CRP, metabolic panel, glucose
Note on molecular assays: A 2025 Cochrane review (PMID 40105375) evaluated molecular assays (PCR-based) for neonatal sepsis diagnosis, reflecting ongoing interest in improving sensitivity beyond culture-based methods.
Treatment
Antibiotic Therapy
Standard empiric regimen:
- Ampicillin 50-100 mg/kg IV (covers GBS, Listeria, Enterococcus)
- Gentamicin (aminoglycoside) 2.5-4 mg/kg IV (covers E. coli and other gram-negatives)
Modifications:
- If gram-negative meningitis is strongly suspected: replace gentamicin with cefotaxime or ceftazidime 50 mg/kg (better CNS penetration)
- Avoid ceftriaxone in neonates - can displace bilirubin from albumin and cause kernicterus
- Add IV acyclovir if: maternal history of herpes, suspicious CSF findings (lymphocyte and RBC predominance on non-traumatic LP), or any ill-appearing neonate
Key principle: All neonates with suspected sepsis should be admitted and started on IV antibiotics. Do not wait for culture results.
- Tintinalli's Emergency Medicine, p. 774
- Rosen's Emergency Medicine, p. 1714
GBS Prevention (Intrapartum Antibiotic Prophylaxis)
Maternal IAP (penicillin/ampicillin intrapartum) is the primary prevention strategy for GBS EOS. GBS was first recognized as a cause of early-onset neonatal sepsis in the 1970s; by the 1990s it was a leading cause of serious neonatal infection. Widespread IAP has significantly reduced its incidence.
- Creasy & Resnik's Maternal-Fetal Medicine
Recent Evidence (2025)
- A 2025 meta-analysis (PMID 40555905) reviewed antibiotic strategies for neonatal sepsis, highlighting efficacy concerns and emerging antimicrobial resistance patterns - an important clinical consideration when selecting empiric regimens.
- A 2025 Cochrane review (PMID 40105375) assessed molecular (PCR) assays for neonatal sepsis diagnosis, providing updated data on their diagnostic accuracy as alternatives to blood culture.
Summary Points
- Sepsis is the most common cause of neonatal cardiorespiratory distress; fever OR hypothermia should prompt evaluation
- Early-onset (<7 days) is fulminant and maternally acquired; late-onset (>7 days) is more insidious and more commonly causes meningitis
- GBS and E. coli are the dominant pathogens; Listeria requires ampicillin coverage
- Clinical signs are non-specific - maintain a low threshold for full workup and empiric treatment
- Standard empiric therapy: ampicillin + gentamicin; avoid ceftriaxone; add acyclovir when herpes is possible
- Only ~50% of suspected cases yield positive cultures
Neonatal seizures
Finding Sources
Searching PubMed
"neonatal seizures" treatment management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"neonatal seizures" phenobarbital levetiracetam
Reading File
Loading Image
Reading File
Reading File
I now have rich, multi-source content covering all aspects of neonatal seizures. Let me compile the comprehensive answer.
Neonatal Seizures
Overview
Neonatal seizures are the most common neurological emergency in the first 28 days of life and represent one of the most common manifestations of neonatal brain injury. They are more common in the first 28 days than at any other time of life. Unlike seizures in older children and adults (where unprovoked, epileptic seizures predominate), neonatal seizures are almost always acute symptomatic - driven by an underlying brain insult.
- Bradley and Daroff's Neurology in Clinical Practice, p. 2854
Pathophysiology
The neonatal brain has a fundamental developmental vulnerability that drives its high seizure susceptibility:
The GABA Paradox (NKCC1/KCC2 imbalance):
- In adult neurons, GABA-A receptor activation causes chloride influx → membrane hyperpolarization → inhibition
- In immature neurons, there is net chloride efflux with GABA-A activation → membrane depolarization → excitation
- This is because the chloride exporter KCC2 (which maintains low intracellular Cl⁻) is immature. The importer NKCC1 dominates instead, keeping intracellular chloride high.
- As the neonate matures, KCC2 expression becomes dominant, reversing this effect.
Key clinical implication: This reversal of GABA function is why GABA-agonist anticonvulsants like phenobarbital may have disappointing efficacy in neonates - the drug is activating a system that is paradoxically excitatory.
Consequences of prolonged seizures:
- Neuronal injury via disturbances in cerebral energy metabolism and excitotoxicity
- Recurrent shorter seizures → long-term morphological/physiological deficits including suppression of neuronal stem cells
- Independent association with further hypoxic-ischemic brain injury (MR spectroscopy) and later neurodevelopmental impairment
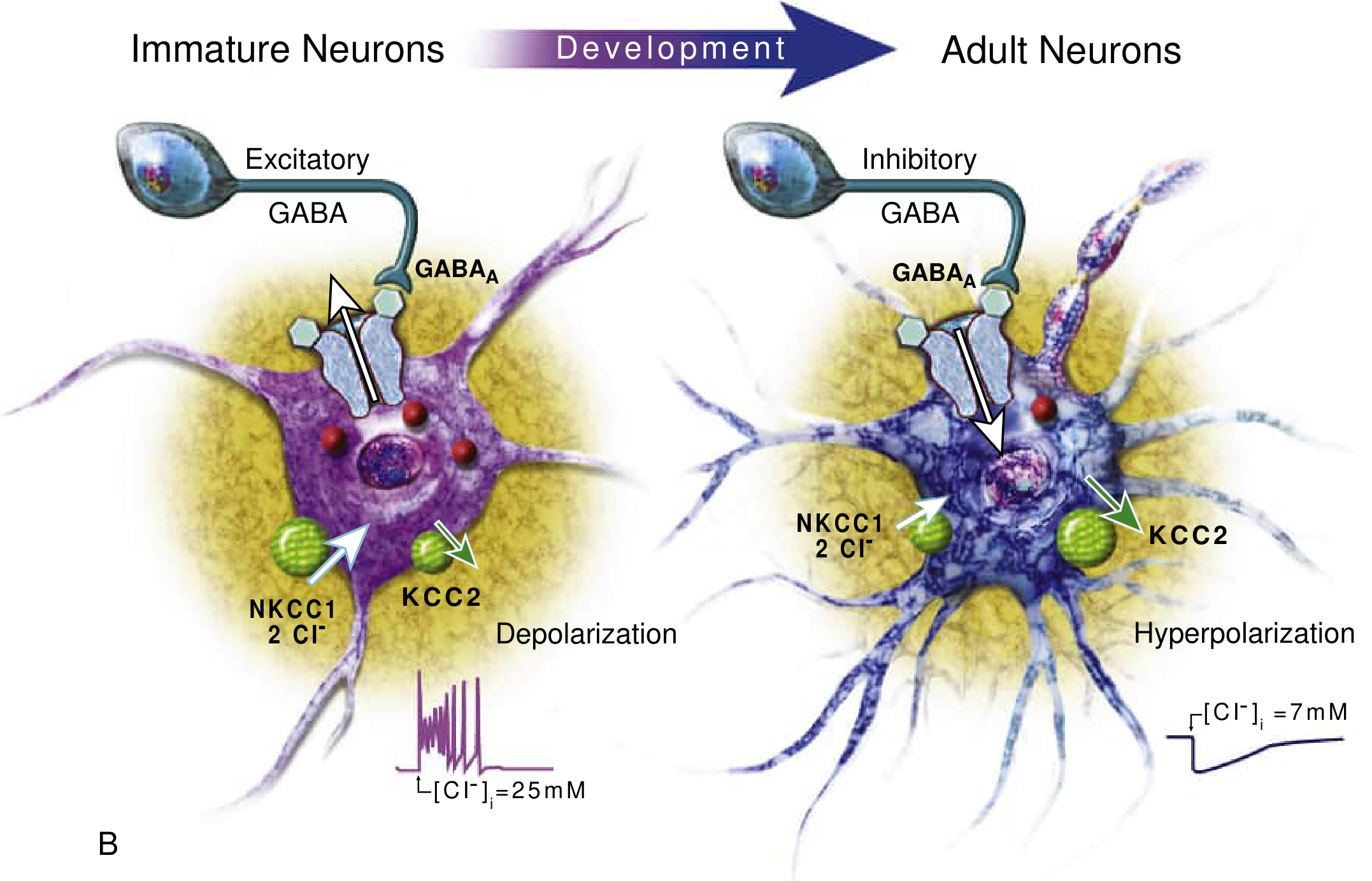
Fig. 110.3 - Developmental alterations of chloride levels, the GABA channel, and chloride cotransporters. GABA depolarizes immature neurons (excitatory) and hyperpolarizes adult ones (inhibitory).
- Bradley and Daroff's Neurology in Clinical Practice, p. 2854-2855
Etiology
Most neonatal seizures are acute symptomatic; the remainder relate to developmental brain abnormalities and genetic neonatal epilepsy syndromes.
Causes by timing of onset:
| Onset | Most Likely Causes |
|---|---|
| Day 0-1 | Hypoxic-ischemic encephalopathy (HIE), birth trauma, severe hypoglycemia |
| Day 1-3 | Hypocalcemia, metabolic disorders, inborn errors of metabolism |
| Day 3-7 | Infection (bacterial meningitis, HSV), infarction, metabolic |
| >1 week | Infection, genetic/metabolic epilepsy syndromes |
Major etiologies:
- Hypoxic-Ischemic Encephalopathy (HIE) - accounts for ~50% of neonatal seizures in term newborns; ~30% in preterm (where intracranial hemorrhage is equally common)
- Intracranial hemorrhage - accounts for ~30% in preterm newborns
- Metabolic:
- Hypoglycemia (most frequent metabolic cause)
- Hypocalcemia (tetany; now less common)
- Hyponatremia, hypomagnesemia
- Pyridoxine (B6) deficiency - rare but treatable; responds to IV pyridoxine 100 mg; may even cause in utero seizures
- Biotinidase deficiency
- Nonketotic hyperglycinemia, maple syrup urine disease, other inborn errors
- CNS infection - meningitis (GBS, E. coli, Listeria), HSV encephalitis
- Structural/Congenital CNS abnormalities - 5-10% of cases; dysplasia (seizures often refractory)
- Perinatal stroke - focal clonic seizures in a term newborn are most commonly associated with focal cerebral infarction
- Drug withdrawal - maternal narcotics
- Non-accidental trauma
- Bradley and Daroff's Neurology in Clinical Practice, p. 2855-2856
- Adams and Victor's Principles of Neurology, p. 352
Neonatal Epilepsy Syndromes
These are genetic conditions distinct from acute symptomatic seizures:
-
Benign Familial Neonatal Epilepsy (BFNE) - autosomal dominant; mutations in voltage-gated K⁺ channels KCNQ2, KCNQ3 (also SCN2A); onset first week of life; seizures remit within first year; normal neurodevelopment
-
Benign Neonatal Seizures ("fifth-day fits") - clonic convulsions starting days 2-7; discontinuous theta on EEG; good prognosis, rarely recur
-
Ohtahara Syndrome - severe epileptic encephalopathy; intractable tonic seizures + burst-suppression on EEG; caused by increasing number of genetic mutations; may evolve into West or Lennox-Gastaut syndromes
-
Early Myoclonic Encephalopathy - erratic focal myoclonus shifting asynchronously, burst suppression on EEG
-
Pyridoxine-dependent epilepsy (antiquitin/ALDH7A1 deficiency) - responds to pyridoxal phosphate + folinic acid; biomarkers: elevated urinary α-aminoadipic semialdehyde (AASA) and CSF pipecolic acid
-
Bradley and Daroff's Neurology in Clinical Practice, p. 2855
Clinical Features and Semiology
Neonatal seizures are often subtle, focal, and clinically silent. The immature brain prevents organized generalized tonic-clonic activity and limits bihemispheric spread.
Classification (Volpe):
| Type | Manifestations | Key Points |
|---|---|---|
| Subtle | Eye deviation, blinking, fixed stare; lip-smacking, tongue movements; apnea; bicycling, swimming limb movements | ~50% of all neonatal seizures |
| Clonic (focal/multifocal) | Rhythmic movements of muscle groups | Fast + slow component; often suggests focal pathology |
| Tonic (focal/generalized) | Sustained flexion or extension | May not have electrographic correlate |
| Myoclonic | Synchronous flexion jerks | Must distinguish from physiological myoclonus |
Important: Only one-third of neonatal EEG seizures had clinical signs on simultaneous video; only one-third of those were recognized by experienced staff; and only one-quarter of clinically suspected seizures had electrographic confirmation. This bidirectional unreliability mandates EEG monitoring.
- Bradley and Daroff's Neurology in Clinical Practice, p. 2857
- Tintinalli's Emergency Medicine
- Adams and Victor's Principles of Neurology
Distinguishing Seizures from Non-Epileptic Events
| Feature | Seizures | Jitteriness |
|---|---|---|
| Stimulus sensitivity | No | Yes (exaggerated startle) |
| Ocular movements | Yes (deviation, nystagmus) | Absent |
| Autonomic changes | Tachycardia, hypertension, apnea | Absent |
| Movement character | Clonic = fast + slow component | Tremor = equal rate + amplitude |
| Passive flexion | Seizure continues | Jitteriness stops |
Other mimics: physiological myoclonus, hyperekplexia (exaggerated startle, glycine neurotransmission mutations)
Electroencephalography
Continuous conventional EEG is the gold standard (ACNS guidelines). Key EEG criteria for neonatal seizures:
- Sudden electrographic change
- Repetitive waveforms evolving in morphology, frequency, and/or location
- Amplitude ≥2 μV
- Duration ≥10 seconds
aEEG (amplitude-integrated EEG) - simplified bedside trend monitor; less sensitive than full EEG but interpretable by trained bedside staff. A cornerstone of modern neonatal neurocritical care.
Uncoupling - clinical manifestations terminate while electrographic seizures persist; common after anticonvulsant administration and may lead to undertreatment.
Burst-suppression pattern (high-voltage bursts alternating with voltage suppression) indicates serious injury; must be distinguished from the normal trace-alternant pattern of quiet sleep in term infants.
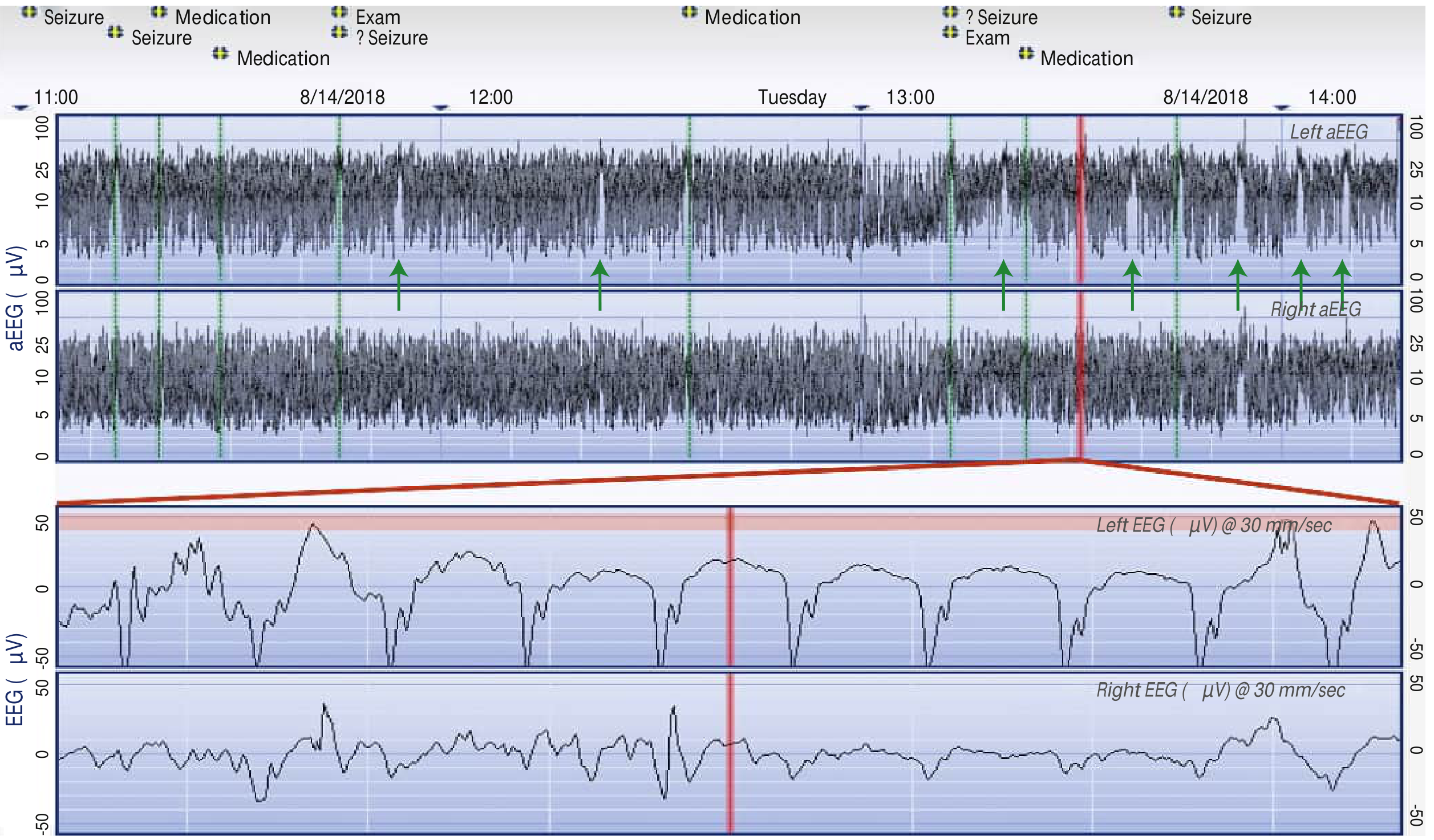
Fig. 110.1 - Amplitude-integrated EEG (aEEG) of a neonate demonstrating seizures. Repetitive sudden rise in the lower margin of the aEEG trace corresponds to seizures on the raw EEG. Events appearing as seizures on aEEG but not marked in real time are shown by green arrows.
- Bradley and Daroff's Neurology in Clinical Practice, p. 2857
Investigations
A broad workup is required for all neonates with witnessed seizures:
Metabolic/labs:
- Blood glucose (treat hypoglycemia immediately)
- Electrolytes: Na⁺, K⁺, Cl⁻, HCO₃⁻, BUN, creatinine
- Calcium, magnesium
- CBC with differential
- Lactic acid, ammonia, serum amino acids, urine organic acids (for inborn errors of metabolism)
Microbiological:
- Blood, urine, CSF cultures
- CSF: cell count, protein, glucose, HSV PCR
- LP should be performed (meningitis is not clinically reliable to exclude in young infants)
Neuroimaging:
- Head CT if non-accidental trauma, hemorrhage, or infarction suspected
- MRI is preferred for structural assessment once stabilized
- Bedside head ultrasound if neonate is unstable (to screen for neurosurgical emergency)
Toxicology: If maternal narcotic use or withdrawal is suspected
Genetics/Metabolic: Genetic testing increasingly important for neonatal epilepsy syndromes
- Rosen's Emergency Medicine, p. 1262
- Tintinalli's Emergency Medicine, p. 2678
Treatment
Step 1: Treat Reversible Causes Immediately
- Hypoglycemia: IV dextrose (D10W 2-4 mL/kg)
- Hypocalcemia: IV calcium gluconate
- Hypomagnesemia: IV magnesium sulfate
- Hyponatremia: Correct cautiously
Step 2: Antiepileptic Drugs
First-line: Phenobarbital
- Standard first-line agent for neonatal seizures
- Loading dose IV; maintenance dosing follows
- Limitation: Growing evidence of phenobarbital-induced neuronal apoptosis even with a single dose, and evidence of memory/learning difficulties in animal models. This has prompted investigation of alternatives.
Second-line: Fosphenytoin / Phenytoin
- If seizures continue after phenobarbital loading
Refractory seizures:
- Benzodiazepine infusion (lorazepam, midazolam)
- Levetiracetam (see note below)
Empiric treatment for suspected metabolic epilepsy (unknown etiology):
- Pyridoxine 15-30 mg/kg/day (max 500 mg/day) IV, can repeat over 30 minutes - with concurrent EEG monitoring (can induce apnea)
- Alternatively: folinic acid + pyridoxal phosphate for 3 days pending genetic results
- Stop if no improvement; continue if clinical response
For channelopathies (KCNQ2, SCN2A):
- Sodium channel blockers (phenytoin, carbamazepine) are particularly effective
Antimicrobials
-
Start empiric parenteral antibiotics (ampicillin + aminoglycoside/cefotaxime) if infection suspected
-
Add IV acyclovir if HSV encephalitis is possible (maternal herpes history, skin/mucosal lesions, CSF RBCs, no other clear cause)
-
Rosen's Emergency Medicine, p. 1268-1270
-
Tintinalli's Emergency Medicine, p. 2687
-
Bradley and Daroff's Neurology in Clinical Practice, p. 2856
Recent Evidence: Phenobarbital vs. Levetiracetam
Two 2025 meta-analyses address the growing debate over first-line therapy:
- A systematic review and meta-analysis (PMID 37938514) compared levetiracetam vs. phenobarbital for neonatal seizures.
- A second meta-analysis (PMID 40975024) evaluated efficacy and safety of levetiracetam vs. phenobarbital.
Both reflect the active clinical debate driven by phenobarbital's neurotoxicity concerns. Current practice at many centers increasingly uses levetiracetam as an alternative or alongside phenobarbital, though phenobarbital remains the most widely used first-line agent.
Prognosis
-
Neonatal seizures within 24-48h of a difficult birth (usually HIE): severe cerebral damage; many infants succumb; ~50% of survivors are severely disabled
-
Seizures with onset days-weeks after birth (metabolic, hereditary): more often treatable if identified early; better prognosis with specific therapies (pyridoxine, biotin)
-
Benign familial neonatal epilepsy: good prognosis, seizures remit by first year of life
-
"Fifth-day fits": good prognosis, normal development, rarely recur
-
Ohtahara / early myoclonic encephalopathy: poor; often evolves to West or Lennox-Gastaut syndromes
-
Early myoclonic jerks with burst-suppression EEG pattern = particularly ominous
-
Seizures associated with HIE → independently associated with later neurodevelopmental impairment
-
Adams and Victor's Principles of Neurology, p. 352
-
Bradley and Daroff's Neurology in Clinical Practice, p. 2855
Key Summary Points
- Neonatal seizures are almost always acute symptomatic; HIE is the most common cause in term neonates
- Seizures are often subtle (lip-smacking, bicycling, eye deviation) - full tonic-clonic is uncommon
- EEG is mandatory - clinical detection is unreliable in both directions
- The GABA/NKCC1-KCC2 developmental imbalance explains why phenobarbital may be less effective
- Workup must include glucose, electrolytes (Ca, Mg), LP with HSV PCR, and neuroimaging
- Treat immediately: correct metabolic causes, start phenobarbital (first-line), add acyclovir if HSV is possible
- Consider pyridoxine empirically in seizures of unknown etiology
- All neonates with seizures require hospital admission and neurological evaluation
This is a shared conversation. Sign in to Orris to start your own chat.