Epilepsy drugs in easy all information
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive data from the textbooks. Let me compile a thorough, easy-to-read guide.
💊 Epilepsy Drugs — Complete Easy Guide
Source: Adams and Victor's Principles of Neurology, 12th Ed. | Katzung's Basic & Clinical Pharmacology, 16th Ed. | Goodman & Gilman's
🧠 Why Are These Drugs Needed?
Epilepsy is caused by abnormal, excessive electrical firing of brain neurons. Antiepileptic drugs (AEDs) work by:
- Reducing neuronal excitation — blocking sodium or calcium channels
- Enhancing inhibition — boosting GABA (the brain's "brake" chemical)
- Blocking glutamate — reducing the brain's main "accelerator"
📋 Quick Classification
| Group | How They Work | Examples |
|---|---|---|
| Na⁺ Channel Blockers | Stop rapid firing of neurons | Phenytoin, Carbamazepine, Lamotrigine, Lacosamide, Oxcarbazepine |
| GABA Enhancers | Boost brain inhibition | Valproate, Phenobarbital, Benzodiazepines, Vigabatrin, Gabapentin |
| Ca²⁺ Channel Blockers | Block T-type calcium channels | Ethosuximide, Valproate, Zonisamide |
| SV2A Modulators | Modulate synaptic vesicle protein | Levetiracetam, Brivaracetam |
| Glutamate Blockers | Block AMPA receptors | Perampanel, Topiramate |
| Multi-mechanism | Several combined actions | Valproate, Topiramate |
💉 Individual Drug Profiles
1. 🔶 Valproic Acid (Valproate)
- Mechanism: Multiple — GABA potentiation + sodium channel block + T-type Ca²⁺ block + NMDA inhibition
- Used for: ALL seizure types — focal, generalized, absence, myoclonic
- Side effects: Weight gain, hair loss, tremor, liver toxicity (especially in children <2 years), pancreatitis
- ⚠️ Pregnancy: Highly teratogenic — avoid in women of childbearing age (neural tube defects, cognitive impairment in offspring). Virtually absent in breast milk (safe for breastfeeding)
- Special: Drug of choice for juvenile myoclonic epilepsy
2. 🔷 Phenytoin (Dilantin)
- Mechanism: Sodium channel blocker — stabilizes inactive state of Na⁺ channels
- Used for: Focal and generalized tonic-clonic seizures, status epilepticus (IV form)
- Side effects: Gum overgrowth (gingival hyperplasia), hirsutism, facial coarsening, cerebellar atrophy with long-term use, rash
- ⚠️ Tricky pharmacokinetics: Zero-order (non-linear) — small dose changes cause big blood level changes → narrow therapeutic window
- Drug interactions: Hepatic enzyme INDUCER — reduces levels of many other drugs
- HLA warning: HLA-B*1502 (Asian ancestry) → risk of Stevens-Johnson syndrome
3. 🔷 Carbamazepine (Tegretol)
- Mechanism: Sodium channel blocker
- Used for: Focal seizures, generalized tonic-clonic; also trigeminal neuralgia and bipolar disorder
- Side effects: Diplopia, dizziness, ataxia, hyponatremia (SIADH), rash, blood dyscrasias
- ⚠️ Cross-reactivity: High cross-reactivity with phenytoin and phenobarbital for skin reactions
- Enzyme inducer: Speeds up metabolism of many drugs (including its own!)
- In breast milk: 40% of maternal serum level — considered relatively safe
4. 🔷 Oxcarbazepine / Eslicarbazepine
- Mechanism: Sodium channel blocker (similar to carbamazepine)
- Used for: Focal seizures
- Advantage over carbamazepine: Less drug interactions, better tolerated
- Side effects: Hyponatremia (more than carbamazepine), dizziness, rash
5. 🟢 Lamotrigine (Lamictal)
- Mechanism: Sodium channel blocker
- Used for: Focal and generalized seizures, absence seizures
- Side effects: Serious rash — Stevens-Johnson syndrome (especially if titrated too fast)
- Rule: Start LOW, go SLOW with dose titration
- Pregnancy: Relatively preferred over valproate for women of childbearing age
- Enzyme inducer — interactions with other AEDs
6. 🟢 Levetiracetam (Keppra)
- Mechanism: SV2A protein modulation (synaptic vesicle release)
- Used for: Focal and generalized seizures — very broad spectrum
- Advantages: Minimal drug interactions, renal excretion (no liver concerns), no enzyme induction
- Side effects: Mood disturbance, irritability, psychosis (most important limitation)
- Pregnancy: Switch from valproate to levetiracetam is often recommended for women with juvenile myoclonic epilepsy planning pregnancy
7. 🟢 Brivaracetam (Briviact)
- Mechanism: SV2A modulation (like levetiracetam but higher affinity)
- Used for: Focal and generalized seizures
- Advantage: Less psychiatric side effects than levetiracetam
8. 🟡 Phenobarbital
- Mechanism: GABA-A receptor potentiation (increases Cl⁻ channel opening duration)
- Used for: Focal and generalized seizures, neonatal seizures
- Side effects: Sedation, cognitive impairment, dependence
- ⚠️ Breast milk: High concentration → sedates newborns (risky for breastfeeding)
- Enzyme inducer: Major interactions
9. 🟡 Topiramate (Topamax)
- Mechanism: Multiple — GABA potentiation + AMPA/kainate glutamate block + Na⁺ channel block + Ca²⁺ block
- Used for: Focal and generalized seizures; also migraine prevention, obesity
- Side effects: Cognitive impairment ("Dopamax"), word-finding difficulty, kidney stones (nephrolithiasis), weight loss, metabolic acidosis
- Also used in: Status epilepticus (refractory)
10. 🟡 Ethosuximide (Zarontin)
- Mechanism: T-type calcium channel blocker
- Used for: Absence seizures (petit mal) ONLY
- Side effects: GI upset, hiccups, insomnia
- Important: Does NOT work for tonic-clonic or focal seizures — very narrow indication
11. 🟡 Gabapentin / Pregabalin
- Mechanism: Binds α2δ subunit of voltage-gated Ca²⁺ channels → reduces Ca²⁺ influx
- Gabapentin used for: Adjunctive focal seizures, neuropathic pain, postherpetic neuralgia
- Pregabalin used for: Adjunctive focal seizures, neuropathic pain, fibromyalgia, anxiety
- Side effects (both): Sedation, dizziness, peripheral edema, weight gain (pregabalin > gabapentin)
- Advantage: No hepatic metabolism, no drug interactions
12. 🔴 Benzodiazepines (Diazepam, Lorazepam, Clonazepam, Midazolam)
- Mechanism: GABA-A receptor potentiation (increase frequency of Cl⁻ channel opening)
- Primary use: EMERGENCY treatment — status epilepticus (lorazepam/diazepam IV is first-line)
- Clonazepam: Long-term adjunctive use for myoclonic seizures
- Side effects: Sedation, respiratory depression, tolerance, dependence
- ⚠️ Breast milk: High levels — sedation risk for newborns
13. 🔵 Lacosamide (Vimpat)
- Mechanism: Slow inactivation of Na⁺ channels (unique mechanism — different from other Na blockers)
- Used for: Focal and generalized seizures
- Side effects: Dizziness, diplopia, PR interval prolongation (cardiac monitoring if pre-existing conduction issues)
14. 🔵 Zonisamide (Zonegran)
- Mechanism: Na⁺ channel block + T-type Ca²⁺ block (similar profile to topiramate)
- Used for: Focal and generalized seizures
- Side effects: Kidney stones, cognitive impairment, weight loss (similar to topiramate)
- Also: Sulfonamide derivative — contraindicated if sulfa allergy
15. 🔵 Vigabatrin (Sabril)
- Mechanism: Irreversible GABA transaminase inhibitor → increases GABA levels
- Used for: Infantile spasms (West syndrome — first-line), refractory focal seizures
- ⚠️ Major side effect: Permanent visual field defects (retinal toxicity) — requires regular ophthalmology monitoring
16. 🔵 Perampanel (Fycompa)
- Mechanism: AMPA glutamate receptor antagonist (unique class)
- Used for: Focal and generalized seizures (adjunctive)
- Side effects: Dizziness, aggression/hostility, psychiatric symptoms
⚡ Status Epilepticus Treatment (Emergency)
| Step | Drug | Route |
|---|---|---|
| 1st line | Lorazepam or Diazepam | IV |
| 2nd line | Phenytoin / Fosphenytoin or Valproate | IV |
| 3rd line (refractory) | Phenobarbital, Propofol, Midazolam, Ketamine | IV infusion |
🤰 Epilepsy Drugs in Pregnancy
| Drug | Safety | Notes |
|---|---|---|
| Valproate | ❌ Most dangerous | Neural tube defects, cognitive harm to fetus |
| Phenytoin | ⚠️ Avoid if possible | Fetal hydantoin syndrome |
| Carbamazepine | ⚠️ Caution | Spina bifida risk |
| Lamotrigine | ✅ Preferred | Monitor levels (clearance increases) |
| Levetiracetam | ✅ Preferred | Good safety profile |
| Phenobarbital | ⚠️ Caution | Neonatal withdrawal risk |
🧬 Key Skin Reaction Warning
The aromatic drugs — phenytoin, carbamazepine, phenobarbital, lamotrigine — carry risk of:
- Maculopapular rash (common, usually resolves on stopping)
- Stevens-Johnson syndrome / Toxic Epidermal Necrolysis (life-threatening)
- High cross-reactivity between this group — if one causes rash, avoid all aromatics
Genetic test: HLA-B*1502 (Asian ancestry) → screen before starting carbamazepine/phenytoin
🔑 Memory Tricks
| Drug | Easy Memory |
|---|---|
| Ethosuximide | E= Elite drug for absence only |
| Vigabatrin | Vision loss (Visual field defect) |
| Levetiracetam | Loses temper (mood/behavior side effects) |
| Topiramate | Thinks slowly (Topiramate = cognitive impairment) |
| Phenytoin | Pharmacokinetics are tricky (non-linear/zero-order) |
| Valproate | Very broad but Very teratogenic |
📊 Summary at a Glance
| Drug | Type | Best For | Key Side Effect |
|---|---|---|---|
| Valproate | Multi-mechanism | All seizure types | Teratogenic, weight gain |
| Phenytoin | Na blocker | Focal, GTC, status | Non-linear kinetics, gum hyperplasia |
| Carbamazepine | Na blocker | Focal, GTC | Hyponatremia, rash |
| Lamotrigine | Na blocker | Focal, generalized | SJS risk if titrated fast |
| Levetiracetam | SV2A | Focal, generalized | Irritability, psychosis |
| Ethosuximide | Ca blocker | Absence ONLY | GI upset |
| Phenobarbital | GABA | Focal, generalized | Sedation, dependence |
| Topiramate | Multi | Focal, generalized | Cognitive impairment, kidney stones |
| Gabapentin | Ca blocker | Focal (adjunct), pain | Sedation, edema |
| Vigabatrin | GABA | Infantile spasms | Retinal toxicity |
| Benzodiazepines | GABA | Status epilepticus | Tolerance, sedation |
| Lacosamide | Na (slow) | Focal, generalized | PR prolongation |
| Perampanel | AMPA blocker | Focal (adjunct) | Aggression |
— Adams and Victor's Principles of Neurology, 12th Edition | Katzung's Basic & Clinical Pharmacology, 16th Edition | Goodman & Gilman's The Pharmacological Basis of Therapeutics
Thiopentone sodium all information
Checking Date & Time
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive information from Miller's Anesthesia and Katzung's Pharmacology. Let me compile the full guide.
💉 Thiopentone Sodium — Complete Guide
Source: Miller's Anesthesia 10th Ed. | Katzung's Basic & Clinical Pharmacology 16th Ed. | Goodman & Gilman's
🧪 Chemical Identity
| Property | Detail |
|---|---|
| Full name | Thiopental sodium (Thiopentone sodium in UK) |
| Drug class | Thiobarbiturate (ultrashort-acting barbiturate) |
| Chemical feature | Sulfur atom at C2 position of barbituric acid ring → makes it highly lipid-soluble with rapid onset |
| pKa | 7.6 — ~50% nonionized at physiologic pH 7.4, enabling rapid CNS penetration |
| pH of solution | 10–11 (highly alkaline — important for drug interactions) |
| Historical note | Introduced into clinical practice in 1934, marking the beginning of modern IV anesthesia |
Chemical Structure
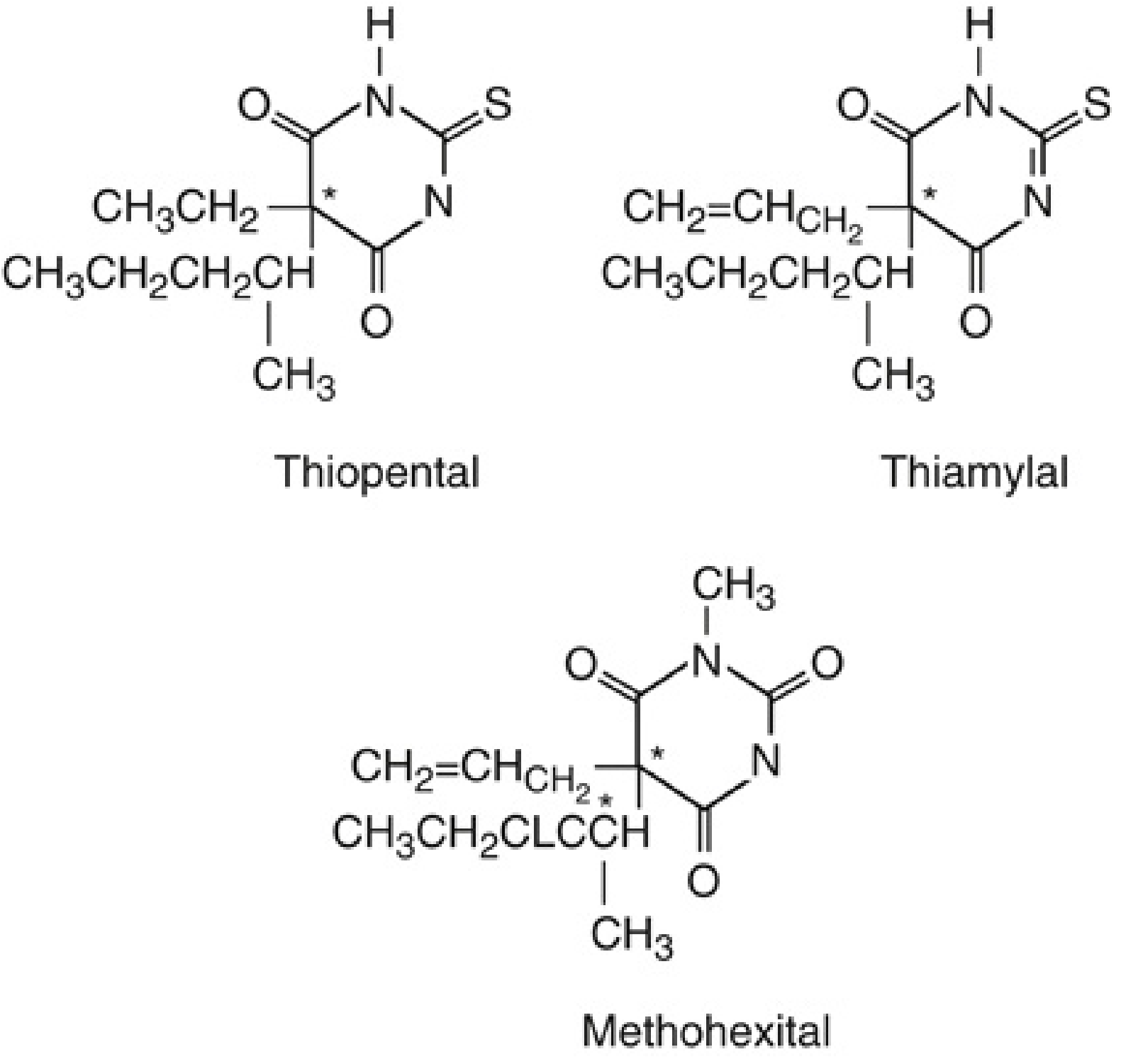
The sulfur at position C2 (vs. oxygen in oxybarbiturates) gives thiopental its rapid onset and high lipid solubility.
⚙️ Mechanism of Action
Thiopentone acts via two main mechanisms:
1. GABA-A Receptor Potentiation (Primary)
- Binds to GABA-A receptor (a Cl⁻ ion channel)
- At low concentrations: Enhances GABA's effect → increases duration of Cl⁻ channel opening → hyperpolarization → sedation/hypnosis
- At higher concentrations: Acts as GABA mimetic itself — opens Cl⁻ channels even without GABA → produces full anesthesia
- Net result: Increased Cl⁻ conductance → hyperpolarized neuron → raised threshold for firing
2. Inhibition of Excitatory Transmission (Secondary)
- Blocks glutamate (NMDA-gated currents) in a concentration-dependent manner
- Decreases extracellular glutamate levels in the CNS
- Also reduces acetylcholine synaptic transmission
Key point: Unlike benzodiazepines (which only increase frequency of Cl⁻ channel opening), barbiturates also increase the duration of opening AND can directly activate channels at high doses.
💊 Pharmacokinetics
Distribution & Redistribution
| Phase | What Happens |
|---|---|
| Onset | Drug enters highly perfused brain within 30 seconds of IV injection |
| Termination of single dose | Due to redistribution — drug moves from brain → lean muscle tissue (NOT due to metabolism) |
| Recovery after single dose | Comparable to propofol — rapid awakening |
| Repeated doses / infusion | Drug saturates peripheral compartments → recovery markedly prolonged (depends on slow hepatic metabolism) |
Key Pharmacokinetic Values
| Parameter | Value |
|---|---|
| Onset | < 30 seconds IV |
| Duration (single dose) | 5–10 minutes |
| Elimination half-life | Long (hours) — due to redistribution |
| Protein binding | High (~85%) |
| Volume of distribution | Large — slightly bigger in women and in pregnancy |
Metabolism
- Hepatic — by 4 processes:
- Oxidation at C5 (most important) → polar metabolites excreted in urine
- N-dealkylation
- Desulfuration at C2 (removes the sulfur)
- Destruction of barbituric acid ring (minor)
- Metabolites are inactive, water-soluble → excreted in urine/bile
- NOT significantly altered by liver cirrhosis (unusually — liver clearance preserved)
- In large doses (300–600 mg/kg): switches from first-order → zero-order kinetics (Michaelis-Menten saturation)
🏥 Clinical Uses & Dosage
| Indication | Dose | Route |
|---|---|---|
| Induction of general anesthesia | 3–5 mg/kg IV | IV bolus |
| Refractory status epilepticus | Higher doses (titrated to isoelectric EEG) | IV infusion |
| Raised ICP / neuroprotection | Titrated to burst suppression on EEG | IV infusion |
| Rectal induction (children) | 20–30 mg/kg | Per rectum |
- Unconsciousness occurs in < 30 seconds
- Patients may notice a garlic or onion taste after injection
- ⚠️ DO NOT mix with depolarizing or non-depolarizing muscle relaxants in the same syringe — precipitation of insoluble thiopentone acid occurs (very different pH)
🫀 Organ System Effects
CNS Effects
| Effect | Detail |
|---|---|
| Dose-dependent CNS depression | Sedation → hypnosis → anesthesia → coma |
| No analgesia | May actually reduce pain threshold (hyperalgesia at subhypnotic doses) |
| Cerebral vasoconstriction | ↓ Cerebral blood flow (CBF) ↓ Cerebral blood volume ↓ ICP |
| ↓ CMRO2 | Reduces cerebral metabolic oxygen consumption (dose-dependent, up to isoelectric EEG) |
| Neuroprotection | From focal ischemia (stroke, surgical retraction, aneurysm surgery) — not for global ischemia (e.g., cardiac arrest) |
| Anticonvulsant | Yes — suppresses EEG activity; used in refractory status epilepticus |
| Amnesia | Less pronounced than benzodiazepines |
| EEG | Progressively slows → burst suppression → isoelectric EEG at maximum dose |
Note: ICP decreases more than MAP after thiopental, preserving cerebral perfusion pressure (CPP = MAP − ICP). This is why it is useful in neurosurgery.
Cardiovascular Effects
- ↓ Blood pressure — primarily from peripheral vasodilation
- Negative inotrope — direct depression of cardiac contractility
- Baroreceptor reflex less inhibited than with propofol → compensatory ↑ heart rate limits hypotension
- ⚠️ More dangerous in: hypovolemia, cardiac tamponade, cardiomyopathy, coronary artery disease — these patients cannot compensate for vasodilation
- Hypotension worsened by: large doses, rapid injection rate
Respiratory Effects
- Respiratory depressant — typical induction dose causes transient apnea
- ↓ Tidal volume + ↓ respiratory rate → ↓ minute ventilation
- ↓ Ventilatory response to hypercapnia and hypoxia
- Laryngeal and cough reflexes less suppressed than propofol → inferior choice for airway instrumentation without muscle relaxants
- Risk of laryngospasm or bronchospasm if airway stimulated during light anesthesia
⚠️ Adverse Effects & Complications
| Complication | Details |
|---|---|
| Transient apnea | After induction dose — have airway equipment ready |
| Hypotension | More severe in hypovolemic/cardiac patients |
| Laryngospasm / bronchospasm | If airway manipulated under light anesthesia |
| Intra-arterial injection | Causes excruciating pain + intense vasoconstriction → gangrene. Treat with stellate ganglion block + local lidocaine 0.5% (5–10 mL) to dilute drug |
| Extravasation | Tissue necrosis (highly alkaline solution) — inject local lidocaine |
| Histamine release | Occasional — bronchospasm, urticaria |
| Allergic reactions | Rare — 1 in 30,000 patients; life-threatening anaphylaxis possible |
| Hyperalgesia | At sub-hypnotic blood levels — lowers pain threshold |
| Hangover / prolonged sedation | After repeated doses or infusion due to accumulation |
🚫 Contraindications
| Contraindication | Reason |
|---|---|
| Acute intermittent porphyria | Barbiturates stimulate γ-aminolevulinic acid synthetase → ↑ porphyrin production → precipitates acute porphyric crisis |
| Severe hypovolemia / shock | Profound hypotension risk |
| Airway obstruction / difficult airway | Respiratory depression + ↓ airway reflexes |
| Known hypersensitivity to barbiturates | Anaphylaxis risk |
| No IV access | Cannot use without reliable IV line |
🔬 Structure–Activity Relationship
| Position | Substitution | Effect |
|---|---|---|
| C2 — Sulfur (instead of oxygen) | Thiobarbiturate | ↑ Lipid solubility → faster onset |
| C5 — Alkyl/aryl groups | Hypnotic & sedative effect | Longer side chains = more potent |
| C5 — Phenyl group | Anticonvulsant activity | e.g., phenobarbital |
| N1 — Methyl group | Even faster onset | e.g., methohexital (but causes excitatory side effects) |
🔄 Thiopentone vs. Propofol (Key Comparison)
| Feature | Thiopentone | Propofol |
|---|---|---|
| Onset | < 30 sec | < 30 sec |
| Recovery (single dose) | Similar | Similar |
| Recovery (infusion) | Prolonged (accumulates) | Short (context-sensitive) |
| Blood pressure ↓ | Moderate | More pronounced |
| Antiemetic | No | Yes |
| Neuroprotection | Yes | Minimal |
| Anticonvulsant | Yes | Limited |
| Pain on injection | No (IV) | Common |
| Porphyria | Contraindicated | Safe |
| Current role | Largely replaced by propofol | First-line IV induction |
🧠 Memory Summary
THIOPENTONE = "The GABA GAP Closer"
G — GABA potentiation (prolongs Cl⁻ channel opening)
A — Anesthesia induction (3–5 mg/kg IV)
B — Brain protective (↓ ICP, ↓ CMRO2)
A — Apnea + Apnoea risk
G — Garlic/onion taste on injection
A — Avoid in Porphyria (ABSOLUTE contraindication)
P — Precipitation with muscle relaxants (pH mismatch)
📊 Quick Reference Card
| Property | Value |
|---|---|
| Class | Thiobarbiturate |
| Mechanism | GABA-A potentiation + glutamate block |
| Dose (induction) | 3–5 mg/kg IV |
| Onset | < 30 seconds |
| Duration (single dose) | 5–10 minutes |
| Termination mechanism | Redistribution |
| Metabolism | Hepatic (oxidation) |
| Key CNS effect | ↓ ICP, ↓ CMRO2, anticonvulsant |
| Key CVS effect | ↓ BP (vasodilation + neg. inotropy) |
| Key respiratory effect | Transient apnea |
| Absolute contraindication | Acute intermittent porphyria |
| Dangerous complication | Intra-arterial injection → gangrene |
| Key drug interaction | Precipitates with suxamethonium/muscle relaxants |
— Miller's Anesthesia, 10th Edition | Katzung's Basic & Clinical Pharmacology, 16th Edition | Goodman & Gilman's The Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.