Macrolids
Reading File
Finding Sources
Searching PubMed
macrolide antibiotics mechanisms clinical use
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a thorough overview of macrolide antibiotics, drawn from multiple authoritative pharmacology and microbiology textbooks.
Macrolide Antibiotics
1. Structure & Classification
Macrolides are characterized by a large macrocyclic lactone ring (14 atoms in erythromycin and clarithromycin; 15 atoms in azithromycin) to which one or more deoxy sugars are attached. Erythromycin, the prototype, was isolated in 1952 from Streptomyces erythraea. The semisynthetic derivatives were designed to improve upon its weaknesses:
- Clarithromycin: methylation of the 6-OH group - improves acid stability and tissue penetration
- Azithromycin: addition of a methyl-substituted nitrogen into the lactone ring - creates a 15-membered "azalide" ring, broadening spectrum and massively extending half-life
Ketolides (e.g., telithromycin) are related derivatives with a 3-keto group replacing the cladinose sugar; they retain activity against some macrolide-resistant strains, but hepatotoxicity concerns limited their use.
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
2. Mechanism of Action
Macrolides inhibit bacterial protein synthesis by binding to the 50S ribosomal subunit (specifically the 23S rRNA). The key effects are:
- Blocking the polypeptide exit tunnel - prevents peptide chain elongation (transpeptidation)
- Inhibiting translocation - the newly synthesized peptidyl-tRNA cannot move from the acceptor (A) site to the donor (P) site
- Causes dissociation of peptidyl-tRNA from the ribosome
- Erythromycin also inhibits assembly of the 50S subunit
They are generally bacteriostatic, but may be bactericidal at high concentrations or against highly susceptible organisms. Activity is enhanced at alkaline pH.
Their binding site overlaps with that of clindamycin and chloramphenicol, which is clinically relevant for cross-resistance.
- Lippincott Illustrated Reviews: Pharmacology
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
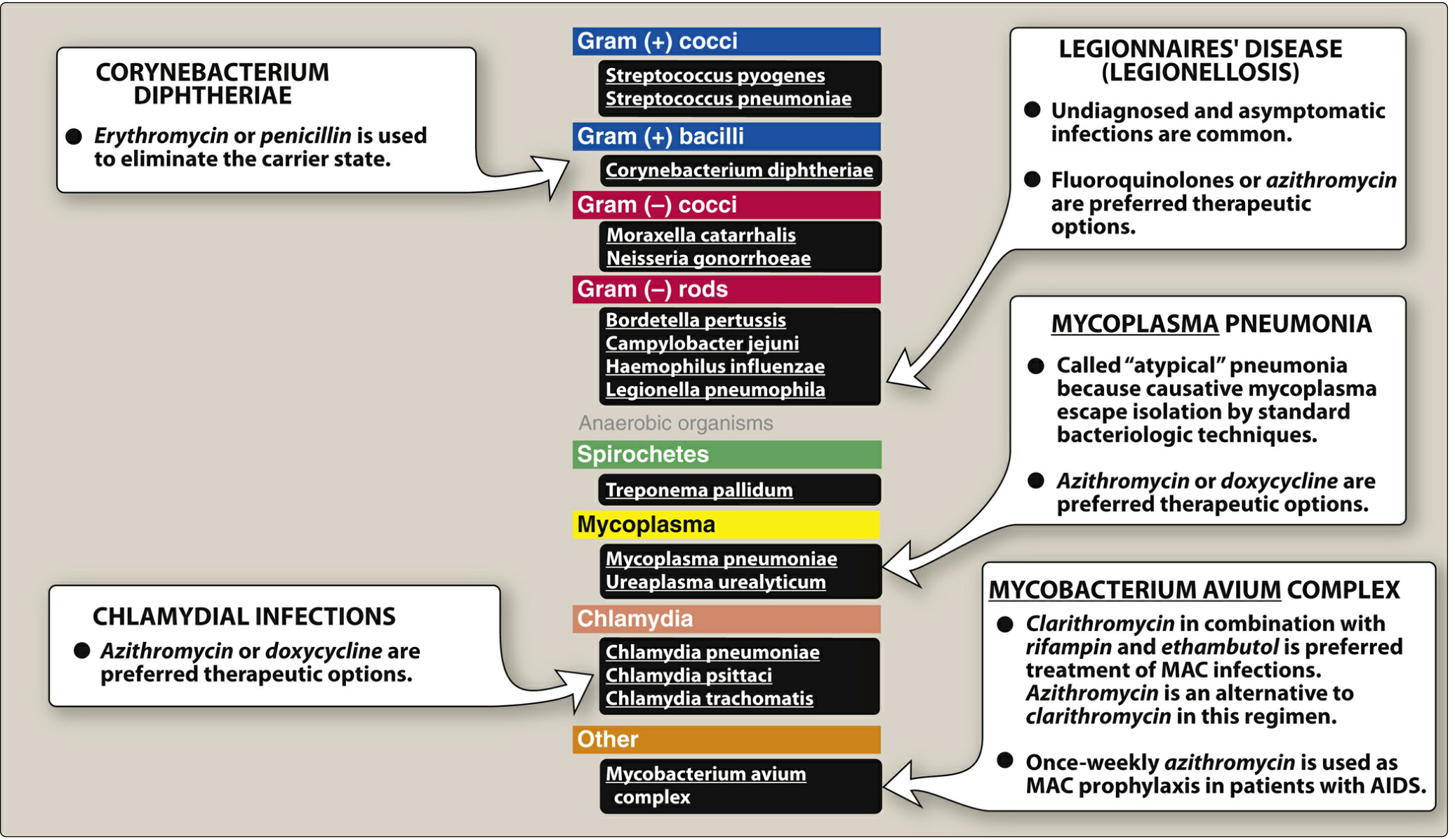
3. Antibacterial Spectrum
| Drug | Key Coverage |
|---|---|
| Erythromycin | Streptococci, pneumococci, Corynebacterium, Treponema pallidum, Bordetella pertussis, Campylobacter, Legionella, Mycoplasma, Chlamydia, Listeria, H. pylori, some Rickettsia |
| Clarithromycin | All of the above + H. influenzae (better), Moraxella catarrhalis, Borrelia burgdorferi, M. avium complex (MAC), Ureaplasma |
| Azithromycin | Less active vs. streptococci/staphylococci, but stronger vs. H. influenzae, M. catarrhalis, N. gonorrhoeae, Campylobacter jejuni, MAC (prophylaxis in AIDS) |
Gram-negative enteric bacilli are largely resistant (due to poor outer membrane permeability). Macrolides do NOT cover aerobic gram-negative rods (Enterobacteriaceae).
- Lippincott Illustrated Reviews: Pharmacology
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.
4. Resistance Mechanisms
Four main mechanisms:
- Reduced uptake / active efflux - efflux pumps encoded by mef and msr genes (most common in gram-positive organisms like pneumococci)
- Ribosomal methylation - a methylase (encoded by erm genes) methylates an adenine in 23S rRNA, reducing binding affinity (inducible or constitutive; plasmid-transmitted)
- Enzymatic inactivation - macrolide esterases produced by Enterobacteriaceae that hydrolyze the lactone ring
- Ribosomal target mutation - chromosomal mutation altering the 50S binding site
Cross-resistance occurs among all macrolides. Resistance to erythromycin = resistance to clarithromycin and azithromycin. Macrolide resistance can also confer cross-resistance to clindamycin (MLSb phenotype).
5. Pharmacokinetics
| Property | Erythromycin | Clarithromycin | Azithromycin |
|---|---|---|---|
| Oral absorption | Yes (acid-labile base; use enteric-coated or ester forms) | Yes (acid-stable) | Yes (acid-stable) |
| Half-life (hours) | ~2 | ~3.5 | ~68 |
| Active metabolite | No | Yes (14-OH-clarithromycin) | No |
| Urinary excretion | <15% | 30-50% | <10% |
| Primary elimination | Hepatic/bile | Hepatic + renal | Bile (as active drug) |
Key points:
-
Azithromycin has the longest half-life of all macrolides and the largest volume of distribution - concentrates in neutrophils, macrophages, and fibroblasts (tissue concentrations far exceed serum levels). This allows short 3-5 day courses.
-
Erythromycin base is destroyed by gastric acid; must be given as enteric-coated tablets or ester formulations (stearate, estolate, ethylsuccinate). Food impairs absorption of erythromycin and azithromycin but increases clarithromycin absorption.
-
All macrolides concentrate in the liver. None penetrate the CSF well.
-
Erythromycin is one of the few antibiotics to penetrate prostatic fluid.
-
Lippincott Illustrated Reviews: Pharmacology
6. Clinical Uses
| Indication | Preferred Agent |
|---|---|
| Community-acquired pneumonia (atypical) | Azithromycin or clarithromycin |
| Legionnaires' disease | Azithromycin (or fluoroquinolone) |
| Chlamydial infections (urogenital) | Azithromycin (single dose 1 g) or doxycycline |
| Mycoplasma pneumoniae | Azithromycin or doxycycline |
| H. pylori eradication | Clarithromycin + amoxicillin + PPI (triple therapy) |
| MAC infection (HIV/AIDS) | Clarithromycin + rifabutin + ethambutol |
| MAC prophylaxis (AIDS, CD4 <50) | Weekly azithromycin |
| Pertussis (whooping cough) | Azithromycin or erythromycin |
| Diphtheria carrier state | Erythromycin or penicillin |
| Penicillin-allergic patients | Erythromycin as alternative for strep/pneumococcal infections |
| Gastroparesis | Erythromycin (prokinetic effect via motilin receptor agonism) |
7. Adverse Effects
- GI distress - most common adverse effect, especially with erythromycin (nausea, vomiting, abdominal cramping). Erythromycin acts as a motilin receptor agonist, stimulating GI motility - exploited therapeutically for gastroparesis/ileus.
- Cholestatic jaundice - mainly with erythromycin estolate (hypersensitivity reaction); also reported with other formulations.
- Ototoxicity - transient hearing loss with erythromycin at high doses; irreversible sensorineural hearing loss reported with azithromycin.
- QT prolongation / cardiac arrhythmias - ventricular tachycardia (torsades de pointes) risk with all macrolides, especially IV erythromycin. Risk is increased by co-administration of CYP3A4 inhibitors. Use with caution in patients with pre-existing QT prolongation.
- Hepatotoxicity - erythromycin hepatotoxicity may be increased during pregnancy.
- Drug interactions - Erythromycin and clarithromycin are potent CYP3A4 inhibitors and also inhibit P-glycoprotein. This raises plasma levels of co-administered drugs like statins, cyclosporine, tacrolimus, warfarin, digoxin, alprazolam, and others. Azithromycin minimally inhibits CYP3A4.
8. Summary Comparison
| Feature | Erythromycin | Clarithromycin | Azithromycin |
|---|---|---|---|
| Acid stability | Poor | Good | Good |
| GI side effects | High | Moderate | Low |
| Half-life | Short (2h) | Moderate (3.5h) | Very long (68h) |
| CYP3A4 inhibition | Strong | Strong | Minimal |
| H. pylori coverage | Yes | Yes (preferred) | Less preferred |
| MAC coverage | Weak | Yes | Yes |
| H. influenzae | Weak | Moderate | Best |
| Dosing | 4x/day | 2x/day | 1x/day (or 3-5 day course) |
Sources: Katzung's Basic and Clinical Pharmacology 16th Ed., Goodman & Gilman's 14th Ed., Jawetz Melnick & Adelberg's Medical Microbiology 28th Ed., Lippincott Illustrated Reviews: Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.