Recurrent herpes simplex virus with clinical feature, histopathology, laboratory finding and treatment
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material to write a detailed, well-structured answer. Let me compile everything.
Recurrent Herpes Simplex Virus (HSV) Infection
Overview and Pathogenesis
Recurrent HSV infection (secondary HSV) represents a recrudescent viral infection in a person previously infected with HSV-1 or HSV-2. It is not a new infection but the re-emergence of latent virus. After primary infection, HSV establishes latency within dermatome-associated ganglionic neurons (trigeminal ganglion for HSV-1 orolabial, sacral ganglia for HSV-2 genital). Latency-infected neuronal cells range from 4% to 35% within the affected ganglion. The virus is maintained in a dormant state through host immune suppression of alpha-gene expression. When immunological homeostasis is disturbed, the virus reactivates, travels anterograde down the nerve, and causes recurrent disease. - Cummings Otolaryngology, p. 1592
Triggers for reactivation include:
- UV light / sunlight exposure
- Physical or emotional stress
- Fever / systemic illness
- Menstruation or hormonal changes
- Immunosuppression (HIV, chemotherapy, transplant)
- Trauma (dental procedures, laser resurfacing)
- Epidural morphine administration (3.5-30% incidence of HSV labialis reactivation reported) - Morgan & Mikhail's Clinical Anesthesiology
Clinical Features
1. Herpes Labialis (Cold Sore / Fever Blister)
The most common form of recurrent HSV-1 disease. Prevalence of primary HSV-1 immunity in the US ranges from 40-60%; of those, 5-23% suffer recurrences, while 58-61% have recurrences every 1-4 months.
Clinical course:
| Stage | Features |
|---|---|
| Prodrome | Focal tingling, burning, or altered sensation (hours before vesicles) |
| Vesicular stage | Pinhead-sized, clustered vesicles on erythematous/edematous base over the vermilion border |
| Ulcerative stage | Vesicles coalesce then rupture, forming tender erosions |
| Crusting stage | Lesions crust over and heal, typically within 7-10 days |
| Healing | Heals without scarring in immunocompetent patients |
The site of involvement is consistent and repetitive from episode to episode (unlike fixed drug eruption, where the site is exactly the same). The lesion typically occurs at the vermilion border of the lip, extending to adjacent skin. - Cummings Otolaryngology, p. 1592-1593

Recurrent herpes simplex infection (tongue) - Andrews' Diseases of the Skin
2. Recurrent Intraoral HSV
Affects keratinized/attached mucosa only - the hard palate, attached gingiva, and dorsal tongue. This is a key distinguishing feature from recurrent aphthous stomatitis (which involves non-attached, non-keratinized mucosa). Lesions occur as numerous small, discrete vesicles in clusters, which rupture rapidly to form punctate erosions with a red base. Distribution is typically unilateral, following the greater palatine nerve in the first molar and premolar region, and does not cross the midline. - Andrews' Diseases of the Skin, p. 931
3. Recurrent Genital Herpes (HSV-1 or HSV-2)
- Males: lesions on the glans, shaft of penis, or urethra (presents as dysuria and clear penile discharge - often misdiagnosed as NGU)
- Females: vulva, vagina, cervix, perianal area, inner thigh; accompanied by itching and mucoid vaginal discharge
- Both sexes: upper buttock is a common site
- Recurrent disease is shorter in duration and less severe than the primary episode
- ~50% of patients have prodromal burning/tingling before lesion eruption
- Heals without scarring
- Episodes may occur every 2-3 weeks or may be infrequent
- Inguinal adenopathy may be present
- Natural history: frequency of outbreaks decreases after 3-5 years in at least two-thirds of patients - Andrews' Diseases of the Skin, p. 819-822
4. Special Patterns
- Eczema herpeticum (Kaposi varicelliform eruption): HSV dissemination into eczematous skin of atopic patients
- Herpetic whitlow: digital HSV, recurrent in healthcare workers
- Herpes gladiatorum: wrestlers; HSV spread through skin abrasions
- Chronic progressive ulcerative herpes: seen in HIV-infected and immunocompromised patients (leukemia, neutropenia) - may mimic mucosal toxicity to chemotherapy
- Herpetic geometric glossitis: linear longitudinal, cross-hatched, or branching fissures of the dorsal tongue, mainly in immunocompromised patients
Histopathology
The histopathological hallmarks of HSV infection are:
- Intraepithelial/intraepidermal vesicle - the earliest lesion; virus replicates within the squamous epithelium causing ballooning degeneration of cells and intraepidermal vesicle formation
- Ballooning degeneration - intracellular edema in keratinocytes in response to cytopathic viral effects
- Acantholysis - loss of intercellular connections leads to intraepithelial vesiculation
- Multinucleated giant cells (polykaryocytes) - keratinocytes fuse due to viral glycoproteins; nuclei show:
- Ground-glass ("steel grey") chromatin - margination of chromatin
- Nuclear molding - nuclei conform to each other's shape
- Cowdry type A intranuclear inclusion bodies - eosinophilic inclusions surrounded by a clear halo that may occupy up to half the nuclear volume; with time they become more basophilic, filling and deforming the nucleus
- Necrotic cellular debris within the vesicle
- As vesicles enlarge and ulcerate, they may coalesce into larger lesions with normal intervening mucosa
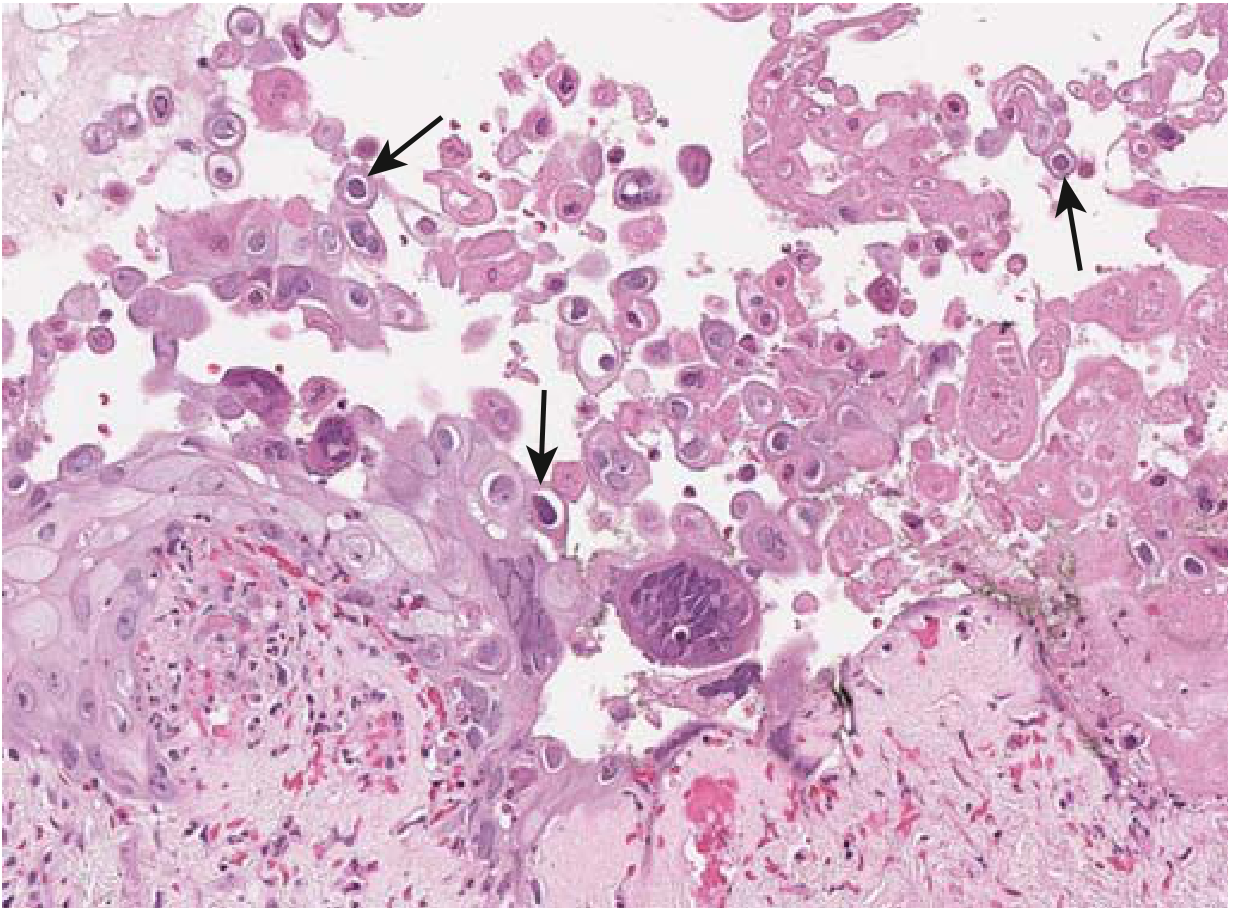
HSV biopsy: intraepithelial vesicle with Cowdry-type A bodies (arrows - purple intranuclear inclusions surrounded by halo) and multinucleate cells with nuclear molding - Robbins & Kumar Basic Pathology
Biopsy tip: Biopsies and cytological brushings should be taken from the edge of an ulcer, not the ulcer base, because the viral cytopathic effect with multinucleated giant cells is best identified at the edge. - Yamada's Textbook of Gastroenterology, p. 927
Laboratory Findings / Diagnosis
| Approach | Test | Comment |
|---|---|---|
| Tzanck smear | Direct microscopic exam of cells scraped from vesicle base; Wright or Giemsa stain | Shows multinucleated giant cells and Cowdry type A inclusion bodies; does NOT distinguish HSV from VZV |
| Viral culture | Inoculation of vesicle fluid or swab into cell cultures | Identifiable cytopathic effect in most cell cultures; gold standard for genital lesions; sensitivity decreases with older lesions |
| PCR (currently favored) | Assay of tissue biopsy, smear, CSF, or vesicular fluid for HSV DNA | Most sensitive and specific; preferred for CSF in encephalitis; can type HSV-1 vs HSV-2 |
| Immunofluorescence (DFA) | Direct fluorescent antibody staining of smear or biopsy | Rapid antigen detection; can distinguish HSV from VZV; allows typing |
| Enzyme immunoassay (EIA) | Antigen detection from vesicle fluid or tissue | Useful for rapid diagnosis |
| Serology | Type-specific antibody (IgG to gC-1/gG-2) | Not useful for diagnosing active recurrent lesions; useful for epidemiology and determining prior infection status; identifies HSV-1 vs HSV-2 |
| Immunohistochemistry | Specific monoclonal antibodies to HSV on biopsy | Helpful when viral cytopathic effect is infrequent |
- Medical Microbiology 9e, Table 43.2; Yamada's Textbook of Gastroenterology
PCR is the currently favored approach for most confirmatory testing. Serology is not useful for diagnosing active recurrent disease.
Clinical diagnosis pitfall: The diagnosis of recurrent genital herpes should not be made on clinical appearance alone because of the significant psychological impact; laboratory confirmation (culture, PCR, or DFA) is recommended. - Andrews' Diseases of the Skin, p. 828
Treatment
Principles
Treatment goals include reducing symptom duration, accelerating healing, reducing viral shedding, and (for genital herpes) reducing transmission risk. HSV cannot be eradicated. All antivirals below work by inhibiting viral DNA polymerase after phosphorylation by viral thymidine kinase.
Episodic (Intermittent) Therapy
To be effective, must be initiated at the earliest prodromal symptom (before vesicle formation). Patient should have medication available in advance. Reduces recurrence duration by approximately 1 day.
Recurrent Genital Herpes - Episodic options:
| Drug | Dose | Duration |
|---|---|---|
| Acyclovir | 200 mg 5× daily OR 800 mg twice daily | 5 days |
| Acyclovir (short course) | 800 mg 3× daily | 2 days |
| Valacyclovir | 500 mg twice daily | 3 days |
| Famciclovir | 125 mg twice daily | 5 days |
| Famciclovir (short course) | 1 g twice daily | 1 day |
Recurrent Herpes Labialis:
- Valacyclovir: single dose at prodrome
- Topical penciclovir (approved): reduces pain and lesions by ~1 day
- Topical acyclovir / docosanol: approved for orolabial use but much less effective than oral drugs
Suppressive (Chronic) Therapy
For patients with frequent recurrences (6-12 per year). Suppresses 85% of recurrences; 20% of patients become recurrence-free.
| Drug | Dose |
|---|---|
| Acyclovir | 400 mg twice daily OR 200 mg 3× daily OR 800 mg once daily |
| Valacyclovir | 500 mg/day (or 1000 mg/day if >10 recurrences/year) |
| Famciclovir | 250 mg twice daily |
Valacyclovir 500 mg/day also reduces transmission of genital HSV to uninfected partners.
Special Populations
- Immunocompromised patients: Higher doses required; more frequent recurrences; may develop acyclovir-resistant strains
- Acyclovir-resistant HSV (due to thymidine kinase mutations): Treat with foscarnet IV; alternatives include cidofovir or topical trifluridine
- Pregnancy: Acyclovir 400 mg 3× daily for initial episodes; chronic suppressive therapy from 36 weeks to delivery recommended to reduce outbreaks and cesarean delivery need - Andrews' Diseases of the Skin
Topical Agents
- Topical penciclovir cream: approved for herpes labialis
- Topical foscarnet, trifluridine, cidofovir: for acyclovir-resistant mucosal disease in immunocompromised hosts
- Intralesional cidofovir: for resistant cases
Differential Diagnosis
| Condition | Distinguishing features |
|---|---|
| Recurrent aphthous stomatitis | Non-attached mucosa (labial, buccal); solitary or few; NOT preceded by vesicles |
| Herpes zoster | Dermatome, does not recur in same distribution; culture/DFA distinguish |
| Herpangina | Non-attached mucosa; posterior oropharynx; coxsackievirus; not on gingiva |
| Fixed drug eruption | Same exact site; no prodrome; related to drug ingestion |
| Chancre (syphilis) | Indurated, painless; single lesion; serologic testing |
| Behcet disease | Oral and genital ulcers + systemic features; no virus isolated |
Key Teaching Points:
- Recurrent HSV is shorter and milder than primary infection in immunocompetent hosts
- Intraoral recurrences always involve keratinized/attached mucosa (hard palate, gingiva)
- Histopathology: intraepithelial vesicle + multinucleated giant cells + Cowdry type A bodies (ground-glass nuclei, nuclear molding)
- Lab diagnosis: Tzanck smear (quick screening), PCR (most sensitive, preferred), culture (gold standard for genital)
- Serology is NOT useful for diagnosing active recurrent lesions
- Treatment: episodic (start at prodrome) or suppressive (for ≥6 recurrences/year)
- Acyclovir-resistant HSV: treat with foscarnet
Sources: Andrews' Diseases of the Skin (9780323547536) | Cummings Otolaryngology (9780323612173) | Robbins & Kumar Basic Pathology (9780323790185) | Medical Microbiology 9e (9780323673228) | Harrison's Principles of Internal Medicine 22E (9781265977061) | Yamada's Textbook of Gastroenterology (9781119600169)
This is a shared conversation. Sign in to Orris to start your own chat.