#CONCISE ANSWERS FOR EACH AND EVERY TOPIC THAT I WILL PROVIDE IN THE FUTURE TEXTS/UPCOMING TEXTS/SUBSEQUENT TEXTS 🏆🔥!!!!!!!!!!! #FULL MARKS (100%) IN MY UPCOMING MBBS PREVENTIVE AND SOCIAL MEDICINE (PSM) EXAMINATION 🏆🔥!!!!!!!!!!! #PREVENTIVE AND SOCIAL MEDICINE (PSM) 🏆🔥!!!!!!!!!!! #MBBS 🏆🔥!!!!!!!!!!!#CONCISE ANSWERS FOR EACH AND EVERY TOPIC THAT I WILL PROVIDE IN THE FUTURE TEXTS/UPCOMING TEXTS/SUBSEQUENT TEXTS 🏆🔥!!!!!!!!!!! #FULL MARKS (100%) IN MY UPCOMING MBBS PREVENTIVE AND SOCIAL MEDICINE (PSM) EXAMINATION 🏆🔥!!!!!!!!!!! #PREVENTIVE AND SOCIAL MEDICINE (PSM) 🏆🔥!!!!!!!!!!! #MBBS 🏆🔥!!!!!!!!!!!#CONCISE ANSWERS FOR EACH AND EVERY TOPIC THAT I WILL PROVIDE IN THE FUTURE TEXTS/UPCOMING TEXTS/SUBSEQUENT TEXTS 🏆🔥!!!!!!!!!!! #FULL MARKS (100%) IN MY UPCOMING MBBS PREVENTIVE AND SOCIAL MEDICINE (PSM) EXAMINATION 🏆🔥!!!!!!!!!!! #PREVENTIVE AND SOCIAL MEDICINE (PSM) 🏆🔥!!!!!!!!!!! #MBBS 🏆🔥!!!!!!!!!!!#CONCISE ANSWERS FOR EACH AND EVERY TOPIC THAT I WILL PROVIDE IN THE FUTURE TEXTS/UPCOMING TEXTS/SUBSEQUENT TEXTS 🏆🔥!!!!!!!!!!! #FULL MARKS (100%) IN MY UPCOMING MBBS PREVENTIVE AND SOCIAL MEDICINE (PSM) EXAMINATION 🏆🔥!!!!!!!!!!! #PREVENTIVE AND SOCIAL MEDICINE (PSM) 🏆🔥!!!!!!!!!!! #MBBS 🏆🔥!!!!!!!!!!!#CONCISE ANSWERS FOR EACH AND EVERY TOPIC THAT I WILL PROVIDE IN THE FUTURE TEXTS/UPCOMING TEXTS/SUBSEQUENT TEXTS 🏆🔥!!!!!!!!!!! #FULL MARKS (100%) IN MY UPCOMING MBBS PREVENTIVE AND SOCIAL MEDICINE (PSM) EXAMINATION 🏆🔥!!!!!!!!!!! #PREVENTIVE AND SOCIAL MEDICINE (PSM) 🏆🔥!!!!!!!!!!! #MBBS 🏆🔥!!!!!!!!!!!
- Bullet-point format for quick revision
- Key definitions, classifications, and mnemonics
- Important numbers/values highlighted
- Exam-relevant points emphasized
Steps in the investigation of an epidemic
Steps in the Investigation of an Epidemic
Objectives of Epidemic Investigation (remember: DICE + R)
- Define magnitude in terms of time, place, person
- Identify cause, source of infection, mode of transmission
- Conditions and factors responsible for the epidemic
- Establish control measures
- Recommend prevention of recurrence
Steps (10 Steps - Mnemonic: "Very Clever Dogs Race Past Six Big Orange Trees Rapidly")
Step 1 - Verification of Diagnosis
- Confirm the diagnosis on the spot immediately
- Clinical examination of a sample of cases suffices (not all)
- Laboratory investigations confirm diagnosis - but do NOT delay epidemiological investigation waiting for lab results
- Rule out spurious reports (misinterpretation by laypublic)
Step 2 - Confirmation of Existence of an Epidemic
- Compare current disease frequency with same period in previous years
- Epidemic exists when observed frequency > expected frequency for that population
- Arbitrary limit: 2 standard errors above endemic occurrence = epidemic threshold (e.g., influenza)
- Common-source epidemics (cholera, food poisoning, Hep A) are easily recognized - no comparison needed
- Modern epidemics (cancer, CVD) are not easily recognized
Step 3 - Defining the Population at Risk
- (a) Obtain a map of the area - note landmarks, roads, dwelling units (numbered)
- (b) Count the population - house-to-house census by age and sex
- Lay health workers used
- Needed to compute attack rates in various subgroups
- No denominator = no attack rate calculation
Step 4 - Rapid Search for All Cases and Their Characteristics
- (a) Medical survey - identify ALL cases including those not seeking care; administer epidemiological case sheet
- (b) Epidemiological case sheet (Case Interview Form) - collects:
- Name, age, sex, occupation, social class
- Time of onset, signs and symptoms
- Travel, previous exposure, personal contacts (home, work, school)
- Special events (parties, foods eaten, common vehicles - water/food/milk)
- Blood products, injections, large gatherings attended
- (c) Searching for more cases - ask index case about others with similar illness in home, neighbourhood, school, workplace within the incubation period; check local hospital admissions
- If outbreak is large → examine a random sample
Step 5 - Data Analysis (Characterize by Time, Place, Person)
- Plot an epidemic curve (X-axis = time of onset; Y-axis = number of cases)
- Determines: type of epidemic, incubation period, likely exposure time
- Point source = single sharp peak
- Propagated = series of peaks at intervals of ~1 incubation period
- Prepare a spot map (dot map) - each dot = one case at address
- Identifies geographic clustering and clues about source/mode of spread
- Compute attack rates by age, sex, occupation, etc.
- Identify high-risk groups to focus control measures
- Formula: Attack Rate = (Number of new cases / Population at risk) × 100
Step 6 - Formulation of Hypotheses
- Based on analysis of time, place, person data
- Hypothesize:
- Probable source of infection
- Probable mode of transmission
- Probable causative agent
- Should explain the majority of cases
Step 7 - Testing of Hypotheses
- Use analytical epidemiology - case-control or cohort study
- Case-control study most commonly used in food-borne outbreaks
- Compare food histories of cases vs. controls
- Calculate odds ratios or relative risks
- Statistical tests applied (chi-square, etc.)
- Hypothesis accepted if statistically significant
Step 8 - Instituting Control Measures
- Should not wait until investigation is complete - begin as soon as probable source/mode is identified
- Directed at:
- Agent - treatment, disinfection
- Host - vaccination, chemoprophylaxis
- Environment - water purification, food safety, sanitation
- This is the primary purpose of epidemic investigation
Step 9 - Writing a Report
- Document all findings systematically
- Include: background, methods, results, discussion, conclusions, recommendations
- Serves as a permanent record and guides future action
- Helps in legal matters if required (food poisoning, compensation)
Step 10 - Recommendations for Prevention of Recurrence
- Based on identified cause and contributing factors
- Long-term measures: improved sanitation, water supply, immunization programs, health education
- Submitted to health authorities
Key Points to Remember for Exam
| Feature | Detail |
|---|---|
| First step | Verification of diagnosis |
| Epidemic threshold | 2 SD above endemic level |
| Epidemic curve | Determines type + incubation period |
| Spot map | Shows geographic distribution |
| Attack rate = | (Cases / Population at risk) × 100 |
| Most used analytical study | Case-control study |
| Control measures | Do NOT wait - start early |
| Common source epidemic curve | Single sharp peak |
| Propagated epidemic curve | Multiple peaks |
Source: Park's Textbook of Preventive and Social Medicine - the gold standard for PSM (MBBS)
Case control study
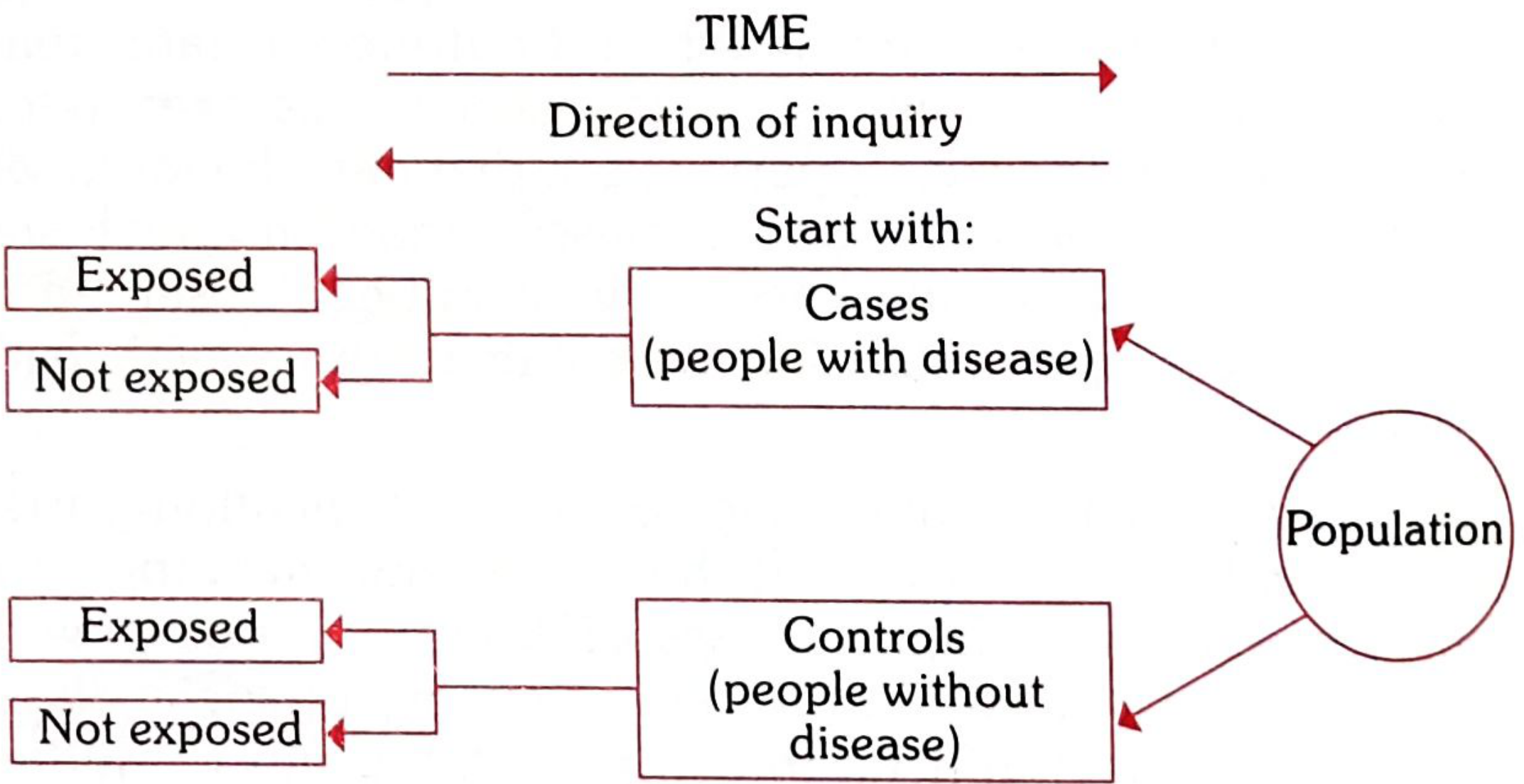
Case-Control Study
Definition
3 Distinct Features (Must Know)
- Both exposure and outcome (disease) have already occurred before the start of the study
- Study proceeds backwards - from effect → cause
- Uses a control/comparison group to support or refute an inference
Design Diagram
The 2×2 Contingency Table (Framework)
| Suspected Risk Factor | Cases (Disease present) | Controls (Disease absent) |
|---|---|---|
| Present | a | b |
| Absent | c | d |
| Total | a+c | b+d |
- Exposure rate in cases = a/(a+c)
- Exposure rate in controls = b/(b+d)
- If exposure rate in cases > controls → association exists
Measure of Association: ODDS RATIO (OR)
Odds Ratio = (a × d) / (b × c)
- OR = 1 → No association
- OR > 1 → Positive association (risk factor)
- OR < 1 → Negative association (protective factor)
- In case-control studies: cannot calculate Relative Risk directly - only estimate it via Odds Ratio
- OR is a good approximation of RR when disease is rare (rare disease assumption)
Classic Example (Smoking & Lung Cancer):
| Lung Cancer (Cases) | Controls | Total | |
|---|---|---|---|
| Smokers | 33 (a) | 55 (b) | 88 |
| Non-smokers | 2 (c) | 27 (d) | 29 |
| Total | 35 | 82 | - |
- Exposure rate in cases = 33/35 = 94.2%
- Exposure rate in controls = 55/82 = 67.0%
- P < 0.001 (statistically significant)
4 Basic Steps in Conducting a Case-Control Study
Step 1 - Selection of Cases and Controls
- Diagnostic criteria - must be defined before study (e.g., histologically confirmed cancer stage)
- Eligibility criteria - preferably newly diagnosed (incident) cases, not prevalent cases
- Sources: (i) Hospitals (single or network), (ii) General population
- Must be comparable to cases in known confounding factors (age, sex, occupation, social class)
- Sources:
- Hospital controls (admitted for unrelated conditions)
- General population controls
- Relatives/neighbors (neighborhood controls)
- Dead controls (from death certificates)
- Controls must be free from the disease under study
- Ratio: usually 1 case : 1 control (can go up to 1:4 to increase statistical power)
Step 2 - Matching
- Process of making cases and controls comparable with respect to confounding variables
- Types of matching:
- Individual matching (Pair matching) - each case matched to one or more controls for specific characteristics
- Group matching (Frequency matching) - controls selected so the overall distribution of confounders is similar
- Variables commonly matched: age, sex, race, occupation, socioeconomic status
- Overmatching (matching on too many variables) reduces efficiency
Step 3 - Measurement of Exposure
- Information collected about past exposure to suspected risk factors
- Methods:
- Interviews / questionnaires
- Medical records
- Biological specimens
- Data collected on: diet, smoking, occupational exposure, medications, family history, etc.
Step 4 - Analysis and Interpretation
- (a) Exposure rates - compare frequency of exposure in cases vs. controls
- (b) Odds Ratio - estimate of disease risk associated with exposure
- Statistical test: Chi-square test (for discrete variables); p ≤ 0.05 = statistically significant
- Statistical significance ≠ causation
Sources of Bias in Case-Control Studies
| Bias | Description |
|---|---|
| Recall (Memory) bias | Cases remember past exposures better than controls |
| Selection bias | Cases/controls not representative of general population |
| Berkesonian bias | Different hospital admission rates for different diseases (hospital-based studies) |
| Interviewer bias | Interviewer questions cases more thoroughly if aware of hypothesis - eliminated by double-blinding |
| Confounding bias | Third variable distorts the association - controlled by matching |
Advantages vs Disadvantages
| Advantages | Disadvantages |
|---|---|
| Relatively easy to carry out | Subject to recall bias |
| Rapid and inexpensive (vs. cohort) | Selection of controls is difficult |
| Requires few subjects | Cannot measure incidence directly |
| Ideal for rare diseases | Can only estimate relative risk (via OR) |
| No follow-up required (no attrition) | Cannot distinguish cause from associated factors |
| Can study multiple etiological factors simultaneously | Not suitable for evaluating therapy or prophylaxis |
| No risk to subjects | Representativeness of cases/controls may be questionable |
| Minimal ethical problems |
Key Comparisons to Remember
| Feature | Case-Control | Cohort |
|---|---|---|
| Direction | Backward (effect → cause) | Forward (cause → effect) |
| Starts with | Disease status | Exposure status |
| Also called | Retrospective | Prospective |
| Measure | Odds Ratio | Relative Risk |
| Best for | Rare diseases | Rare exposures |
| Time | Short | Long |
| Cost | Cheap | Expensive |
| Incidence | Cannot calculate | Can calculate |
High-Yield Exam Points
- Case-control = retrospective study
- Proceeds backwards: effect → cause
- Measure of association = Odds Ratio (OR) = ad/bc
- OR approximates RR when disease is rare
- Most common bias = recall/memory bias
- Berkesonian bias = unique to hospital-based case-control studies
- Best for: rare diseases, chronic diseases, multiple risk factor analysis
- Cannot measure incidence rates
Source: Park's Textbook of Preventive and Social Medicine